
Abstract
Patients with rheumatoid arthritis (RA) taking long-term immunosuppressive drugs are more susceptible to opportunistic infections, such as cryptococcosis. A 65-year-old woman was transferred to our hospital for rapidly progressing pulmonary lesions identified by lung computed tomography. She had a 7-year history of RA and had been prescribed methotrexate and glucocorticoids for 10 months. Additionally, our patient had a history of environmental exposure to house renovation lasting approximately 1 week before onset. Her serological test results and histopathological examination confirmed the diagnosis of pulmonary cryptococcosis (PC). The patient recovered well after 6 months of fluconazole treatment. In addition, we summarized 28 reported cases of RA patients with PC and found that older age might be a risk factor for cryptococcal infection in RA patients. The most common location for pulmonary lesions was the lower lobe, and the most common radiologic manifestations were nodules. Detection of cryptococcal capsular polysaccharide antigen was important for diagnosis. Patients undergoing antirheumatic therapy should avoid exposure to Cryptococcus.
Keywords
Introduction
Cryptococcus is an encapsulated fungus found in soil, decaying wood, rotten food, and the feces of birds, especially pigeons. Fungal contamination also occurs in living areas.1,2 Pulmonary cryptococcosis (PC) is considered an opportunistic infection that occurs through inhalation of cryptococcal spores into the lung. It is more common in people with acquired immunodeficiency syndrome and other immunocompromised patients and less common in immunocompetent individuals.2,3 Here, we report a case of possible environmental exposure-associated PC in a patient with RA receiving methotrexate (MTX) and glucocorticoids (GCs). Moreover, we summarized 28 reported cases of RA with PC, including patient demographics, symptoms, radiology, laboratory examination, treatment, and outcomes.
Case report
Our patient was a 65-year-old woman with a 7-year history of RA who had been treated with methylprednisolone (2 mg, every other day) and MTX (10 mg/week) for 10 months. She developed a fever of 38°C and a paroxysmal cough with copious amounts of white sputum. Chest computed tomography (CT) showed nodular and patchy infiltration in the left lower, right middle, and right lower lung fields (Figure 1a). Following 1 week of antibiotic treatment, the patient’s cough and fever improved. However, her radiographic findings worsened, with lung CT depicting multiple invasive lesions in the right middle and bilateral lower lung fields (Figure 1b). Thus, she was admitted to a local hospital and prescribed amoxicillin/clavulanate potassium (2.4 g/day) combined with levofloxacin (0.5 g/day). However, re-examination by CT after 10 days revealed bilateral airspace consolidation and multiple nodules (Figure 1c). Therefore, the patient was transferred to our department because of the rapidly progressing pulmonary lesions. She had no history of smoking or alcohol abuse but she had a history of environmental exposure to house renovation lasting approximately 1 week before onset. Her vital signs were stable. Moist rales were audible in both lung bases. She was treated with cefoxitin 2.0 g intravenously twice daily from the first day, and methylprednisolone (40 mg/day) was added beginning on day 2 after admission. Laboratory findings were as follows: leukocytes, 6400/µL (78.8% neutrophils, 13.4% lymphocytes, 0.8% eosinophils, 0.2% basophils, 6.8% monocytes); hemoglobin, 115 g/L; hematocrit, 37.5%; platelets, 19.5 × 104/µL; total protein, 57.5 g/L; albumin, 33.9 g/L; globulin, 23.6 g/L; serum calcium, 1.88 mmol/L; and fasting blood glucose, 3.43 mmol/L. Serum procalcitonin, C-reactive protein (CRP), rheumatoid factor, immunoglobulins, complements, tumor markers, anti-myeloperoxidase, anti-proteinase 3, antinuclear antibody, and liver and kidney functions were normal. Serological tests showed negative results for human immunodeficiency virus, Aspergillus fumigatus, and respiratory viruses. However, lung CT scans demonstrated no significant improvement after empirical treatment (Figure 1d). Serological tests revealed a positive result for cryptococcal capsular polysaccharide antigen (CrAg) (CrAg Lateral Flow Assay, IMMY Co., Norman, OK, USA). More importantly, a left lung biopsy confirmed granulomatous inflammation. Special histochemical staining showed acid-fast negative, periodic acid-Schiff (PAS) positive, Gomori methenamine silver (GMS) positive and mucicarmine positive, suggesting a cryptococcal infection (Figure 2). In addition, a lumbar puncture revealed no abnormal findings, and the titer of cryptococcal antigen was negative. The patient then received fluconazole treatment. Two weeks later, follow-up radiographic findings showed that the lesions had partially disappeared (Figure 1e). Six months later, a lung CT scan showed that the lesions had almost completely disappeared (Figure 1f). The patient gave informed consent for publication of this case report.
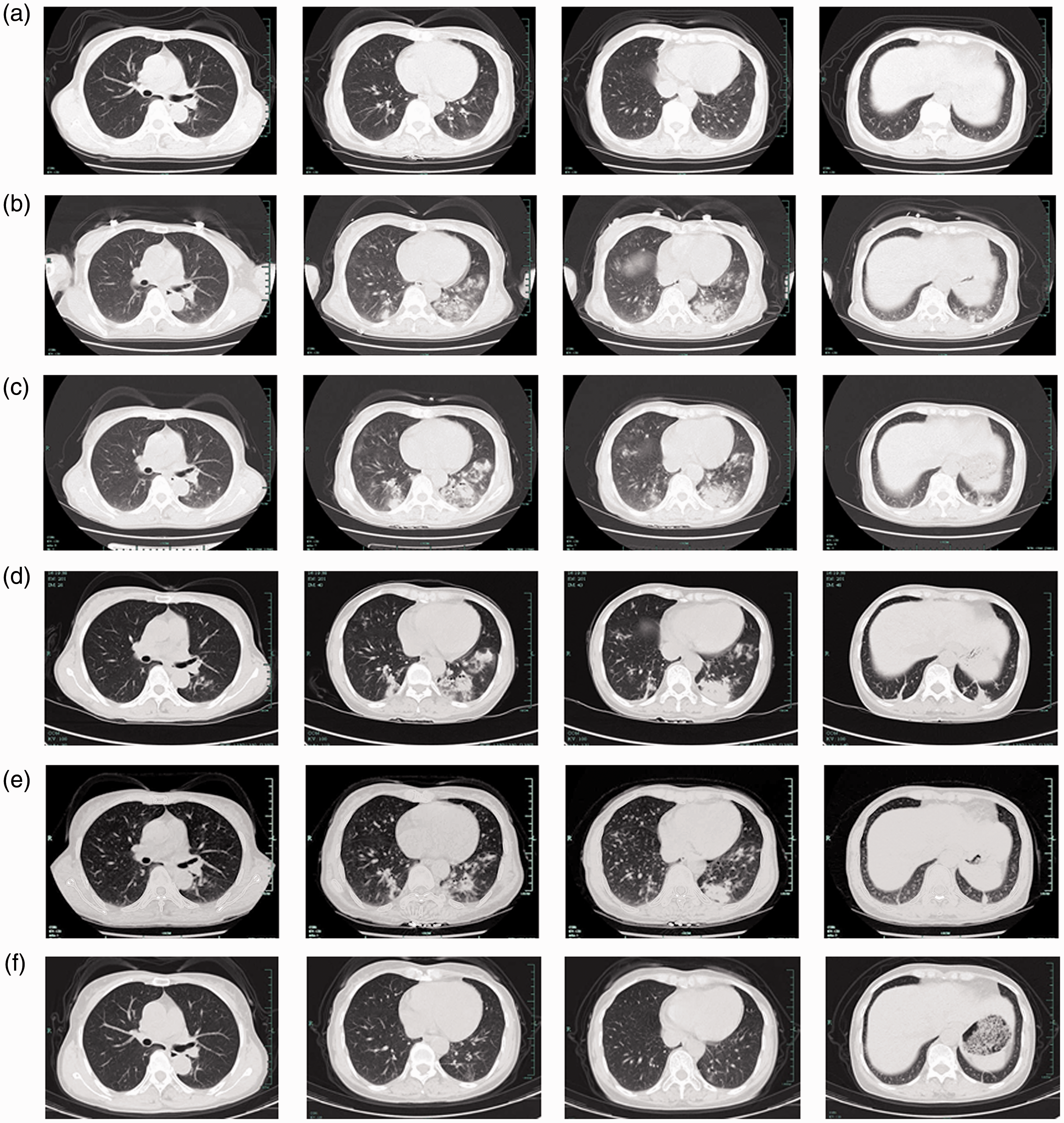
Timeline of the patient’s lung computed tomography (CT) scan: (a) 8 April 2018, (b) 18 April 2018, (c) 27 April 2018, (d) 5 May 2018, (e) 24 May 2018, and (f) 5 December 2018.
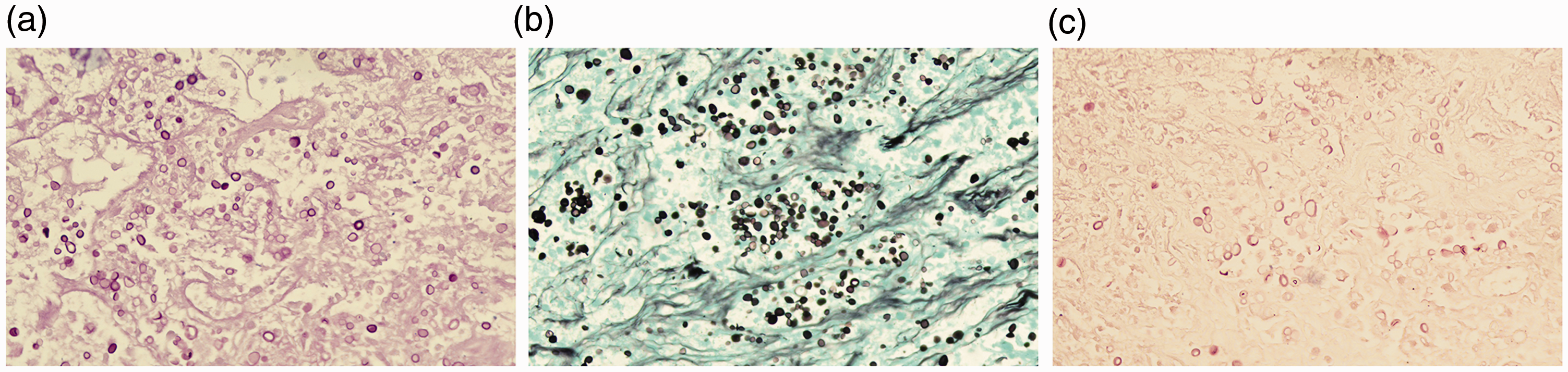
Histopathological staining of specimen by lung biopsy revealed cryptococcal organisms: (a) periodic acid-Schiff (PAS), 400×, (b) Gomori methenamine silver (GMS), 400×, and (c) mucicarmine, 400×.
Discussion
The present case describes a patient with RA on a methylprednisolone and MTX treatment regimen who suffered from PC after exposure to 1 week of house renovation. PC is an important opportunistic infection that is more likely to occur in individuals in immunocompromised states, such as patients with acquired immunodeficiency syndrome, malignancy, or organ transplantation. 3 As in the present case, PC can also develop as a complication of RA. The increased risk of cryptococcal infection in RA patients may be associated with the disease itself because of the intrinsic alteration in cellular immunity. 4 Moreover, the drugs used to treat RA likely play a crucial role in the development of severe infections. MTX, an antimetabolite drug that interferes with synthesis of DNA and certain amino acids by inhibiting dihydrofolate reductase, has a profound immunosuppressive effect, suppressing both the number and function of phagocytes and lymphocytes, as well as antibody production.4,5 Furthermore, MTX itself has pulmonary toxicity and increases the chance of bacterial and opportunistic infections. 6 GCs have broad immune-suppressing and anti-inflammatory effects that change the distribution and impair the function of lymphocytes, monocytes, and neutrophils; these changes are associated with suppressed cell-mediated immunity that results in an increased susceptibility to cryptococcal infection.4,5
We summarize 28 reported cases of patients with RA and PC, including our case, in Table 1.7–23 There were 21 female and 7 male patients aged from 47 to 83 years (median age 65 years). It is worth noting that nearly two-thirds of patients (67.9%, 19/28) were older than 60 years, indicating that older age may be a risk factor for cryptococcal infection in RA patients and that infection occurred predominantly in female patients (75.0%, 21/28). Duration of RA ranged from 3 months to 20 years according to the data available, and 17 of the patients (73.9%, 17/23) had a history of RA for more than 1 year. The treatment regimen of RA patients whose data were reported was as follows: 23 of 27 patients (85.2%) had received GCs including prednisolone and triamcinolone, and 16 of 27 patients (59.3%) had received MTX. Twenty patients (71.4%) received more than 2 drugs. Therefore, GCs and MTX are the predominant reported medications for patients with RA and PC. Twelve patients (41.4%) were asymptomatic, and the remaining 16 patients presented with flu-like symptoms. The most common clinical features were cough (62.5%, 10/16) and fever (56.3%, 9/16); others included hemoptysis (6.3%, 1/16), weakness (6.3%, 1/16), anorexia (6.3%, 1/16), weight loss (12.5%, 2/16), dyspnea (25.0%, 4/16), sputum (12.5%, 2/16), frontal headache (6.3%, 1/16), and chest pain (6.3%, 1/16). We found that the white blood cell count or CRP were elevated in almost all patients with clinical symptoms. Twenty-seven patients underwent lung CT scans. The most common location of lesions was the lower lobe (51.9%, 14/27). Nodules were the most common radiological finding, being observed in 16 patients (61.5%); the second and third most common radiological abnormalities were consolidation (30.8%, 8/26) and cavities (26.9%, 7/26). Our results were in agreement with those of previous studies on the radiographic characteristics of RA patients with PC.24–27 Serology, histopathology, and mycological culture play important roles in the diagnosis of PC. Twenty-five patients had at least one of the following conditions: serum CrAg or positive culture, bronchoalveolar lavage (BAL) CrAg or positive culture, or Cryptococcus-positive histopathology. Among these patients, the histopathological results all revealed cryptococcal granuloma. Eleven of 14 patients (78.6%) had a positive serum CrAg test, 6 of 8 patients had a positive bronchoalveolar lavage fluid (BALF) CrAg test, and 2 patients had positive CrAg tests for both serum and BALF. Half of the patients (50%, 7/14) were treated with fluconazole monotherapy, 6 patients (42.9%, 6/14) received combination antifungal therapy, and 1 patient recovered without the use of any further antifungal agents. All patients (100%, 15/15) recovered after treatment.
Summary of 28 cases of patients with rheumatoid arthritis (RA) and pulmonary cryptococcosis.

Adal, adalimumab; AMB, amphotericin-B; BAL, bronchoalveolar lavage; CrAg: cryptococcal capsular polysaccharide antigen; CRP, C-reactive protein; CsA, cyclosporine; d, day; 5-FC, flucytosine; FCZ, fluconazole; Flagyl, metronidazole; GCs, glucocorticosteroid; HXQ, hydroxychloroquine; LEF, leflunomide; Infl, infliximab; MCZ, miconazole; MINO, minocycline; MTX, methotrexate; PSL, prednisolone; PTLB, percutaneous lung biopsy; SASP, salazosulfapyridine; TBLB, transbronchial lung biopsy; VATS, video-assisted thoracoscopic surgery; w, week; WBC, white blood cell; WL, weight loss.
As reported in this case, an RA patient in an immunocompromised state received repeated antibiotic treatment for bacterial pneumonia for 24 days, and her cough and fever improved. However, lung CT findings showed rapid development of bilateral infiltration. Fortunately, after the diagnosis of PC and initiation of antifungal therapy, her condition gradually improved. This case revealed the importance of reassessing the causative pathogen when the initial anti-infection treatment fails.
It is noteworthy that our patient reported a history of house renovation approximately 1 week before suffering from PC. In the cases we summarized, one patient seemed to have acquired cryptococcal infection from aerosolized excreta while cleaning his cockatiel’s cage, and another patient’s infection may have been related to heavy contamination of her living surroundings with pigeon droppings.16,17 Moreover, it has been reported that dust in the home environment also carries the potential for Cryptococcus contamination. 28 Although we failed to identify dust in the patient’s home environment carrying Cryptococcus contamination, and serological tests for her family members were negative for CrAg, we could not exclude the possibility that our patient acquired a cryptococcal infection while renovating her house. Therefore, exposure to contaminated environments should be avoided for immunocompromised individuals.
In summary, this case contributes to the list of cases of PC associated with patients with RA on MTX and GC treatment regimens. Furthermore, our case report suggests the following important findings in clinical work: RA patients may develop opportunistic fungal infections during immunosuppressive therapy. History of house renovation may be related to cryptococcal infection of an immunocompromised RA patient, so clinicians should ask about occupational and environmental exposure history.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by Zhejiang Provincial Natural Science Foundation (No: LY18H160016) and Project of Health and Family Planning Commission of Zhejiang Province, China (No: 2019C03042).