
Abstract
Objective
To identify potential drug interactions (DIs) between pangenotypic direct-acting antivirals (pDAAs) and concomitant cardiovascular (CV) therapies in patients with chronic hepatitis C (CHC).
Methods
A retrospective observational study was carried out. Patients ≥18 years of age diagnosed with CHC and treated with pDAAs during 2017 were included. Information was collected on concomitant CV therapies and potential DIs [www.hep-druginteractions.org]. The pDAAs analyzed were sofosbuvir/velpatasvir (SOF/VEL), glecaprevir/pibrentasvir (GLE/PIB) and sofosbuvir/velpatasvir/voxilaprevir (SOF/VEL/VOX). An analysis including lipid-lowering drugs was also performed.
Results
In total, 1286 patients (mean age 64.9 years, 56.6% men) were recruited. The percentages of potential DIs with CV drugs were 1.9% contraindications, 38.1% clinically significant and 2.4% weak. When lipid-lowering drugs were included, the percentages of potential DIs with CV drugs were 10.3% contraindications, 46.3% clinically significant and 3.2% weak. Potential DIs associated with each pDAA were as follows (contraindications; clinically significant; weak): SOF/VEL (1.4%; 23.0%; 0.9%), GLE/PIB (12.8%; 60.8%; 4.7%) and SOF/VEL/VOX (16.6%; 55.1%; 4.9%).
Conclusions
Approximately on third of patients with CHC are concomitantly treated with CV drugs. SOF/VEL may have fewer DIs with CV drugs than other pDAAs.
Keywords
Introduction
Chronic hepatitis C virus (HCV) infection is a worldwide public health problem with an estimated prevalence of 1% to 2% among the general population.1–4 Research into viral replication mechanisms has identified potential therapeutic targets. 5 The development of new direct-acting antivirals (DAAs) against HCV was a great step forward in the treatment of this infection. The aim of these drugs is to achieve greater efficacy and safety, with fewer side effects, including potential drug interactions (DIs). Many DIs arise from drug metabolism mediated by cytochrome P450 (isoenzyme CYP3A) and/or P-glycoprotein transport.6,7
For several years, treatment regimens were used according to the HCV genotype in each individual patient. However, current DAAs are pangenotypic (pDAAs) and are effective against all HCV genotypes. 8 A single DAA alone cannot prevent HCV replication and mutation. For this reason, treatment should comprise 2 to 3 drugs from different inhibitor classes. 9
In general, patients receiving pDAAs are older and have increased risks of comorbidities. Thus, they may be receiving several drugs, which can result in adverse effects arising from DIs. 10 In addition, DIs with therapies used to treat comorbidities may contraindicate the use of pDAAs.10–12 A recent study conducted in Spain reported high rates of comorbidities and concomitant medication rates in patients with HCV. The most commonly prescribed therapies with potential DIs were those related to the cardiovascular (CV) system and the central nervous system. 13
Careful review of the medications used by patients with HCV is therefore advisable. 2 ,10–13 Little information is currently available on the true risks of DAAs based on patterns of concomitant medication use at the population level. The objective of our study was thus to identify DIs between pDAAs and concomitant CV therapies in patients with HCV in standard clinical practice in Spain.
Patients and methods
An observational, retrospective study based on review of medical records (from electronic databases) was carried out. The study population was obtained from the records of healthcare providers corresponding to different Spanish centers (unified in the BIG-PAC anonymized database). 14 Data were derived from electronic medical records and other supplementary databases from seven Spanish Autonomous Communities (1.8 million patients). Before exporting from the BIG-PAC database, all electronic records were rigorously anonymized by the centers/hospitals of origin in compliance with Organic Law 3/2018 on the Protection of Personal Data and Guarantee of Digital Rights. Patients ≥18 years of age diagnosed with HCV infection (ICD-10-MC [B18.2]) and treated with pDAAs during 2017 were consecutively recruited. The patients were required to meet the following criteria: (i) age ≥18 years; (ii) diagnosis of HCV infection at least 12 months prior to the start of the study (patients active in the database); (iii) enrolment in the chronic medication program for obtaining medical prescriptions (with a documented record of the daily dose and duration of each treatment and ≥2 prescriptions over the follow-up period for any drug administered); and (iv) regular monitoring throughout the study (≥2 healthcare registries in the electronic system). Patients who transferred to other sites, as well as those who moved outside the study area, were excluded.
The study variables included demographic data, body mass index (BMI, kg/m2), HCV duration, personal history (detailed in Table 1) and comorbidities (ICD-10-MC). The Charlson comorbidity index was used as a summary variable of general comorbidity 15 to assess severity. Among patients with HCV infection, we identified those receiving concomitant treatment with one of the following CV drug classes: anticoagulants, cardiac therapy, antihypertensive agents, diuretics, beta-blockers, calcium channel blockers, and agents acting on the renin–angiotensin system. 13 Treatment description was based on the Anatomical Therapeutic Chemical Classification System. 16 Patient assignment to a concrete treatment regimen was determined according to standard clinical practice. The pDAAs selected were sofosbuvir/velpatasvir (SOF/VEL), glecaprevir/pibrentasvir (GLE/PIB) and sofosbuvir/velpatasvir/voxilaprevir (SOF/VEL/VOX). Concomitant medications were analyzed during the antiviral treatment period, and only chronic or regular medications administered to patients were assessed. An additional analysis was performed including lipid-lowering medications. Contraindicated drugs and major interactions were described.
General characteristics of study patients.

Values reported as mean (standard deviation) or percentages.
CV, cardiovascular; BMI, body mass index; COPD, chronic obstructive pulmonary disease; HIV/AIDS, human immunodeficiency virus/acquired immunodeficiency syndrome.
To identify potential DIs, the guidelines of the University of Liverpool 17 were followed. This resource is recommended by the European Association for the Study of the Liver. 2 Potential DIs were classified as contraindications, clinically significant, or weak. In addition, we identified the main indications for prescription of drugs such as enalapril, atorvastatin, amiodarone and digoxin.
Data were anonymized and all analyses were confidential, in accordance with Spanish legislation on personal data protection. The study was classified by the Spanish Agency for Medicines and Health Products (EPA-OD) and was subsequently approved by the Clinical Research Ethics Committee of the Unió Catalana Balears de Hospitals de Barcelona, Spain (reference: 15/49). According to Spanish legislation, retrospective studies of secondary data do not require written informed consent of the patient. Data were validated to ensure quality and consistency of the records. Descriptive univariate statistical analyses were performed. The SPSSWIN version 23 statistical package was used for all analyses. Values of p < 0.05 were considered statistically significant.
Results
We identified 1286 HCV patients (37.5%) receiving chronic CV medications (Figure 1). Table 1 shows the general characteristics of the patients. Patients were 64.9 years old on average (standard deviation [SD]: 12.5 years) and 56.6% were men. Their mean BMI was 28.1 kg/m2, and the mean Charlson index was 1.6 (SD: 1.1). The most common comorbidities were arterial hypertension (68.1%), dyslipidemia (41.6%), anxiety disorders (36.5%) and diabetes (29.8%). The mean number of medications received was 3.6 (SD: 2.5) per patient per year.

Study flow chart.
The drugs administered for CV therapy (excluding lipid-lowering drugs) showing potential DIs with pDAAs included enalapril (n = 365), amlodipine (n = 150), acenocoumarol (n = 77), olmesartan (n = 73) and valsartan (n = 60) (Table 2). The percentages of potential DIs associated with CV drugs were 1.9% contraindications, 38.1% clinically significant and 2.4% weak. The percentages of DIs associated with each class of pDAAs were as follows (contraindications; clinically significant; weak): SOF/VEL (1.4%; 8.1%; 0.9%), GLE/PIB (0.2%; 55.3%; 4.7%) and SOF/VEL/VOX (1.6%; 53.0%; 4.0%) (Figure 2a).
Potential drug interactions of pangenotypic direct-acting antivirals (pDAAs).
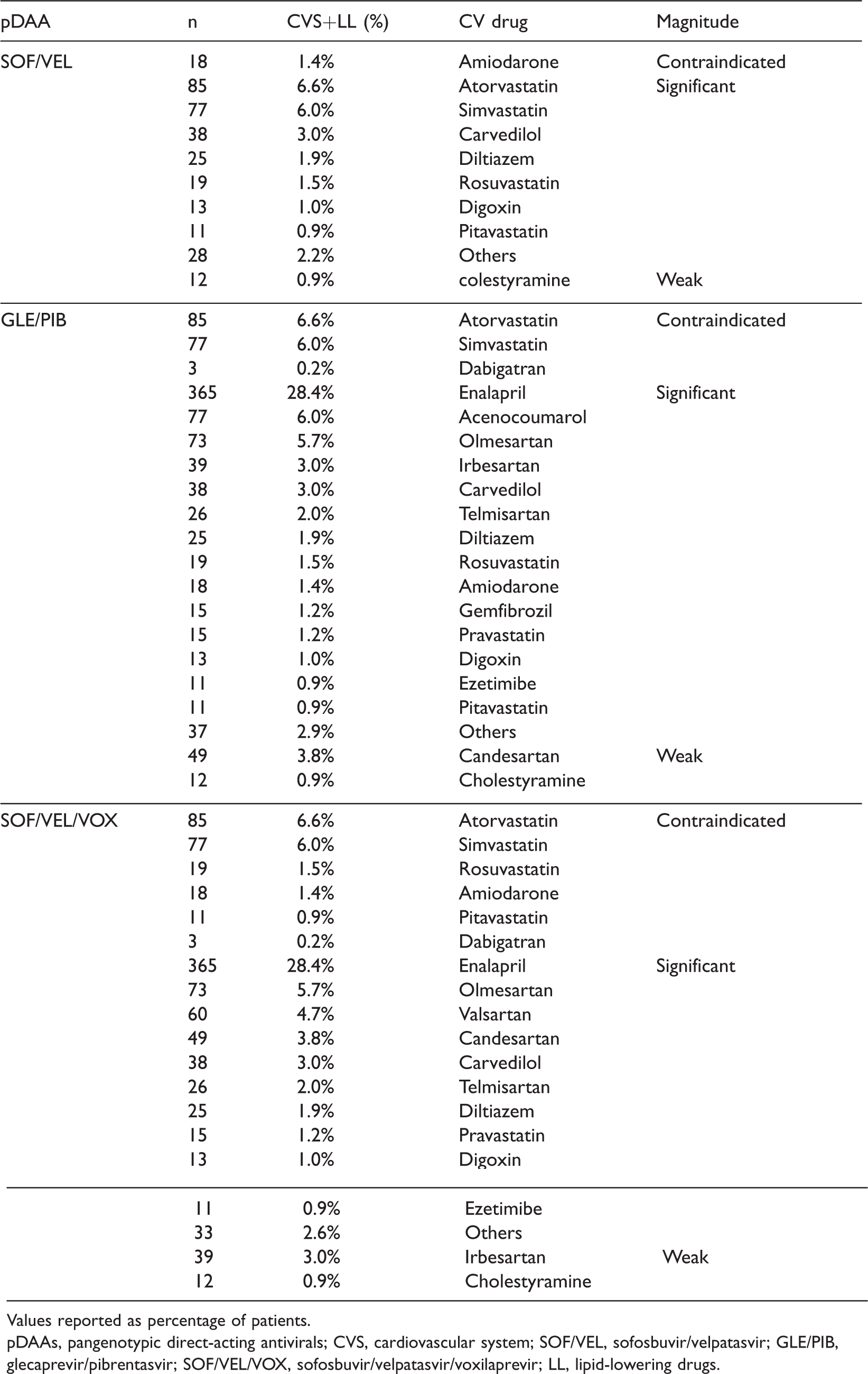
Values reported as percentage of patients.
pDAAs, pangenotypic direct-acting antivirals; CVS, cardiovascular system; SOF/VEL, sofosbuvir/velpatasvir; GLE/PIB, glecaprevir/pibrentasvir; SOF/VEL/VOX, sofosbuvir/velpatasvir/voxilaprevir; LL, lipid-lowering drugs.
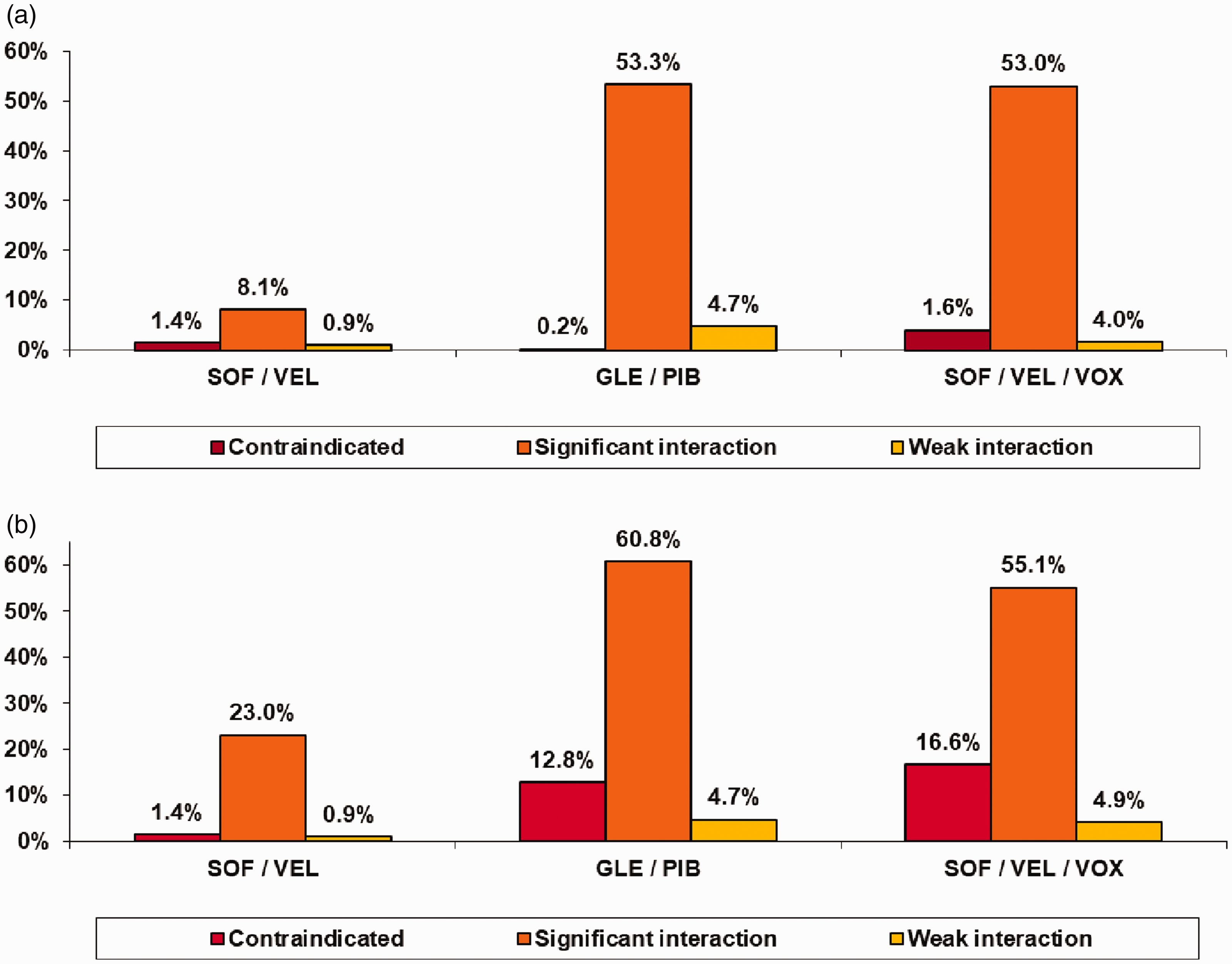
Potential cardiovascular system drug interactions according to pangenotypic direct-acting antiviral (pDAA) regimen. (a) Not including lipid-lowering agents and (b) Including lipid-lowering agents.
Inclusion of lipid-lowering drugs (particularly atorvastatin and simvastatin) in the analysis yielded the following percentages of potential DIs: 10.3% contraindications, 46.3% clinically significant and 3.2% weak. The percentages of DIs associated with each class of pDAAs were as follows (contraindications; clinically significant; weak): SOF/VEL (1.4%; 23.0%; 0.9%), GLE/PIB (12.8%; 60.8%; 4.7%) and SOF/VEL/VOX (16.6%; 55.1%; 4.9%) (Table 2 and Figure 2b).
The reasons for prescribing CV drugs were as follows: (i) enalapril (n = 365): arterial hypertension (n = 195, 53%), heart failure (n = 95, 26%) and renal failure (n = 75, 21%); (ii) atorvastatin (n = 85): secondary prevention (n = 52, 61%) and dyslipidemia (n = 33, 39%); (iii) amiodarone (n = 18): tachycardia (n = 8, 44%) and ventricular fibrillation (n = 10, 56%); and (iv) digoxin (n = 13): heart failure with atrial fibrillation (n = 13, 100%).
Atorvastatin was the drug with the highest potential for DIs (contraindicated: n = 85, 6.6%). During the administration of pDAAs, reasonable alternatives determined by physicians included the following: (i) discontinuation of atorvastatin (n = 14, 16.5%); (ii) dose reduction (n = 33, 38.8%); and (iii) substitution with another drug (n = 38, 44.7%).
Discussion
The present study showed that more than one third of patients with HCV infection received concomitant medications acting upon the CV system. Statins such as atorvastatin and simvastatin had increased risks of potential DIs. SOF/VEL had a lower risk of DIs than other pDAAs.
Patients with HCV infection tend to have many comorbidities. For example, Basseri 18 found that kidney disease, diabetes and obesity were more prevalent in patients with HCV infection compared with the general population in the United States. McKibben 19 concluded that HCV infection was associated with CV disease risk. Notwithstanding its methodological limitations, the findings of our study agree with those reported in the literature. 2
When lipid-lowering drugs were included in our analyses, the percentages of potential DIs were 10.2% contraindications, 46.3% clinically significant, and 3.2% weak. Some studies have found that two-thirds of patients experience potential interactions with DAAs, and that approximately 20% of concurrent drugs are contraindicated.10,11,13 The PITER study 20 found that 30% to 44% of all patients receiving DAAs were at risk of clinically significant interactions. The authors underscored the need for greater care when these drugs are administered, particularly to patients with moderate to severe liver disease. Other studies reported similar or substantially higher percentages of DIs.10–13,21 Our results agree with those of previous studies, although we recorded a lower proportion of clinically relevant drug interactions. This may be because our study was conducted with the more recently marketed pDAAs. The literature available for comparison is relatively limited.
We found that SOF/VEL exhibited a lower proportion of DIs compared with other regimens. SOF is a NS5B polymerase inhibitor, while VEL is an NS5 replication complex inhibitor. 8 The intracellular metabolic activation of SOF is mediated by nucleotide phosphorylation and hydrolase activity (generally of low affinity and high capacity), and is therefore unlikely to be affected by concomitant medications. 22 Recent reviews reported that administration of drugs concomitantly with SOF generally resulted in fewer DIs than with protease inhibitor-based regimens. However, the analysis of each DI was theoretical, and further interaction studies would be required to confirm the real effect. 22 Interactions may occur at the phases of drug absorption, distribution, or metabolism. The P450 enzyme system (CYP450), and particularly isoenzyme CYP3A4, is responsible for most drug oxidation. The administration of inducers, inhibitors or substrates of this enzyme system may alter the plasma concentrations of drugs, and thus the pharmacological response.23,24
According to the indications for administration of some CV medications such as enalapril, atorvastatin, amiodarone and digoxin, it would be difficult to adopt a single strategy during the period of pDAA administration. For example, it is advisable to monitor blood pressure and heart rate and/or to reduce the dose of antihypertensive treatments. In the case of amiodarone, one should consider replacement with another drug or dose reduction in the face of DIs, and cardiac function should be monitored. In the case of statins, it is advisable to reduce the dose and monitor potential side effects because of the increased risk of myopathy and rhabdomyolysis. Nevertheless, the safest pDAA should be chosen based on the concomitant medications used in each patient. 25 The results of our study regarding potential DIs with statins have also been reported in other published studies. 26
The present study had several limitations inherent to retrospective studies. These included underreporting of the disease and potential variability of professionals and patients, because an observational design was used. It should be noted that this study design is not free from biases, including those based on socioeconomic background, cultural or educational level, drug doses used, treatment duration, treatment adherence, or treatment suitability. In addition, over-the-counter drugs, patient self-medication or prescriptions issued at other health institutions (public or private) were not considered in our study. Our study could not account for over-the-counter drugs (not funded by the Spanish National Health System). However, we believe that this circumstance is rare. However, these factors may together have led to underestimation of DIs in our study. Our study demonstrated several potential DIs in patients with HCV. Other limitations of the study included bias in selection of the drug to be administered by the attending physician, as well as potentially limited external validity. Our results therefore should be interpreted with caution. Potential DIs are a serious problem in clinical practice, but many of them can be avoided by adjusting drug dosage or selecting a safer alternative drug. New care models, including e-prescription support tools or clinical decision support systems, may be of considerable help for clinicians in this respect. Early detection and treatment are important for prevention of the most severe consequences of HCV infection.
Conclusions
About one third of patients with HCV infection were concomitantly treated with CV drugs. Protease inhibitor pDAAs may have increased numbers of DIs with CV drugs. SOF/VEL may have fewer DIs than other pDAAs.
Footnotes
Author contributions
The study was conceived and designed by A. Sicras. Data compilation and statistical analysis was performed by A. Sicras. All authors participated in data interpretation and in manuscript writing, review, and approval.
Declaration of conflicting interest
A. Sicras was an independent consultant for the development of this manuscript. R. Morillo has no conflicts of interest.
Funding
This study was sponsored by Gilead Sciences.