
Abstract
Paraduodenal pancreatitis (PP) is a rare type of focal pancreatitis involving the groove space. It mimics pancreatic head carcinoma, and its diagnosis and treatment are challenging. Pancreatoduodenectomy (PD) has traditionally been the primary surgical treatment for duodenal stenosis or suspected cancer.
We herein report a case of PP in a 65-year-old man. The patient was admitted to the hospital for postprandial epigastric pain and vomiting. A low-density mass between the uncinate process of the pancreas and the horizontal segment of the duodenum was suspected based on computed tomography findings. Both upper gastrointestinal radiography and gastrointestinal endoscopy showed an obstruction of the distal part of the descending duodenum. An operation was performed to release the obstruction and obtain a definitive diagnosis. A 3-cm mass in the groove area was compressing the third part of the duodenum, and PD was empirically performed. The final histopathological diagnosis was PP. Postoperatively, the patient developed anastomotic leakage of the gastrojejunostomy site with bleeding and was eventually discharged on postoperative day 51 after emergency surgery.
PP should be considered as a differential diagnosis of pancreatic ductal adenocarcinoma or duodenal stenosis, and accurate preoperative diagnosis preserves the opportunity for conservative or endoscopic management.
Keywords
Introduction
The pancreatoduodenal groove (anatomical groove) is a potential area bordered by the head of the pancreas, duodenum, and common bile duct. Paraduodenal pancreatitis (PP) is a very rare subtype of chronic pancreatitis that masks or coexists with pancreatic ductal adenocarcinoma. It usually manifests in middle-aged men with heavy drinking or smoking habits.1,2 The principal manifestation is always non-typical, including symptoms such as upper abdominal pain, postprandial nausea, and vomiting, mimicking pancreatic head carcinoma. Considering the low incidence of PP,3–6 the similarity of clinical symptoms with those of pancreatic head carcinoma, and the variability of biopsy findings depending on the area sampled, achievement of an accurate preoperative diagnosis is difficult. Pancreaticoduodenectomy (PD) is the foremost surgical approach to the treatment of PP with duodenal obstruction or suspected malignancy. We herein report a case of PP that was diagnosed after surgery. The patient developed and recovered from severe postoperative complications. This case reminds us of the importance of early diagnosis to avoid an unnecessary radical operation.
Case presentation
A 65-year-old man was admitted to the hospital with a 2-month history of postprandial epigastric pain and 4-day history of vomiting. He had no history of nicotine or alcohol abuse. He also denied a history of hypertension, diabetes, a family history of cancer, and prior surgery. The physical examination revealed no noteworthy findings except slight upper abdominal pain on application of pressure. Laboratory data showed the following abnormalities: white blood cell count of 10.12 × 1012/L [reference range (RR), 4.0–9.0 × 1012/L], neutrophilic granulocyte percentage of 0.81 (RR, 0.5–0.7), blood amylase concentration of 144 U/L (RR, 40–110 U/L), urine amylase concentration of 990 U/L (RR, 100–330 U/L), and D-dimer concentration of 360 µg/L (RR, <200 µg/L). The CA19-9, CA125, and carcinoembryonic antigen concentrations were within normal limits. Nothing abnormal was identified in the liver function, whole immunoglobulins, or immunoglobulin G4.
Triple-phase contrast computed tomography of the abdomen showed a low-density mass between the sulcus of the pancreas and horizontal part of the duodenum (Figure 1). During the upper gastrointestinal radiographic examination, the contrast medium entered the horizontal duodenum extremely slowly. Furthermore, gastrointestinal endoscopy revealed obstruction of the distal part of the descending duodenum combined with mucous hyperemia (Figure 2). Endosonography showed no focal lesion; only a thickened duodenal wall was evident. Ultrasound showed an enlarged gallbladder with a moderately dilated common bile duct.

(a) A delayed-phase contrast-enhanced computed tomography image demonstrated a low-density mass (arrows). (b) A reconstructed coronal computed tomography image showed an ill-defined, irregularly shaped, heterogeneous mass (arrows) in the pancreatic uncinate process, and the duodenum was dilated secondary to obstruction of the distal part of the descending duodenum.

(a) Contrast medium slowly passed through the horizontal duodenum during upper gastrointestinal radiography. (b) The gastroscope revealed obstruction of the distal part of the descending duodenum with mucosal hyperemia.
The clinical evaluation revealed duodenal stenosis, and pancreatic uncinate carcinoma was suspected. Because of the diagnostic uncertainty, a multidisciplinary team meeting was arranged. Despite the lack of definitive evidence of malignancy, the duodenal obstruction was obvious, and we intended to relieve the obstruction and achieve a definitive diagnosis. An operation was performed, followed by gastrointestinal decompression and intravenous nutrition for 7 days. Surgical exploration revealed obvious edema of the gastric wall as well as contracture and edema of the third part of the duodenal wall. The bowel lumen was exceedingly narrow. A 2.5- × 2.0-cm hard mass was located in the uncinate process of the pancreas, compressing the horizontal part of the duodenum and adhering to the mesenteric root. The peripancreatic lymph node was hard and enlarged and thus highly suspicious of malignancy. Radical PD (Whipple procedure with pancreatic-jejunal anastomosis) was carried out to relieve the obstruction, thoroughly remove the pancreatic lesions, and dissect the surrounding lymph nodes. Postoperative pathologic examination of the specimens showed thrombosis with thrombus organization accompanied by fibrous tissue hyperplasia between the pancreas and duodenum with chronic inflammatory changes. A thickened duodenal wall and submucosal fibrosis were also found. Pancreatic ectopic tissue with localized inflammation and scarring in the duodenal wall was evident. The lymph node showed reactive hyperplasia (Figure 3).
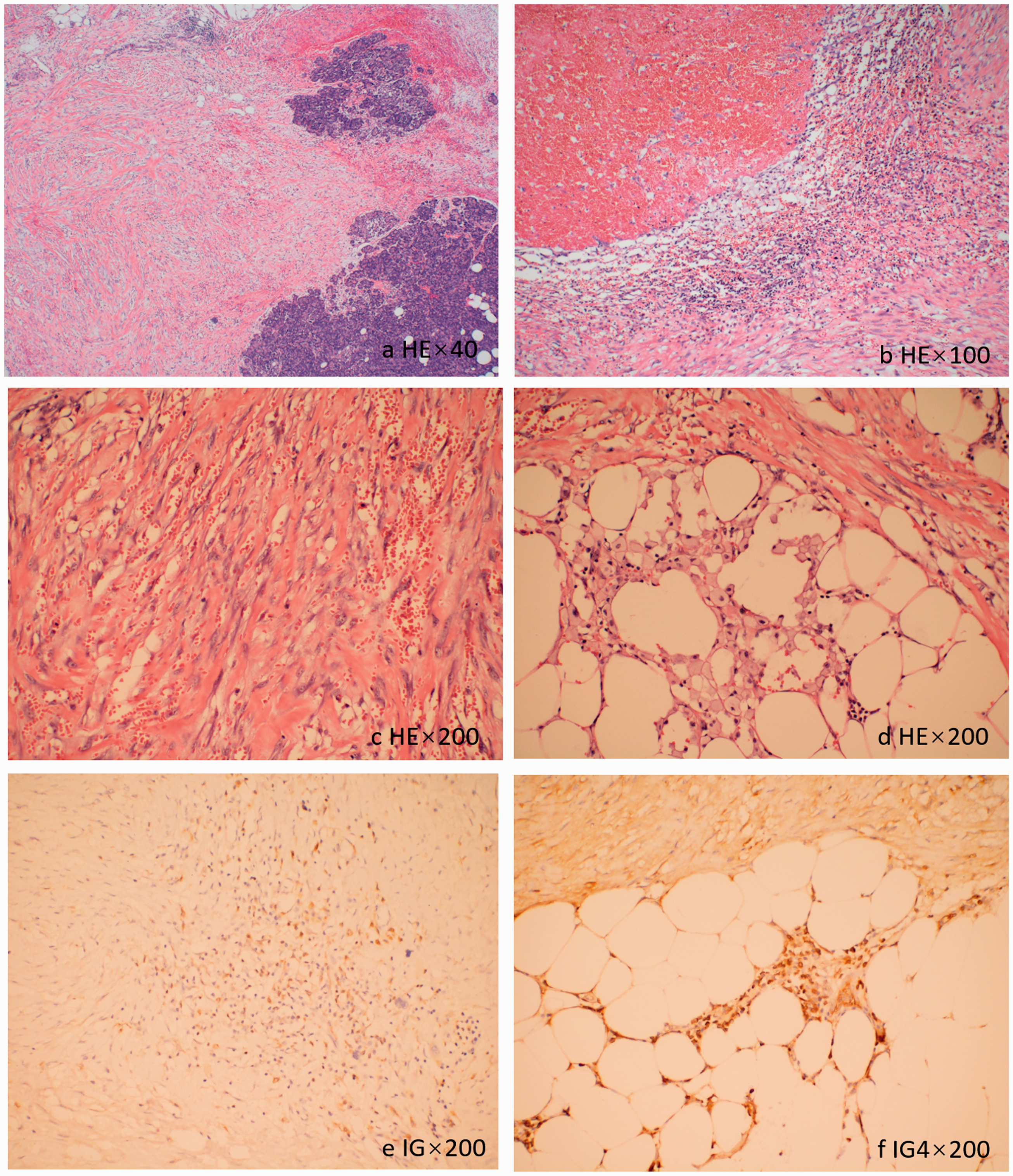
Histopathological examination showed (a) fibrous proliferation and chronic inflammation between the pancreas and duodenum with chronic inflammatory infiltration as well as (b) thrombosis with venous thrombus organization. The duodenal wall was thickened, and submucosal fibrosis was found. (c, d) Ectopic pancreatic tissue was evident in the duodenal wall with localized inflammation and scarring, and (e, f) whole immunoglobulin and immunoglobulin G4 staining was negative.
On postoperative day 5, the patient developed a fever and leukocytosis, and Doppler ultrasound revealed fluid in the gallbladder fossa. On postoperative day 6, fresh blood began draining from the abdominal and gastric tubes, and brown liquid gushed out of the incision. The patient immediately underwent an emergency operation. After removing the blood from the stomach and abdominal cavity, a 2-cm-long rupture of the gastrointestinal anastomosis was found. Adequate drainage was performed after repairing the rupture. The patient recovered slowly and was discharged on postoperative day 51.
Discussion
PP is a rare form of chronic focal pancreatitis 7 that affects the pancreatic duodenal groove space. The reported incidence of PP varies significantly,3–6 and it reportedly accounts for only 2% of cases of chronic pancreatitis after PD. 8 PP can be caused by anatomical obstruction in the minor papilla, by heavy smoking, or by alcohol toxicity-induced abnormal papillary function. Patients with PP generally present with abdominal pain coupled with nausea and postprandial vomiting. Slight elevations in pancreatic and hepatic enzymes can be found in the acute period. The CA19-9 and carcinoembryonic antigen concentrations are usually normal or slightly raised. 9 The patient in the present case had similar symptoms and laboratory findings with the exception of heavy smoking or drinking.
The inflammation or fibrosis of PP can result in a pseudotumor mimicking local pancreatic carcinoma. Nearly 60% of cases of PP with a solid variant appearance have been preoperatively diagnosed as cancer.10,11 A multidisciplinary team meeting can facilitate the diagnosis of pancreatic disease. PP should be considered as a differential diagnosis of pancreatic masses or duodenal stenosis. Although both computed tomography and magnetic resonance imaging have been proven useful, fine needle aspiration is the most accurate and reliable way to differentiate and diagnose pancreatic masses. However, definitive diagnosis is sometimes complicated because the mucosal and submucosal features are often subtle and not specific to PP. Fine needle aspiration is not helpful to rule out cancer because of its negative results. 12
The initial therapeutic approaches in patients with PP may include alcohol withdrawal, abstinence of tobacco, pancreatic rest, analgesics, and eventually somatostatin. Endoscopic treatment should be proposed in nonresponders. 13 A surgical procedure should be preferentially selected only in patients with suspected malignancy, intractable pain or severe duodenal stenosis, or failure to respond to repeated endotherapy.1,2 PD is the usual preliminary choice because it allows for a definitive tissue diagnosis, resolution of pain, and prevention of recurrence. Considering the mortality rate of PD (2%–3%), 14 various less invasive therapies are likewise effective for patients with less severe symptoms. In a review of 138 patients, more than half of patients who received conservative or endoscopic treatment achieved full symptom relief. 15 Preoperative pathologic findings may contribute to exclusion of malignancy and allow for performance of a more conservative procedure.
Preoperative diagnosis of PP is challenging; however, the intraoperative biopsy may help to avoid a more invasive operation. In this case, we failed to obtain a pathological result before radical PD because of the special anatomical location of the mass. Additionally, because it appeared to be a tumor during the operation, PD was performed based on our experience. After 7 days of gastrointestinal decompression, intraoperative edema was still encountered. Delayed anastomotic leakage at the gastrojejunostomy site with bleeding then occurred Although there were enough reasons to perform PD in this case, PD should be carefully and selectively performed with consideration of the potential complications and adverse outcomes.
Conclusion
PP presents a unique diagnostic challenge. Surgical resection is often required to achieve a definitive diagnosis. PD allows successful management of refractory symptoms, and definitive surgical resection eliminates diagnostic uncertainty in most patients with PP. Given the morbidity and complications connected with PD, accurate preoperative diagnosis preserves the opportunity for less invasive means of treatment.
Footnotes
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Authors’ contributions
MW contributed to the data collection and analysis. CJ contributed to the data analysis and interpretation and drafting of the manuscript. X-Y L contributed to the data interpretation and critical revision of the manuscript for important intellectual content. W-K Y contributed to the pathological results.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics approval and consent to participate
This article was approved by the Ethics Committee of the First Hospital of Jilin University. Informed consent was collected (according to the World Medical Association Declaration of Helsinki) at the First Hospital of Jilin University. The study was approved by the Institutional Review Board at the First Hospital of Jilin University. Written informed consent was provided by the patient for publication of this report and any accompanying images.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the China Scholarship Council (201906175060) and the Teaching Reform Fund of Standardized Training of Residents from the First Hospital of Jilin University (2018015).