
Abstract
Objective
This study aimed to examine the relationship between total bilirubin levels and initial ischemic stroke in patients with non-valvular atrial fibrillation.
Methods
This was a retrospective study. Atrial fibrillation was diagnosed by 24-hour Holter electrocardiography and serum total bilirubin levels were divided into quintiles. Ischemic stroke was diagnosed by symptoms, signs, and a medical image examination. The multivariate Cox proportional hazards model and survival analysis were used to estimate the association of total bilirubin with initial ischemic stroke.
Results
We studied 316 patients with non-valvular atrial fibrillation. During follow-up, there were 42 (13.29%) first ischemic strokes. After multivariate adjustment, for each 1 µmol/L increase in total bilirubin, the risk of first ischemic stroke increased by 4% (95% confidence interval [CI]: 1.01, 1.07). When using the first quintile as the reference, from the second to fifth quintiles, the risks of first ischemic stroke were 0.52 (95% CI: 0.17, 1.65), 0.23 (95% CI: 0.06, 0.87), 0.92 (95% CI: 0.32, 2.67), and 1.33 (95% CI: 1.09, 4.41), respectively. The optimal cut-off point of total bilirubin for the lowest risk of ischemic stroke was 17.0 µmol/L.
Conclusions
Total bilirubin levels are nonlinearly associated with initial ischemic stroke in patients with non-valvular atrial fibrillation.
Keywords
Introduction
Stroke is one of the most common and undertreated chronic diseases, and is the second most common cause of death worldwide.1,2 In China, ischemic stroke is the most common type of stroke.3,4 Stroke is a disease with multiple factors. Although some certain factors, such as atrial thrombosis and hypertension, are closely related to the occurrence of stroke, its mechanism is still unclear.5,6 Previous studies have shown that excessive oxidative stress causes structural and functional damage to the brain, which is an important pathophysiological process of stroke.7–9 Bilirubin, which is a major metabolite of iron porphyrin compounds in the body, is also an important indicator for clinical judgment of jaundice and abnormal liver function. 10 Studies have also demonstrated that bilirubin causes irreversible damage to the brain and nervous system with high concentrations, 11 but also has antioxidant functions that can inhibit oxidation of linoleic acid and phospholipids, 12 which are related to stroke. Although bilirubin is considered to have a protective effect on ischemic diseases owing to its strong antioxidant properties, 13 in recent years, studies have indicated that the relationship between bilirubin and stroke is controversial. A Mendelian randomization study on Koreans showed that bilirubin levels were not a risk determinant of stroke, and there was no obvious causal effect of serum total bilirubin levels on stroke. 14 However, a two-sample summary Mendelian randomization study provided clear evidence that there was a significant causal relationship between elevated bilirubin levels and reduced stroke. 15 This finding suggests that total bilirubin could serve as a therapeutic target for oxidative stress-related diseases, such as stroke. Additionally, a meta-analysis of 11 observational studies involving 131,450 subjects showed that there was an inverse association between circulating total bilirubin levels and a risk for ischemic stroke. 16
Stroke is a major public health problem. 17 Early prevention and early warning for stroke are necessary and important, especially for the population at high risk of stroke, such as those with atrial fibrillation.18,19 A large number of clinical or cohort studies have shown that atrial fibrillation is a most common risk factor for stroke owing to atrial thrombus formation and embolization, 20 and it is also a common arrhythmia.21,22 Identifying stroke-related risk factors and early warning in patients with atrial fibrillation are necessary. At present, the relationship between serum bilirubin levels and stroke in patients with atrial fibrillation is unclear. Therefore, this study aimed to examine the relationship between serum total bilirubin levels and the occurrence of initial ischemic stroke in patients with non-valvular atrial fibrillation.
Methods
Study population
We performed a retrospective single-center study. A total of 2756 patients were consecutively enrolled from the Central Hospital of Yongzhou, China between September 2014 and November 2019. Participants who completed 24-hour Holter monitoring and were aged ≥18 years were enrolled. The exclusion criteria mainly included non-atrial fibrillation, valvular atrial fibrillation, missing bilirubin data, and having a previous history of stroke. A flow diagram of patients who were included for analysis is shown in Figure 1. This retrospective cohort study was approved by the Ethical Committee of Yongzhou Central Hospital (approval No. 2019-17), Yongzhou, China, with a waiver of informed consent. During the study, information and materials related to the specific identity of the participants were completely and strictly concealed.
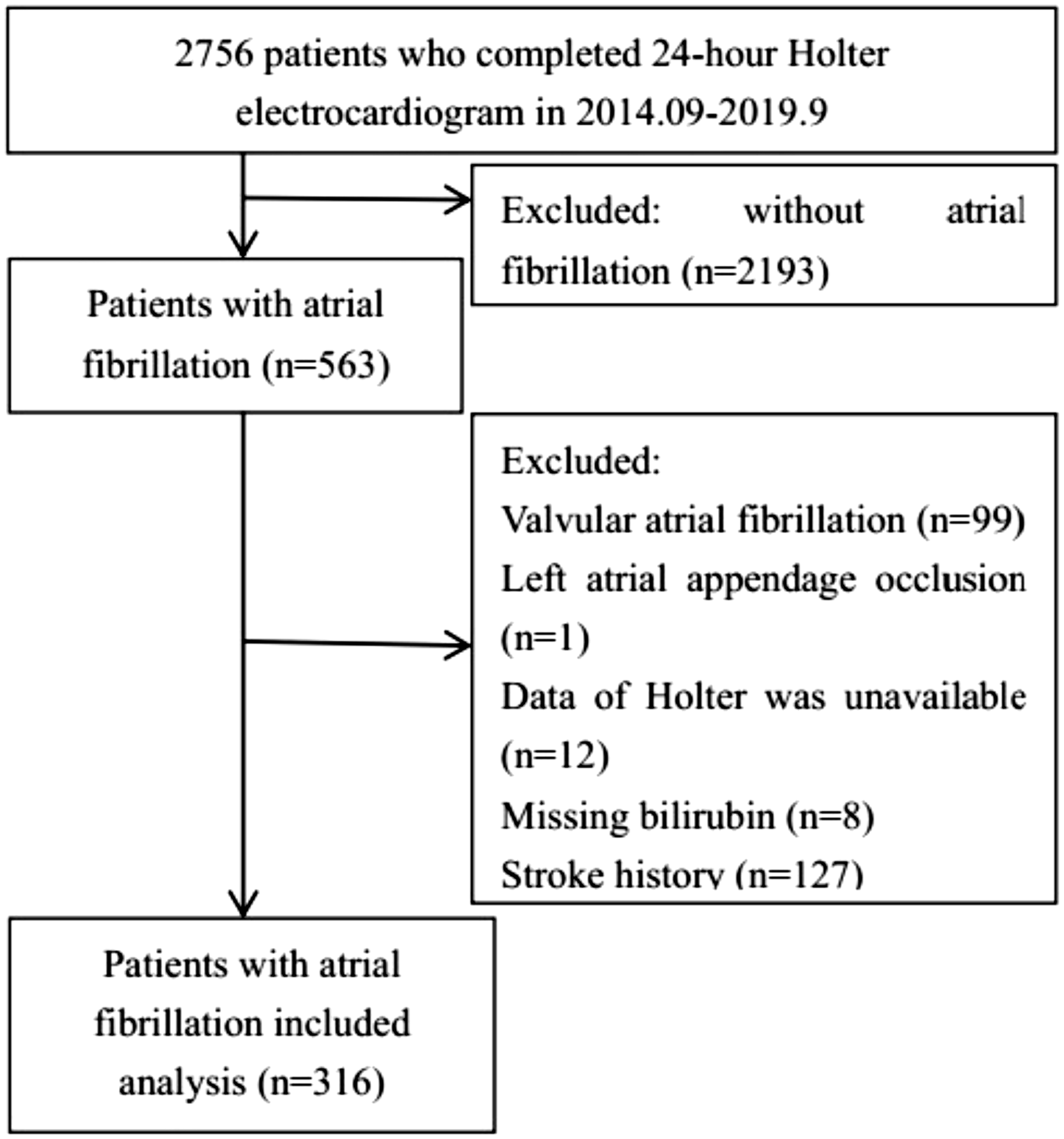
Flow chart of selection of the patients.
Assessment of atrial fibrillation
All patients underwent standard 24-hour Holter electrocardiographic (DMS 300-4A; DM software, Inc., Stateline, NV, USA) monitoring to detect atrial fibrillation. An experienced professional cardiologist who had no information about the characteristics of the patients evaluated the occurrence of atrial fibrillation on the basis of records of the 24-hour Holter electrocardiogram. Atrial fibrillation was defined as an irregular atrial rhythm with a rate of > 300 beats/minute lasting longer than 30 s. Non-sustained ventricular tachycardia was defined as a ventricular rhythm of > 120 beats/minute lasting for ≥three beats and < 30 s. Supraventricular or ventricular tachycardia lasting < 30 s was not considered a diagnostic finding, unless a clear chronological relationship with the clinical symptoms was established.23,24 Valvular atrial fibrillation was defined as rheumatic heart valve disease and a type of atrial fibrillation after cardiac valve surgery. 25
Assessment of other confounding factors
Demographic and laboratory data of the patients were recorded. Demographic data included age, sex, race, smoking, and drinking status. A physical examination included measurement of height, weight, systolic blood pressure (SBP), and diastolic blood pressure (DBP). Laboratory data included creatinine, uric acid, total bilirubin, indirect bilirubin, direct bilirubin, total cholesterol (TC), triglyceride (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), alanine aminotransferase (AST), and aspartate aminotransferase (ALT) levels, and the international standardized ratio. We also collected the medication history (anticoagulant and antiplatelet drugs) and a history of combined diseases (e.g., stroke, hypertension, diabetes, heart failure, and coronary heart disease). The left ventricular ejection fraction (LVEF) and left atrial diameter (LAD) were measured by two-dimensional echocardiography during 1 month of the Holter register. We calculated the congestive heart failure, hypertension, age > 75 years, diabetes, and previous stroke/transient ischemic attack (CHADS) 2 score (1 point each: age [≥75 years], congestive heart failure, hypertension, and diabetes mellitus; and a history of stroke or transient ischemic attack: 2 points). The estimated glomerular filtration rate (eGFR) (mL/minute/1.73 m2) was calculated using the Chronic Kidney Disease-Modification of Diet in Renal Disease formula: 175 × (serum creatinine level)−1.234 × (age)−0.179 × (0.79 for women).
Outcome
The outcome of this study was the first ischemic stroke. All outcome events were obtained by doctors or trained nurses via telephone or outpatient follow-up until January 2020. Ischemic stroke was diagnosed by symptoms, signs, and medical image examinations. Briefly, initial ischemic stroke was confirmed by professional neurologists through a series of standardized diagnostic procedures. Diagnosis of stroke was made from hospitalization or discharge data. When the patient was hospitalized, stroke was diagnosed by a professional neurologist on the basis of a sequence of examinations, including a neurological examination, stroke-related scale assessment, and cranial computed tomographic or magnetic resonance imaging scans.26,27 When the patient was discharged from hospital, the patient’s hospitalization data were obtained during follow-up and then confirmed by the clinical event committee. The Data Monitoring Committee validated all stroke events.
Statistical analysis
Baseline variables are shown as mean ± standard deviation (continuous variables) or percentage (categorical variables) as appropriate. Levels of total bilirubin were divided into five groups (quintile [Q1]–Q5). Comparison between two groups was performed by using the Student’s t test or Mann–Whitney U test for continuous variables, and the chi-square test or Fisher’s test for categorical variables. For non-normally distributed variables, the Mann–Whitney U test with Bonferroni correction was used. One-way ANOVA was used for comparison between multiple groups.
The relationship of total bilirubin levels with the first ischemic stroke was estimated by multivariate Cox proportional hazards models. The results are presented as hazard ratios (HRs) and 95% confidence intervals (CIs), and the lowest quintile (Q1) were used as the reference. Model 1 did not have adjustment for any variables. Model 2 was adjusted for age, sex, and body mass index (BMI). Model 3 was further adjusted for SBP, the CHADS2 score, LVEF, LAD, AST, ALT, uric acid, TC, LDL-C, HDL-C, TGs, eGFR, heart failure, CAD, hypertension, diabetes, drinking, smoking, the international standardized ratio, and taking oral anticoagulants and antiplatelet drugs. The shape of the relationship between total bilirubin levels with the first ischemic stroke was examined by multivariate adjusted restricted cubic spline regression models. We also used the generalized additive model to examine the nonlinear relationship between total bilirubin levels and first ischemic stroke. 28 If a nonlinear relationship was discovered, a multivariate adjusted two-piecewise linear regression model was performed to calculate the threshold effect of total bilirubin levels on first ischemic stroke. 29 The recursive method was used to calculate the inflection point automatically. Survival analysis was also performed using Kaplan–Meier curves and the log-rank test was performed. A two-sided P < 0.05 was considered to be statistically significant. All statistical analyses were performed using R V.3.3.2 (www.r-project.org).
Results
Baseline characteristics
In this study, 316 patients with non-valvular atrial fibrillation were included (mean age: 70.36 ± 10.06 years, 135 [42.72%] men) (Table 1). New ischemic stroke occurred at a mean follow-up of 22.69 ± 16.98 months, with 42 (13.29%) ischemic strokes. Patients with ischemic stroke had significantly higher serum total bilirubin levels (P = 0.006), and a lower proportion of patients were taking antiplatelet and anticoagulant drugs (both P < 0.05) compared with patients without ischemic stroke. However, there were no significant differences in age, LVEF, LAD, levels of AST, ALT, direct bilirubin, indirect bilirubin, uric acid, TC, TGs, HDL-C, and LDL-C, eGFR, SBP, DBP, BMI, international standardized ratio, the CHADS2 score, the rates of heart failure, hypertension, diabetes, and coronary heart disease, sex, smoking, and drinking status between the two groups.
Baseline characteristics of patients with ischemic stroke and non-ischemic stroke among those with non-valvular atrial fibrillation.

Data are shown as mean ± standard deviation or number (%).
LVEF, left ventricular ejection fraction; LAD, left atrial diameter; AST, alanine aminotransferase; ALT, aspartate aminotransferase; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; TGs, triglycerides; SBP, systolic blood pressure; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; BMI, body mass index; INR, international standardized ratio; CHADS2, congestive heart failure, hypertension, age > 75 years, diabetes, and previous stroke/transient ischemic attack; CAD, coronary heart disease.
When the levels of total serum bilirubin were divided into quintiles (Q1–Q5), from the first to the fifth quintiles, the incidence of initial ischemic stroke was 9 (14.29%), 7 (11.11%), 6 (9.38%), 8 (12.90%), and 12 (18.75%) (P = 0.028), respectively (Table 2). Among the five groups (Q1–Q5), there were significant differences in the LVEF, LAD, direct bilirubin levels, indirect bilirubin levels, the international standardized ratio, and the CHADS2 score (all P < 0.05).
Baseline characteristics of the quintile groups of total bilirubin levels.

Data are shown as mean ± standard deviation or number (%).One-way ANOVA, the Kruskal–Wallis rank sum test, Fisher’s test and the chi-square test were used for analysis.
Q, quintile; LVEF, left ventricular ejection fraction; LAD, left atrial diameter; AST, alanine aminotransferase; ALT, aspartate aminotransferase; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; TGs, triglycerides; SBP, systolic blood pressure; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; BMI, body mass index; INR, international standardized ratio; CHADS2, congestive heart failure, hypertension, age > 75 years, diabetes, and previous stroke/transient ischemic attack; CAD, coronary heart disease.
Relationship between total bilirubin levels and first ischemic stroke
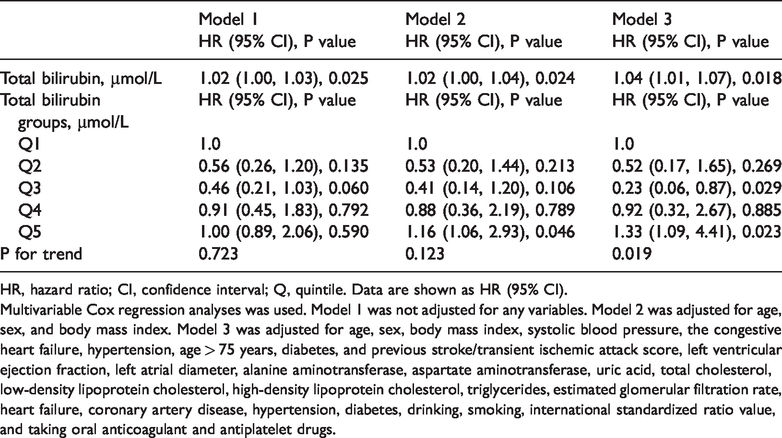
When total serum bilirubin levels were regarded as a continuous variable, in Model 1, total bilirubin levels were significantly associated with the initial ischemic stroke (HR = 1.02, 95% CI: 1.00, 1.03; P = 0.025) (Table 3). In Model 3, multivariate Cox proportional hazards analysis showed that total bilirubin levels (HR: 1.04, 95% CI: 1.01, 1.07, P = 0.018) were still an independent risk factor for initial ischemic stroke after adjustment for many factors. Additionally, when total serum bilirubin levels were regarded as a category variable with the first quintile (Q1) as a reference, the risks of first ischemic stroke were 0.52 (95% CI: 0.17, 1.65), 0.23 (95% CI: 0.06, 0.87), 0.92 (95% CI: 0.32, 2.67) and 1.33 (95%CI: 1.09, 4.41) (P for tend = 0.019) from Q2 to Q5, respectively, after adjusting for multiple potential confounders. The Kaplan–Meier survival curve showed that there was a significant difference in the occurrence of first ischemic stroke from Q1 to Q5 based on serum total bilirubin levels (log-rank, P < 0.001) (Figure 2).
Multivariable Cox regression analyses between total bilirubin levels and ischemic stroke.
HR, hazard ratio; CI, confidence interval; Q, quintile. Data are shown as HR (95% CI).
Multivariable Cox regression analyses was used. Model 1 was not adjusted for any variables. Model 2 was adjusted for age, sex, and body mass index. Model 3 was adjusted for age, sex, body mass index, systolic blood pressure, the congestive heart failure, hypertension, age > 75 years, diabetes, and previous stroke/transient ischemic attack score, left ventricular ejection fraction, left atrial diameter, alanine aminotransferase, aspartate aminotransferase, uric acid, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, estimated glomerular filtration rate, heart failure, coronary artery disease, hypertension, diabetes, drinking, smoking, international standardized ratio value, and taking oral anticoagulant and antiplatelet drugs.
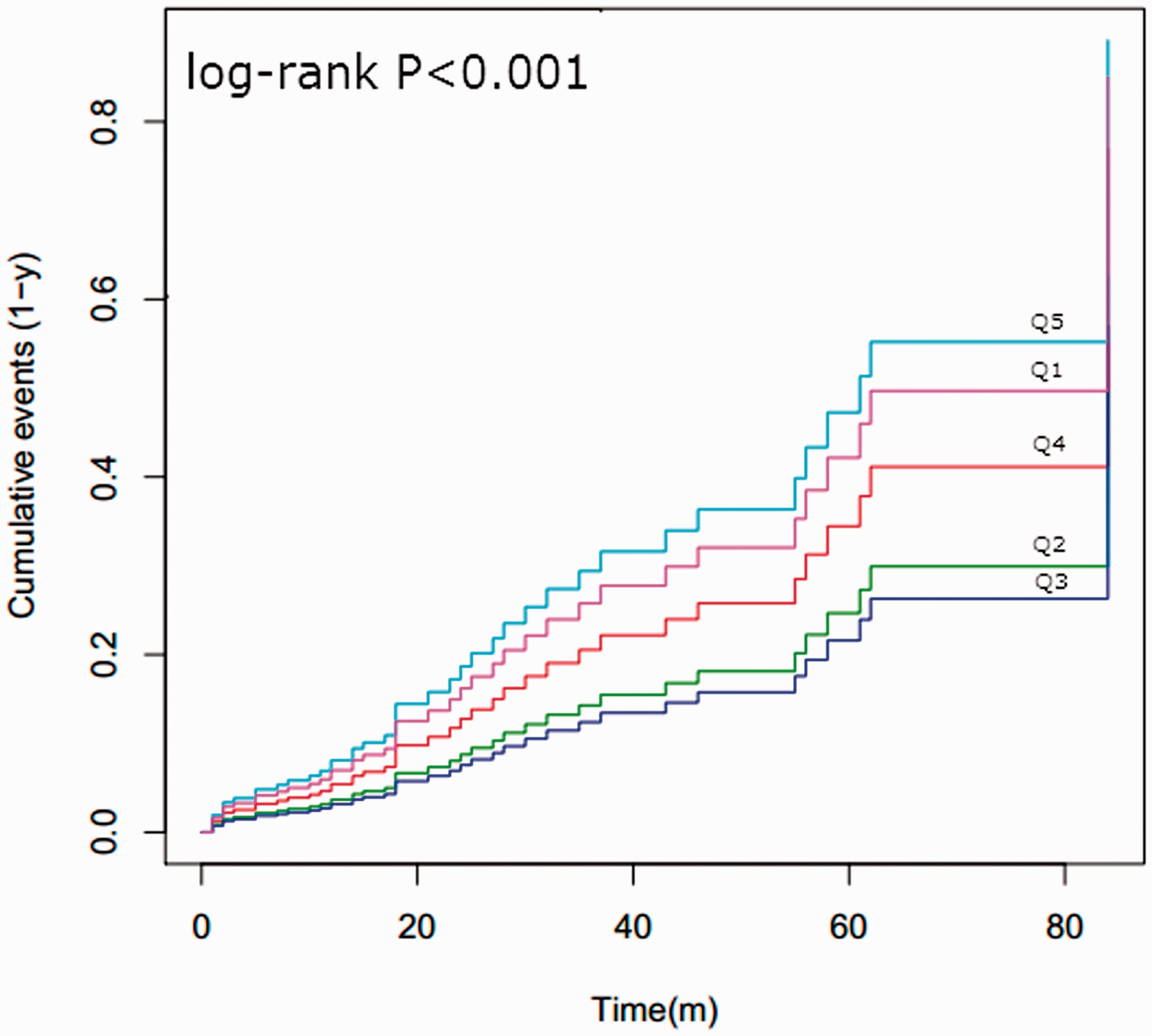
Kaplan–Meier curve of serum total bilirubin levels and initial ischemic stroke.
Multivariate adjusted smoothing spline plots showed that serum total bilirubin levels had a nonlinear relationship with first ischemic stroke. The risk of first ischemic stroke was the lowest when the serum total bilirubin level was 17.0 µmol/L (Figure 3). We further examined the association between serum total bilirubin levels and the first ischemic stroke using the Cox proportional hazards model and the two-piecewise Cox proportional hazards model. The inflection point that we identified for serum total bilirubin levels was approximately 17.0 µmol/L. When serum total bilirubin levels were < 17.0 µmol/L, although increased total bilirubin levels were significantly associated with a reduced risk of first ischemic stroke, they were not significantly associated with an increased risk of first ischemic stroke in two-piecewise linear regression (HR: 0.87, 95% CI: 0.73, 1.02) (Table 4). However, when serum total bilirubin levels were ≥17.0 µmol/L, they were significantly associated with an increased risk of first ischemic stroke (HR: 1.05, 95% CI: 1.01, 1.08, P = 0.005).

Multivariate adjusted restrictive cubic curve of serum total bilirubin levels and initial ischemic stroke.
Results of the two-piecewise linear regression model between total bilirubin levels and ischemic stroke.

HR, hazard ratio; CI, confidence interval. The generalized additive model and two-piecewise linear regression model were used for analysis.
Variables included in the regression model were age, sex, body mass index, systolic blood pressure, the congestive heart failure, hypertension, age > 75 years, diabetes, and previous stroke/transient ischemic attack score, left ventricular ejection fraction, left atrial diameter, alanine aminotransferase, aspartate aminotransferase, uric acid, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, estimated glomerular filtration rate, heart failure, coronary artery disease, hypertension, diabetes, drinking, smoking, international standardized ratio value, and taking oral anticoagulant and antiplatelet drugs.
Discussion
In this retrospective single-center study, we found that in patients with non-valvular atrial fibrillation, those with ischemic stroke had higher serum total bilirubin levels compared with non-ischemic stroke patients. Serum total bilirubin levels were closely related to initial ischemic stroke, and may be an independent risk factor for ischemic stroke. Importantly, serum total bilirubin levels had a dose-independent relationship with initial ischemic stroke, which suggested that when total bilirubin levels were ≥17.0 µmol/L, the risk of ischemic stroke significantly increased.
Previous studies have indicated that there is a significant relationship between serum bilirubin levels and stroke.15,16 Importantly, we found a dose-dependent relationship between total bilirubin levels and ischemic stroke. We found that when bilirubin levels were < 17 µmol/L, they may be a protective factor for stroke. The results of our study are similar to previous studies, which showed that serum total bilirubin levels were inversely related to stroke.15,16 These findings suggest that low total bilirubin levels may have a protective effect on prevention and treatment of stroke. Additionally, the National Health and Nutrition Examination Survey 1999 to 2004 suggested that higher serum total bilirubin levels were associated with a reduced prevalence of stroke and improved stroke outcomes. 30 This finding supports the hypothesis that bilirubin is a protective biomarker for stroke. A prospective study from Korea showed that the serum bilirubin level might have some protective function against the risk of stroke in the Korean population. 31 However, we found that when serum total bilirubin levels were ≥17 µmol/L, for each 1 unit increase in the total bilirubin level, the risk of stroke increased by 5%. This finding indicated that the total bilirubin level was an independent risk factor for stroke. This finding suggests that high total bilirubin levels may damage blood vessels or tissues, and may be detrimental to the occurrence of stroke. Ayromlou et al. 32 showed that when total bilirubin levels were high in the circulation, they could become highly toxic. This finding suggests that an increased level of bilirubin is associated with the severity of stroke and ischemic area. We speculate that the reasons for the difference between the results of our study and most previous studies may be as follows. One reason is that the study population was different among the studies because enrolled subjects in our study had atrial fibrillation and most of the previous studies were on the general population. Another reason is that the analysis methods were different between studies. In our study, not only correlation of multivariate Cox regression analysis was carried out, but also non-linear analysis was performed to examine the cut-off value of bilirubin and occurrence of stroke.
Although bilirubin plays a vital role in development of stroke and may be related to stroke, its mechanism is still unclear. Bilirubin can prevent formation of atherosclerotic lesions in low-density lipoprotein receptor-deficient mice by inhibiting endothelial vascular cell adhesion molecule 1 and intercellular adhesion molecule 1-mediated leukocyte migration. 33 A previous study showed that bilirubin inhibited smooth muscle cell proliferation by regulating growth factor activity. 34 Collectively, the potential biological mechanisms of bilirubin during stroke mainly include regulation of lipid oxidation, lipid metabolism, immune cell migration, anti-inflammation and proliferation of vascular cells.35,36 In the future, more basic research is required to clarify the possible mechanisms and roles of circulating bilirubin levels in relation to stroke.
Limitations
This study has some limitations. First, the diagnosis of atrial fibrillation in this study was from 24-hour Holter monitoring. Therefore, some patients with paroxysmal atrial fibrillation and a history of atrial fibrillation may have been excluded. Second, some baseline variables, such as smoking, alcohol consumption, medication history, and a history of comorbidity, were mainly obtained from patients’ self-reports. Therefore, there was a reporting bias. Third, although most of the confounding factors related to stroke were adjusted for, other variables, such as the duration of atrial fibrillation, cystatin C, exercise, inflammation biomarkers, and sleep, were missing in this study. Additionally, data on stroke-related scores, the severity of stroke, imaging results, and the time and regularity of taking anticoagulant or antiplatelet drugs were not collected. Finally, because this study was in a single center with small number of samples, the results cannot be extrapolated.
Conclusion
In patients with non-valvular atrial fibrillation, serum total bilirubin levels are an independent risk factor for initial ischemic stroke, and there is a nonlinear relationship between them. The risk of ischemic stroke is lowest when the total bilirubin level is approximately 17.0 µmol/L. Our research indicates that serum total bilirubin levels may contribute to the risk stratification of atrial fibrillation and detection of bilirubin levels may have a vital role in early warning of ischemic stroke. Furthermore, there is the potential for total bilirubin to serve as a therapeutic target for oxidative stress-related diseases, such as ischemic stroke.
Footnotes
Author contributions
Ying Liu drafted the manuscript. Jie Wang and Wen-zhen Zeng helped with statistical analysis. Qing-shan Lyu and Ying Liu participated in the design of the study. Jie Wang, Wen-zhen Zeng, and Qing-shan Lyu revised the manuscript. Ying Liu, Jie Wang, Wen-zhen Zeng, and Qing-shan Lyu participated in data collection. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by the Natural Science Foundation of Hunan Province (grant number: 2018JJ6079) and the Scientific Research Project of Hunan Health and Family Planning Commission (grant number: B20180462).