
Abstract
Objective
We performed a meta-analysis to evaluate the prognostic and clinicopathological significance of programmed cell death-1 (PD-1) expression in patients with hepatocellular carcinoma (HCC).
Methods
We searched the Wanfang, Chinese Biomedical Literature, CNKI, PubMed, Embase, and Web of Science databases for relevant articles from inception to 1 July 2020. Statistical analysis was performed using RevMan 5.3 (Cochrane, London, UK) and Stata 14.0 software (StataCorp LP, College Station, TX, USA).
Results
Eight studies involving 732 patients with HCC were included. Higher expression of PD-1 predicted longer disease-free survival [hazard ratio (HR) 0.53, 95% confidence interval (CI): 0.38–0.72]. No significant correlation was observed between PD-1 expression and overall survival (HR 0.89, 95% CI: 0.58–1.35). PD-1 expression was correlated with age [odds ratio (OR) 0.66, 95% CI: 0.46–0.94] and alpha-fetoprotein level (OR 2.27, 95% CI: 1.45–3.55); no correlation was observed with sex, tumor size, tumor metastasis, hepatitis B virus history, tumor stage, or tumor multiplicity. Sensitivity analysis demonstrated no excessive effect on stability of the pooled results. No significant publication bias was found among the identified studies.
Conclusion
PD-1 overexpression predicted better disease-free survival in patients with HCC. Moreover, PD-1 expression was associated with age and alpha-fetoprotein level.
Keywords
Introduction
According to global cancer statistics, hepatocellular carcinoma (HCC) had become the sixth most common cancer and the fourth leading cause of cancer-related death worldwide by the end of 2018. There are approximately 841,000 new cases and 782,000 deaths each year, posing a substantial threat to human life and health. 1 , 2 Despite significant improvements in diagnosis and treatment in the past few decades, the mortality associated with HCC has remained high, and the 5-year survival rate after surgery is around 35%. 3 The high mortality may be due to the lack of early diagnosis and specific markers to predict progression and prognosis. The American Association for the Study of Liver Diseases and European Association for the Study of the Liver guidelines recommend the Barcelona Clinic Liver Cancer (BCLC) staging algorithm for the treatment of liver cancer, which currently includes five treatment strategies (i.e., liver transplantation, surgical resection, radiofrequency ablation, transarterial embolization or chemoembolization, and sorafenib). 4 However, the BCLC staging algorithm is not perfect and needs to be updated regularly. An increasing number of new treatment methods have been proposed and adopted, with their effectiveness and safety gradually becoming established. New diagnostic and therapeutic methods are necessary to improve the prognosis of patients with HCC.
Programmed cell death-1 (PD-1), a member of the B7-CD28 co-stimulatory receptor family, is mainly expressed on activated T lymphocytes, B lymphocytes, and monocytes. Its ligand, programmed death ligand 1 (PD-L1), is mainly expressed on cancer cells. 5 After binding to PD-L1, PD-1 inactivates the T cell or induces cell death, which inhibits cellular immune responses and promotes tumor cell growth.6–10 Current clinical studies have found that PD-1 is highly expressed in gastric cancer and upper urothelial carcinoma, which may be an indicator of patient survival. 11 , 12
Studies have shown that patients with advanced liver cancer respond well to PD-1/PD-L1 inhibitors, which lead to prolonged survival and better prognosis. 13 However, few reports are currently available on the expression of PD-1 in HCC. It has been speculated in some studies that the expression level of PD-1 is closely related to the overall survival of patients with HCC. 14 , 15 Other studies have shown that PD-1 expression does not affect the survival of HCC patients.16–20 In the present meta-analysis, we explored the prognostic value of PD-1 expression in patients with HCC and evaluated the relationship between PD-1 expression and clinicopathological characteristics in HCC.
Materials and methods
Ethics
This study did not involve human subjects, so informed consent was not required. In addition, no approval was required from an institutional review board.
Literature search
This meta-analysis is based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 21 Two independent investigators (QZ and KZ) searched the WanFang, Chinese Biomedical Literaure (CBM), CNKI, PubMed, Embase, and Web of Science databases for articles published before 1 July 2020. The search terms were “hepatocellular carcinoma,” “hepatocellular cancer,” “HCC,” “liver cancer,” “programmed cell death-1,” and “PD-1.” After initial screening based on titles and abstracts, studies containing relevant data were retrieved for full-text assessment, and only original articles were considered. Finally, eight articles meeting the following criteria were included for further evaluation and data extraction (Figure 1). Data extraction and analysis were performed by researchers trained in literature search, statistics, and evidence-based medicine.
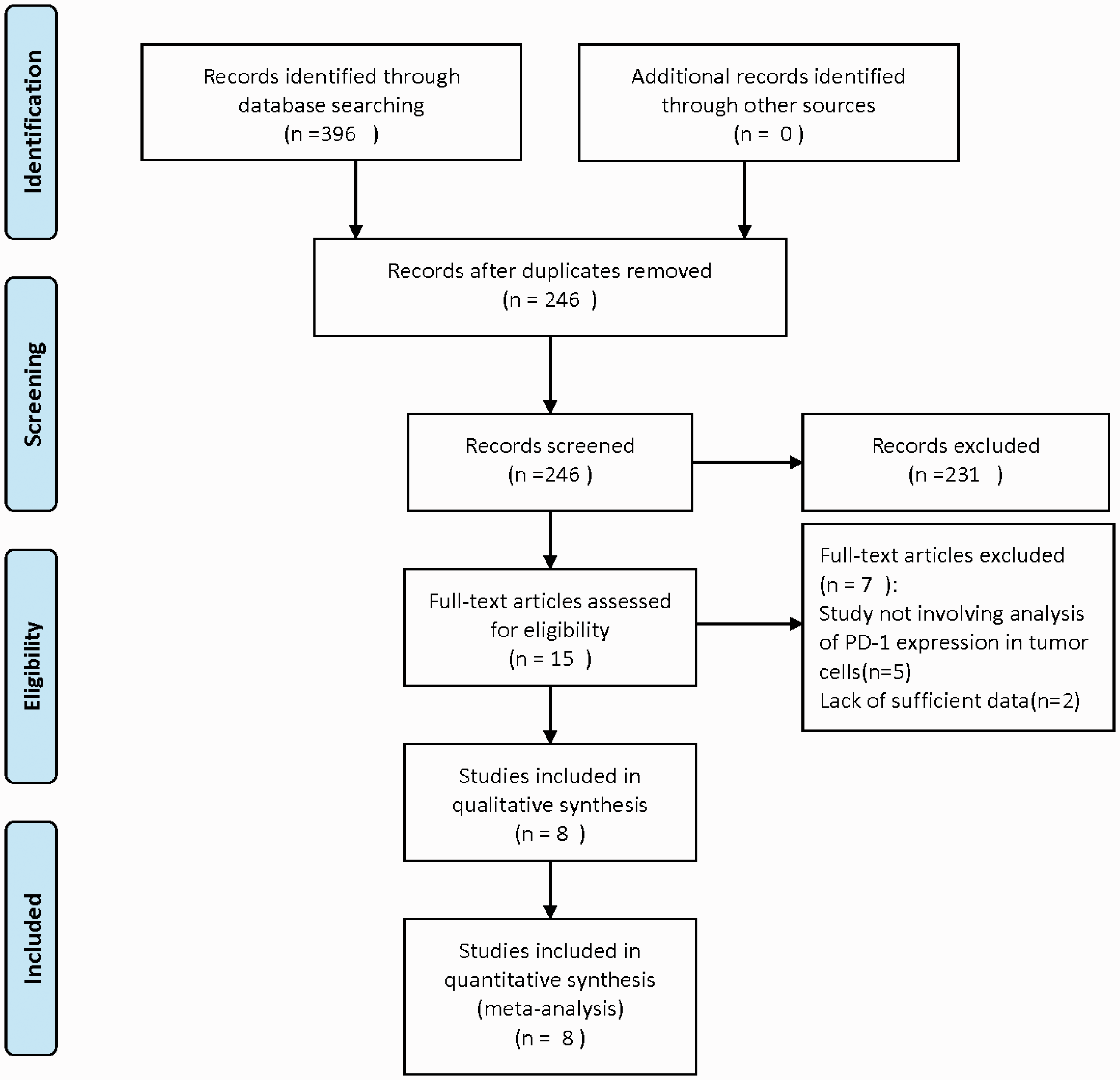
PRISMA flowchart showing the process of identifying articles.
Study selection
Included studies met the following criteria: (1) HCC diagnosed by histopathology; (2) PD-1 expression detected by immunohistochemistry and other methods; (3) reported PD-1 survival-related data, including overall survival (OS) and disease-free survival (DFS); (4) patients divided into PD-1 positive (high) and PD-1 negative (low) groups; (5) studies evaluated the relationship between PD-1 expression and clinicopathological characteristics, such as age, sex, tumor node metastasis (TNM) staging, BCLC stage, and tumor size; and (6) full-text articles. The following types of studies were excluded: (1) conference abstract, case series reports, or letters; (2) animal experiments; (3) studies that lacked measurement indicators and survival data.
Data extraction
Data were double input into EpiData software (version 3.0; The EpiData Association, Odense, Denmark) by two investigators (QZ and KZ); differences were resolved through group discussions. The following information was extracted: name of the first author and year of publication, country, histology type, tumor stage, sample size, PD-1 detection method, hazard ratio (HR) and 95% confidence interval (CI) for OS and DFS, if provided. The HR and 95% CI were obtained from Kaplan–Meier survival curves via Engauge Digitizer version 4.1 (http://digitizer.sourceforge.net/).
Quality assessment
The Newcastle–Ottawa scale (NOS) was applied for quality evaluation, with a score of >6 indicating high-quality research.
Statistical analysis
The 95% CIs and HRs were used to evaluate the relationship between PD-1 expression and OS and DFS. Odds ratios (OR) and 95% CI were used to evaluate the effect of PD-1 expression on clinicopathological characteristics. First, statistical heterogeneity tests were performed. When there was no statistical heterogeneity among the included studies (I2 < 50% or P > 0.1), a fixed-effects model was applied; when statistical heterogeneity was observed (P < 0.1 or I2 ≥ 50%), the source of heterogeneity was analyzed. In the absence of significant clinical and methodological heterogeneity, statistical heterogeneity was considered, and a random-effects models was adopted for analysis. When clinical heterogeneity was significantly high, no meta-analysis was performed (only a descriptive analysis). Begg’s funnel plot was applied to evaluate publication bias. Statistical analysis was performed by Stata 14.0 (StataCorp. LP, College Station, TX, USA) and RevMan 5.3 (Cochrane, London, UK). All P-values were two-sided and P < 0.05 was considered the threshold of statistically significance.
Results
Characteristics of the included studies
A total of 396 studies were preliminarily retrieved; after screening, eight articles with 732 patients were finally included.14–20, 22 Basic characteristics of the included studies are shown in Table 1. The NOS scale was applied to evaluate literature quality, and the included studies all scored 7 or 8, indicating high-quality studies (Table 2).
Main characteristics of eligible studies included in the meta-analysis.

ELISA, enzyme-linked immunosorbent assay; IHC, immunohistochemistry; qRT-PCR, quantitative real-time PCR; OS, overall survival; HBV, hepatitis B virus; AFP, alpha-fetoprotein; DFS, disease-free survival; BCLC, Barcelona Clinic Liver Cancer; TNM, tumor node metastasis; NA, data not available.
Newcastle–Ottawa Scale for quality assessment.

Prognostic role of PD-1 expression for OS and DFS
By pooling the data of six studies, no significant difference (HR = 0.89, 95% CI: 0.58–1.35) but significant heterogeneity (P = 0.0002; I2 = 79%) was found in OS between high and low PD-1 groups (Figure 2). By pooling the data of three studies, DFS was found to be significantly different between high and low PD-1 groups (HR = 0.53; 95% CI: 0.38–0.72; P < 0.0001) with no significant heterogeneity (P = 0.14; I2 = 49%) (Figure 3).

Forest plot of hazard ratios for the association of programmed cell death-1 (PD-1) expression with overall survival in patients with hepatocellular carcinoma.

Forest plot of hazard ratios for the association of programmed cell death-1 (PD-1) expression with disease-free survival in patients with hepatocellular carcinoma.
Association between PD-1 expression and clinicopathological features
Correlations between PD-1 expression and clinicopathological features were evaluated by OR and 95% CI (Table 3). At least two studies were included in each subgroup analysis. The clinicopathological features included age, sex, tumor size, tumor metastasis, hepatitis B virus (HBV) history, tumor stage, tumor multiplicity, and alpha-fetoprotein (AFP). Age and AFP were found to be significantly correlated with the expression of PD-1 (P = 0.023 and P = 0.000, respectively). No significant association was found between the expression of PD-1 and the other clinicopathological features listed above (Table 3).
Association between PD-1 expression and clinical features of patients with hepatocellular carcinoma in meta-analysis.

P-values were obtained using the “metan” program in Revman 5.3; P < 0.05 was considered statistically significant.
HBV, hepatitis B virus; AFP, alpha-fetoprotein; FEM, fixed-effects model; BCLC, Barcelona Clinic Liver Cancer; TNM, tumor node metastasis; OR, odds ratio; CI, confidence interval.
Sensitivity analysis
Sensitivity analysis was conducted to assess the potential influence of each study on the pooled HRs. The results demonstrated that no study had an excessive effect on the stability of the pooled results of comparisons (Figure 4). Therefore, results of this meta-analysis were considered robust.

Sensitivity analysis for all eligible studies investigating the association between programmed cell death-1 (PD-1) expression and overall survival in patients with hepatocellular carcinoma.
Publication bias
Begg’s funnel plots were used to evaluate potential publication bias. As shown in Figure 5, the funnel plots revealed no asymmetry for OS (Begg’s test: P = 0.091).

Begg’s funnel plot for publication bias test including programmed cell death-1 (PD-1) expression and prognosis in hepatocellular carcinoma.
Discussion
HCC is a common malignant tumor of the digestive system. Its incidence and mortality are relatively high worldwide and are still trending upward in many industrialized countries. 23 Studies have found that most HCCs are correlated with chronic HBV infection; alcoholic cirrhosis, smoking, obesity, and alcoholism are also common risk factors for HCC.24–28 Patients with HCC generally have a poor prognosis. Studies have reported that the 5-year relative survival rate of liver cancer patients in Europe is only 12%, and HCC seriously affects human life and health. 29 HCC is difficult to treat. On the one hand, the existing treatments are costly and have poor compliance, so few patients with liver cancer can be treated in clinical practice by completely curing the hepatitis infection. On the other hand, the treatment options for patients with advanced HCC are often limited, and common chemotherapy agents are accompanied by toxic side effects. 30 , 31 Therefore, finding a new treatment is critical for treating and improving the prognosis of patients with HCC.
Researchers are increasingly using immune checkpoints to explain the immune escape of tumors. The main immune checkpoints are PD-1/PD-L1, which are coinhibitory molecules expressed on the surface of various tumors that downregulate T cells. Antitumor activity is involved in the immune escape of tumor cells; therefore, treatments that block the PD-1/PD-L1 pathway have become the focus of cancer immunotherapy.32–36 Immunotherapy is now the fourth most common cancer treatment after surgery, radiotherapy, and chemotherapy. In the United States, Europe, and Japan, antibodies against PD-1 have been approved for the clinical treatment of melanoma and non-small-cell lung cancer. 37 In addition, PD-1 is abnormally expressed in various cancers, and this abnormal expression can be used as a marker for poor prognosis in patients with breast cancer and thymic carcinoma. 38 However, the relationship between PD-1 expression and the prognosis of patients with HCC remains controversial. 39 Some studies report a significant correlation between high PD-1 expression and poor prognosis.14–17 Other studies have reported no significant correlation between the two. 20 , 22
In this study, we combined and analyzed the available information in the published literature to evaluate the relationship between PD-1 expression and HCC prognosis. The results showed that PD-1 expression was not significantly related to OS in HCC patients but was significantly related to DFS. In terms of clinicopathological features, high PD-1 expression was correlated with age and AFP but had no correlation with sex, tumor size, tumor metastasis, HBV history, tumor stage, or tumor multiplicity.
In some patients with solid tumors, PD-1 expression can be used as an independent factor to determine prognosis, but it depends on the pathological type of the tumor. For example, PD-1 expression is detected in esophageal cancer tissues, but this expression is not related to the survival rate of patients with esophageal cancer.40,41 In patients with renal cell carcinoma, PD-1 expression is closely related to overall survival rate. 42 , 43 Therefore, whether PD-1 expression can be used as a prognostic marker may depend on the pathological tumor type or on tumor tissues with certain specific clinicopathological characteristics.
To the best of our knowledge, this is the first meta-analysis to evaluate the prognostic and clinical value of PD-1 expression in HCC patients and thus our study is of great importance. The studies included assessed patients after HCC surgery, but the treatment provided after surgery was not clear. We attempted to carry out subgroup analyses according to the mode of postoperative treatment, but the information provided in published articles was limited and could not be analyzed further. However, we speculate that some patients may have used immunosuppressants, which may explain the observation that the DFS of the group with high PD-1 expression was significantly better than that of the group with low expression. We suggest that high expression of PD-1 is a marker for prognosis of patients receiving immunosuppressive therapy for HCC.
Several limitations existed in our study. First, the cut-off values for PD-1 expression were measured using different methods and varied among studies, which may have caused heterogeneity in the overall results. The causes of HCC, such as hepatitis C infection or alcohol consumption, and their effects on the expression and prognostic role of PD-1 were unclear. Second, ethnicity may affect the prognostic value of PD-1 in patients with HCC. Our study included only Asian populations; studies focused on other ethnicities were not found. Therefore, it is unknown whether our conclusions could be generalized to other ethnicities. Different ethnicities and varying levels of medical development in different areas may also influence the outcomes of HCC patients, which may affect the results. In addition, all included studies were based on postoperative analysis. The treatment methods applied before and after surgery were unclear, which affected the quantitative analysis of prognosis in this meta-analysis. Finally, not all HRs and 95% CIs were directly extracted from the studies; we had to extract some data using Kaplan-Meier curves, which influenced the precision of the data.
Conclusion
Despite its limitations, our meta-analysis found that PD-1 expression was correlated with prognosis in patients with HCC. Patients in the high PD-1 expression group had a significantly better prognosis than those in the low PD-1 expression group. Moreover, expression of PD-1 was significantly correlated with age and AFP level. Our results indicate that PD-1 may be related to the occurrence and development of HCC; these findings warrant further investigation.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.