
Abstract
Objective
Activated platelets release serotonin, causing platelet aggregation and vasoconstriction. Serotonin levels were investigated in patients with acute coronary syndrome (ACS) and chronic stable angina (CSA) treated with percutaneous coronary intervention (PCI).
Methods
Consecutive patients undergoing PCI for either ACS or CSA were enrolled between July 2009 and April 2010. Patients were pre-treated with dual antiplatelet agents (aspirin and clopidogrel) before PCI. Serum serotonin levels, measured at baseline, pre- and post-PCI, and at 90 min, and 6, 12, 24 and 48 h following PCI, were compared between ACS and CSA groups.
Results
Sixty-three patients with ACS and 60 with CSA were included. Overall baseline characteristics were similar between the two groups. Serotonin levels at post-PCI (55.2 ± 120.0 versus 20.1 ± 24.0) and at peak (regardless of timepoint; 94.0 ± 170.9 versus 38.8 ± 72.3) were significantly higher in the ACS versus CSA group. At 90 min and 6, 24 and 48 h post-PCI, serum serotonin was numerically, but not significantly, higher in patients with ACS. Serotonin levels fluctuated in both groups, showing an initial rise and fall, rebound at 24 h and drop at 48 h post-PCI.
Conclusions
In patients undergoing PCI, serum serotonin was more elevated in patients with ACS than those with CSA, suggesting the need for more potent and sustained platelet inhibition, particularly in patients with ACS.
Introduction
Serotonin (5-hydroxytryptamine [5HT]) is present in abundance in various cardiac tissues including platelets, and its receptor is detected on the surface of platelets.1 In turn, 5HT released from activated platelets induces the aggregation of platelets and vasoconstriction.2–4 During platelet activation and aggregation, 5HT is further released, facilitating the formation of an occlusive thrombus.5 Platelet adhesion and aggregation in ruptured plaques, leading to thrombotic coronary occlusion, are considered to be key mechanisms causing acute myocardial infarction.6,7 Percutaneous coronary intervention (PCI) is the standard treatment for a wide spectrum of ischaemic heart diseases, including acute coronary syndrome (ACS) and chronic stable angina (CSA).8–10 However, PCI with either balloon angioplasty only or with stent placement may cause barotrauma to the surface of the atherosclerotic plaque, with subsequent complications, such as intimal injury or dissection, further leading to platelet activation and aggregation, which mimic the features of ACS.11 On the basis of this phenomenon and evidence from previous clinical trials, antiplatelet pretreatment with aspirin and P2Y12 receptor inhibitors has become the standard of care in patients undergoing PCI.8,12
Although 5HT has also been related to the pathogenesis of acute myocardial infarction, no study has investigated serial changes in serotonin as a clinical biomarker.13 In addition, there have been few reports on changes in serum serotonin levels before and after PCI in patients with stable coronary artery disease.14,15 Moreover, in patients with ACS, changes in serum serotonin have not been investigated. Therefore, in the present study, serum serotonin levels were serially measured in patients with ACS or CSA undergoing PCI. The primary objective of the present study was to determine and compare changes in serum serotonin levels in patients with ACS or CSA undergoing PCI who were pretreated with a conventional dual antiplatelet loading regimen (aspirin 300 mg and clopidogrel 600 mg).
Patients and methods
Study population
In this prospective observational study, patients undergoing PCI at Hallym University Kangnam Sacred Heart Hospital for either ACS or CSA were enrolled between July 2009 and April 2010, and serial measurements of serum serotonin were obtained at baseline; pre-PCI; post-PCI; and 90 min, 6 h, 12 h, 24 h, and 48 h after PCI. Patients were categorized into two groups, ACS or CSA, according to the American College of Cardiology/American Heart Association guidelines.12,16 The ACS group included patients with acute ST-segment elevation myocardial infarction (STEMI), non-STEMI, and unstable angina. The CSA group included patients with chronic stable coronary disease with objective ischaemia. Those with (1) known allergies to aspirin, prasugrel, ticagrelor, or clopidogrel; (2) oral anticoagulant therapy (vitamin K antagonists, dabigatran, apixaban, rivaroxaban); (3) blood dyscrasia or bleeding diathesis; (4) platelet count < 80 × 106/ml; (5) haemoglobin < 10 g/dl; (6) active bleeding or haemodynamic instability; (7) creatinine clearance < 30 ml/min; and/or (8) a pregnant status (in women) were excluded. Patients’ records were reviewed for potential exclusion from the final analyses.
The study was approved by the Institutional Review Board of Hallym University Kangnam Sacred Heart Hospital (approval No. 2019-07-002) and was performed in accordance with the tenets of the Declaration of Helsinki. Serial measurements of cardiac biomarkers were performed in all patients undergoing PCI at Hallym University Kangnam Sacred Heart Hospital, as part of routine clinical practice. Verbal informed consent for serotonin measurements was obtained for each patient included in the present study.
Antiplatelet agents and serum serotonin measurement
All patients who had not previously received any antiplatelet agents were administered 300 mg aspirin and 600 mg clopidogrel as loading doses before PCI. Patients who had previously taken aspirin received 600 mg clopidogrel before PCI. Likewise, patients who had already received clopidogrel took 300 mg aspirin before PCI. From the day after the loading doses of aspirin and clopidogrel, maintenance doses of 100 mg aspirin and 75 mg clopidogrel, once daily, were administered in all patients as standard care. No antiplatelet (including selective 5HT antagonist) or antithrombotic agents other than aspirin and clopidogrel were given to the patients during the study period.
Blood samples (5 ml) were obtained by venepuncture at specified time-points (baseline; pre-PCI; post-PCI; and 90 min, 6 h, 12 h, 24 h, and 48 h after PCI). The baseline sample was obtained immediately on admission or emergency room visit, and the pre-PCI sample was obtained after antiplatelet administration in the cardiac catheterization laboratory before performing PCI. Blood samples were allowed to clot for 30 min, then centrifuged for 15 min at 5 000×g to obtain serum. Serum serotonin levels were serially measured using a ClinRep® HPLC kit (Recipe Chemicals and Instruments GmbH, Munchen, Germany) according to the manufacturer’s instructions. Creatinine-kinase MB, troponin-I, and troponin-T levels were also obtained as part of routine clinical care. Mean peak serotonin levels following PCI (regardless of timepoint) were calculated and compared between groups.
Statistical analyses
Because of a lack of previous studies, no sample size calculation was performed. Data are presented as mean ± SD or n (%). Differences between the ACS and CSA groups were analysed using Student’s t-test, and changes over time were compared using analysis of covariance. Categorical variables were analysed using χ2-test and Fisher’s exact test. Logistic regression analysis was performed using baseline serum serotonin levels to assess the screening ability for ACS or CSA. Statistical analyses were performed using R programming, version 3.6.0 (The R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org). A two-sided P value < 0.05 was considered statistically significant.
Results
Baseline characteristics
A total of 127 patients who underwent PCI for either ACS or CSA and had serial measurements of serum serotonin were initially included. Following a review of patients’ records, three patients with variant angina or acute myocardial infarction due to spasm, and one patient with outlier values were excluded. Thus, a total of 123 patients were included in the final analysis (Figure 1), comprising 63 patients assigned to the ACS group (STEMI, n = 25; non-STEMI n = 20; and unstable angina, n = 18; Figure 2) and 60 patients assigned to the CSA group. According to past medical history, no patients received selective serotonin reuptake inhibitors (SSRIs) as an antidepressant. The overall baseline characteristics were similar between the two groups (Table 1). However, the proportion of never-smokers was higher in the CSA group (61.7% versus 38.1%, P = 0.006) and the proportion of current smokers was higher in the ACS group (42.9% versus 18.3%, P = 0.003). Angiotensin-converting enzyme (ACE) inhibitors and beta-blockers were more often prescribed in the ACS group (ACE inhibitors: 65.1% versus 41.7%, P = 0.013; beta-blockers: 74.6% versus 45.0%, P = 0.008; Table 1). Conversely, calcium channel blockers and statins were more frequently prescribed in the CSA group (calcium channel blockers: 31.7% versus 11.1%, P = 0.009; statins: 73.3% versus 47.6%, P = 0.002; Table 1). Triglyceride levels were higher in the CSA group than in the ACS group (156.2 ± 122.6 versus 112.1 ± 73.4; P = 0.021).
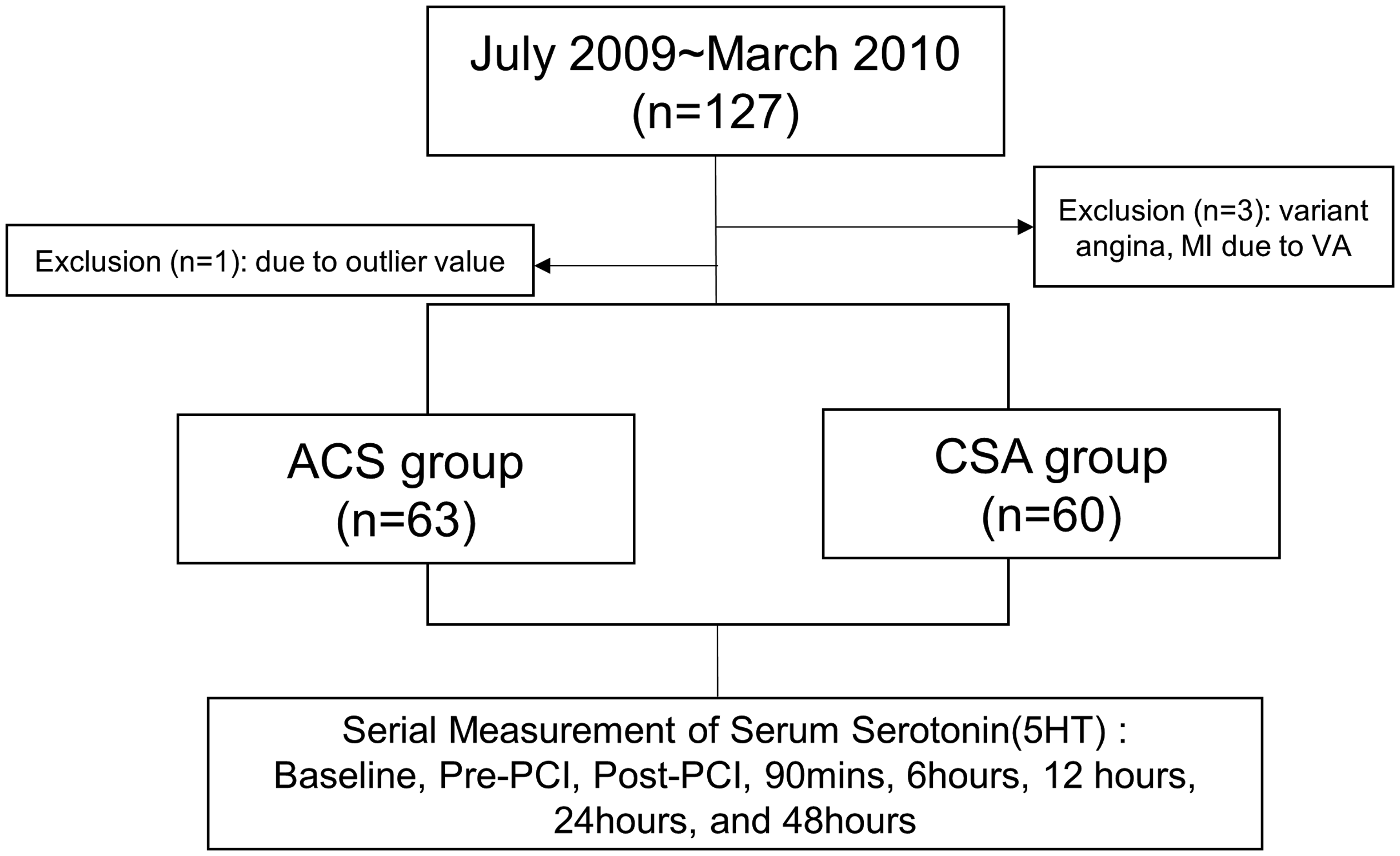
Study flow chart of patient selection. ACS, acute coronary syndrome; CSA, chronic stable angina; MI, myocardial infarction; PCI, percutaneous coronary intervention; VA, variant angina.

Pie chart showing the proportion of patients with ST-segment elevation myocardial infarction (STEMI), non-STEMI (NSTEMI), or unstable angina (UA) in the acute coronary syndrome (ACS) group.
Baseline demographic and clinical characteristics.

Data presented as mean ± SD or n (%).
ACEi, angiotensin converting enzyme inhibitor; ACS, acute coronary syndrome; ARB, angiotensin receptor blocker; BMI, body mass index; BUN, blood urea nitrogen; CCB, calcium channel blocker; CKD, chronic kidney disease; CSA, chronic stable angina; CVA, cerebrovascular accident; LDL-cholesterol, low density lipoprotein cholesterol.
NS, no statistically significant between-group difference (P > 0.05; Student’s t-test, χ2-test or Fisher’s exact test).
Serial serum serotonin measurement
Serum serotonin levels were serially measured at baseline, pre-PCI, post-PCI, and at 90 min, 6 h, 12 h, 24 h, and 48 h after PCI. Serum serotonin showed no statistically significant difference between the CSA group and ACS group at baseline (10.3 ± 15.9 ng/ml versus 8.6 ± 14.6 ng/ml; P = 0.717) and pre-PCI (19.7 ± 47.8 ng/ml versus 18.3 ± 30.7; P = 0.840; Table 2 and Figure 3). At the post-PCI time-point, serum serotonin was higher in the ACS group compared with the CSA group (55.2 ± 120.0 versus 20.1 ± 24.0 ng/ml, P = 0.034) (Table 2). The first peak serum serotonin level was reached post-PCI in the ACS group, whereas the first peak level was reached at 90 min after PCI in the CSA group (Figure 3). The time-point when serum serotonin returned to the lowest level after the initial peak was 6 h in the ACS group, whereas it was delayed to 12 h in the CSA group. In both groups, serum serotonin rebounded and reached the second peak at 24 h after PCI, and then decreased at 48 h post-PCI (Figure 3). All serum serotonin measurements were numerically more increased in the ACS group than the CSA group following PCI, however, the difference was only statistically significant at the post-PCI time-point (P = 0.034; Figure 3 and Table 2).
Comparison of serial serotonin values between patients with chronic stable angina (CSA) and patients with acute coronary syndrome (ACS) who underwent percutaneous coronary intervention (PCI).
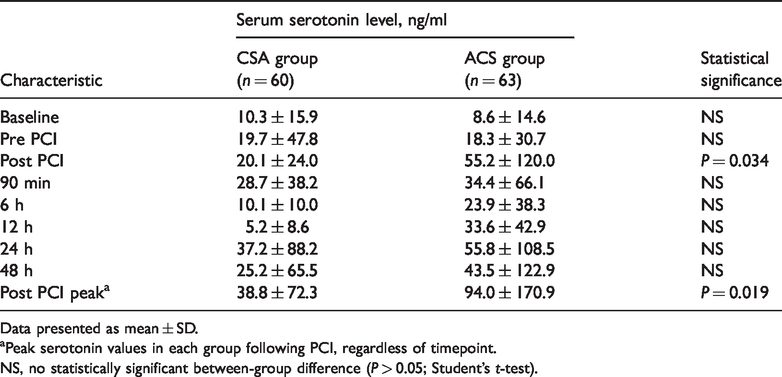
Data presented as mean ± SD.
aPeak serotonin values in each group following PCI, regardless of timepoint.
NS, no statistically significant between-group difference (P > 0.05; Student’s t-test).
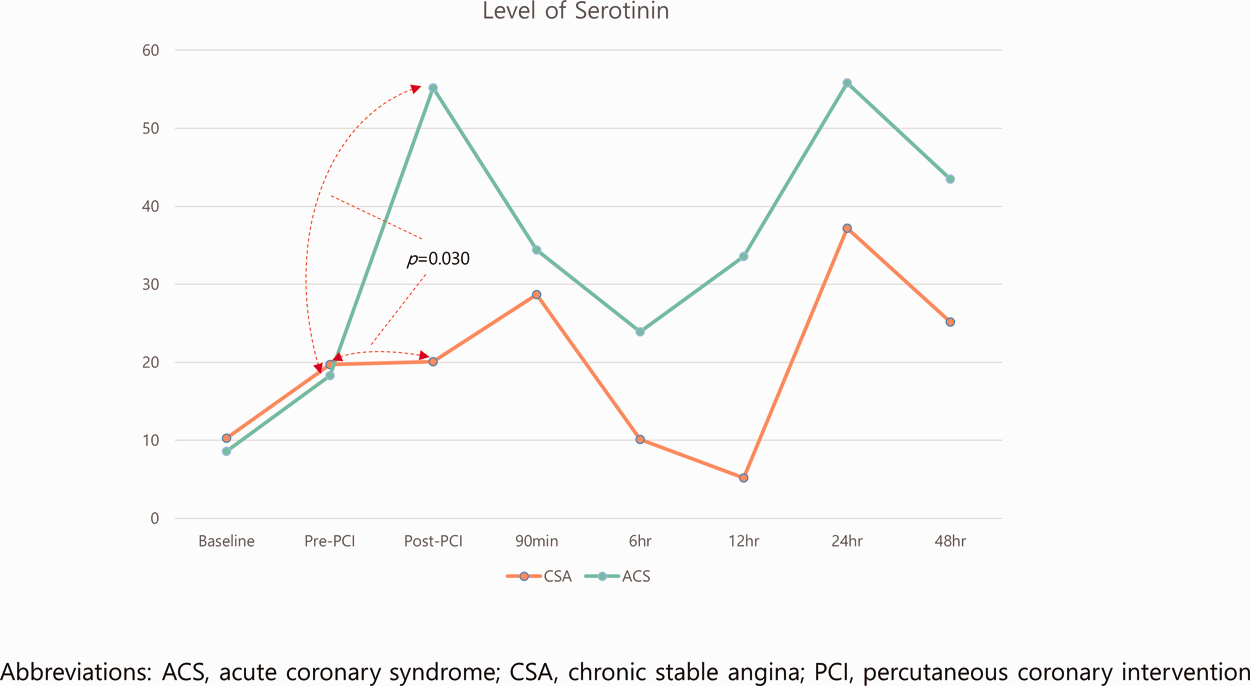
Serial changes in serum serotonin level over time between patients with acute coronary syndrome (ACS) or chronic stable angina (CSA) who underwent percutaneous coronary intervention (PCI).
Although there was no difference in the baseline serotonin level between the two groups (P = 0.717, Figure 3 and Table 2), within-group differences between baseline and peak levels showed statistical significance in both groups (ACS, P < 0.001; CSA, P = 0.003; Figure 3). However, the degrees of change did not show a significant difference between the two groups (P = 0.09). Differences in serum serotonin level between pre-PCI and post-PCI were statistically significant in the ACS group (18.3 ± 30.7 versus 55.2 ± 120 ng/ml; P = 0.027), but not in the CSA group (19.7 ± 47.8 versus 20.1 ± 24 ng/ml, P = 0.088). Between-group comparison of change in serum serotonin from pre- to post-PCI showed that the increase was significantly higher in the ACS group than in the CSA group (arrow in Figure 3, P = 0.030).
Peak serotonin levels following PCI (regardless of timepoint) were significantly higher in the ACS group (94.0 ± 170.9) versus the CSA group (38.8 ± 72.3; P = 0.019; Table 2).
Serum serotonin as a screening biomarker
The ability of baseline serum serotonin levels to distinguish patients with ACS from those with CSA were analysed in the two groups using logistic regression, however, there was no statistically significant association was observed (P = 0.692; Figure 4A). Logistic regression analyses of serum serotonin levels at the post-PCI time-point showed a positive relationship with ACS, with the ACS group showing a greater increase in platelet reactivity than the CSA group (P = 0.028; Figure 4B).

Logistic regression analyses of the correlation between serum serotonin levels and diagnosis of acute coronary syndrome (ACS) in patients with ACS or chronic stable angina (CSA) who underwent percutaneous coronary intervention (PCI): (A) at baseline and (B) at post-PCI period.
Discussion
The present study had several key findings: (1) the change in serum 5HT levels was greater and faster in patients with ACS than those with CSA; (2) the ACS group showed earlier initial peak and dip in serum serotonin following PCI than the CSA group; (3) serum serotonin reached a second peak at 24 h and showed a dip at 48 h following PCI in both groups; and (4) baseline serum serotonin levels could not be used to distinguish ACS from CSA.
Serotonin (5HT) affects platelet activation, aggregation, and thrombosis.2,3,17 5HT is also known to play an important role in the pathogenesis of cardiovascular diseases, such as systemic hypertension, pulmonary hypertension, and coronary artery disease, by inducing vasoconstriction.3,18–20 Particularly in patients with hypertension, the biological profile of platelets becomes abnormal, which leads to increased platelet activation, aggregation, and thrombosis.21,22 Therefore, essential hypertension is considered to be associated with a greater acceleration of the thrombogenic condition, which is why several studies have recommended the administration of antiplatelet agents, such as aspirin and clopidogrel, in patients with hypertension.21,23 In addition, 5HT is known to be associated with myocardial infarction.13,24,25 Yamada et al.13 reported that a 5HT2A receptor gene polymorphism was related to myocardial infarction, particularly the TT genotype of the 5HT2A receptor gene, which might enhance the susceptibility to acute myocardial infarction. However, whether depressive disorder is associated with cardiovascular events, along with the impact of anti-depressant medication, including SSRIs on cardiovascular events, is still under debate.26 Until recently, SSRI was believed to have no additive adverse impact on cardiovascular outcomes, as shown in the SADHART study, in which sertraline, a popular SSRI, showed no statistically significant differences compared with placebo in terms of the occurrence of cardiovascular events.27,28
Increased serum 5HT during coronary intervention has also been reported, and platelet activation during coronary angioplasty has been demonstrated in animal model studies.29,30 Gasperetti et al.11 first reported the relationship between increased platelet aggregation and 5HT during balloon coronary angioplasty among patients with stable coronary artery disease, according to platelet aggregation analysis of blood drawn from the coronary sinus. From this study, it was postulated that balloon-induced arterial injury induces hyperresponsiveness to 5HT, leading to platelet activation and aggregation, and that 5HT is an important mediator of platelet thrombosis during balloon angioplasty.11 In the present study, the level of serum 5HT was directly measured and compared between patients with ACS or CSA undergoing PCI. Patients in the CSA and ACS groups showed increased serum serotonin after PCI compared with baseline values, suggesting that balloon-induced intimal injury may be associated with platelet activation. In CSA, PCI causes barotrauma to the initially intact fibrous cap of atherosclerotic plaque, which leads to intimal injury, such as intimal dissection that exposes the subintimally located von Willebrand factor (vWF). Thereafter, circulating platelets bind vWF via glycoprotein, activating platelets and releasing numerous vasoactive amines including serotonin, which, in turn, further recruit and activate other platelets under a positive feedback loop.31 In ACS, in the background of an already disrupted atherosclerotic plaque, PCI itself may also manipulate the pre-existing thrombi either by plaque rupture or erosion, leading to further platelet activation.32 Ko et al.33 reported increased 5HT levels in aspirated thrombi from patients with acute myocardial infarction undergoing primary PCI, suggesting a link between platelet activation and ACS in the PCI setting. These might be plausible explanations for the more profound incremental increases in serum serotonin in patients with ACS than those with CSA.
In terms of baseline characteristics, the rate of current smokers was higher in the present ACS group. Smoking is reported to affect 5HT/catecholamine signalling leading to an increase in the number of hyperactive platelets,34 which might influence serum serotonin values. However, no differences were shown in baseline and pre-PCI serum serotonin levels between the present ACS and CSA groups, which is not clearly understood. Although it might be arbitrary, serum serotonin may be more affected by the interventional procedure itself, thereby leading to platelet activation, than the baseline ACS or non-ACS status; however, this requires further investigation.
The main finding of the present study was that in the ACS group, serum serotonin reached an initial peak at the post-PCI time-point and dipped at 6 h, compared with an initial peak at 90 min and dip at 12 h after PCI in patients with CSA, which suggests faster and greater activation of platelets in patients with ACS than those with CSA. Of note, a rebound or second peak in serum serotonin level was observed at 24 h in both the ACS and CSA groups. The rebound phenomenon in platelet reactivity has been investigated in previous pharmacodynamic studies with ADP-receptor antagonists, mainly switching from a potent P2Y12 receptor inhibitor (prasugrel or ticagrelor) to the less potent clopidogrel.35,36 However, in the present study involving patients treated with loading doses of aspirin and clopidogrel, a rebound of serum serotonin after a decrease (or stabilization) was observed. This finding might suggest insufficient platelet inhibition achieved by aspirin and clopidogrel, which comprises the standard of care in most patients with CSA or selected patients with ACS undergoing PCI. Although speculative, initial suppression of platelets by the antiplatelet agents aspirin and clopidogrel might lead to biologic adaptation of platelets or megakaryocytes over time, conferring enhanced sensitivity to ADP or other stimuli, and making platelets more susceptible to reactivation.36 To overcome this problem, more potent P2Y12 receptor inhibitors, such as prasugrel or ticagrelor, might be necessary, particularly in patients with ACS, or a third agent could be added to inhibit serotonin-induced platelet activation. The present research group previously investigated the impact of triple antiplatelet therapy including aspirin, clopidogrel, and sarpogrelate (a selective 5HT2A receptor antagonist) in patients with acute STEMI undergoing PCI, and observed an improvement in left ventricular function at 6 months in the triple therapy group compared with the standard dual therapy group.37 Therefore, when prasugrel or ticagrelor are not indicated, adding a 5HT receptor antagonist to aspirin and clopidogrel might be a reasonable approach in patients undergoing PCI, whenever appropriate.
The present results may be limited by several factors. First, the study was conducted in a single centre and the number of included patients was small despite the enrolment of all consecutive patients during the study period. This may have resulted in the observed differences in some of the baseline characteristics (such as a higher proportion of current smokers in the ACS group) affecting the differences in serum serotonin values as confounding factors, other than the status of with or without ACS. Considering that the present study was conducted as a pilot and hypothesis-generating investigation, further studies with larger numbers of patients and a more suitable design would be helpful in elucidating serotonin-mediated platelet activation in a wide spectrum of patients undergoing PCI. Secondly, there might be other causes of serotonin elevation that act as confounding factors. To overcome this limitation, patients with acute myocardial infarction due to coronary vasospasm and those with cardiac arrest, in whom serum serotonin is considered an outlier, were excluded. If their values were included in the analysis, the results may have been different. Thirdly, serum serotonin measurements alone were used to compare between the ACS and CSA groups. Concomitantly performing a platelet aggregation test, with serotonin as an agonist, might provide more information on the serotonin-platelet mechanism. Fourthly, serotonin is believed to have circadian variations and reach its peak level in the night time compared with day time.38 Considering that, unlike in patients with CSA, PCI for ACS (including primary PCI for STEMI) is more frequently performed in the night time than day time, the circadian variation may have affected serum serotonin values to some extent. Finally, analysis of clinical outcomes according to ACS and CSA groups with different serum serotonin values could not be performed due to the limited number of study subjects. Despite these limitations, the present authors believe that the study provides a better understanding of the role of serotonin as a marker of platelet reactivity.
In conclusion, serum serotonin levels were higher in patients with ACS than in those with CSA, which might reflect higher platelet reactivity in patients with ACS. Thus, the authors speculate that serum serotonin might be used as a biomarker of platelet activation during PCI. In addition, under careful monitoring for bleeding events, triple antiplatelet agents, including a selective 5HT2A receptor antagonist, may be beneficial for patients undergoing PCI, particularly patients with ACS. These results may guide future studies into the role of serotonin as a new cardiac biomarker for platelet activity and as a therapeutic target.
Footnotes
Acknowledgments
We thank EJ Park, a colleague at the cardiovascular centre of Kangnam Heart Sacred Hospital, for helping with document collection
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was partially supported by Hallym University Research Fund 2017 (HURF-2017-84), contributed by JHC and DH.