
Abstract
Most intraocular metastases are detected in the choroid, iris, ciliary body, or retina. Conversely, tumors rarely metastasize to the optic disc, and they even less frequently present as the initial sign of cancer. In this study, we presented the case of a patient who first visited the ophthalmology department because of gradual visual impairment without any systemic symptoms, and she was ultimately diagnosed with non-small-cell lung cancer. This case report illustrated that visual impairment may be the first sign of non-small-cell lung cancer; therefore, we should not neglect ocular metastasis even when the patient has no systemic symptoms on her/his first visit to the ophthalmology department.
Introduction
Metastatic tumors in the optic disc are extremely rare. Most intraocular metastases are detected in the choroid (88%), iris (9%), or ciliary body (2%), and less than 1% of these lesions are detected in the retina. 1 In this study, we discussed the case of a patient who first presented to our department with optic disc metastasis as the initial sign of non-small-cell lung cancer.
Case report
A 57-year-old woman was referred to our hospital on July 16, 2017 for gradual visual impairment in her right eye without any systemic symptom such as cough, chest pain, or fever. Her medical and family histories were unremarkable. On examination, her best-corrected visual acuities (BCVAs) were 20/400 in the right eye and 20/20 in the left eye. A relative afferent pupillary defect was detected in her right eye. No other abnormality was noted in the anterior segment of the eye. Funduscopy revealed irregular yellow-white thickening of the optic disc with venous congestion (Figure 1a). Fluorescein fundus angiography disclosed hyperfluorescence of the optic disc together with abnormal extension of the adjacent capillaries in the arterial and early venous phases (Figure 1c). B-scan ultrasonography revealed elevation of the optic disc together with high reflectivity of the adjacent vitreous body in the right eye (Figure 1d). In addition, optic coherence tomography revealed retinal detachment and numerous high-reflective dots in the sub-retinal space (Figure 1e). Because of worsening of her BCVA, the patient underwent computed tomography (CT) of the chest and magnetic resonance imaging (MRI) scan of the brain to exclude systemic diseases. Surprisingly, CT uncovered a large lobulated mass (55 × 35 mm2) in the apex of the left lung. Small metastatic lesions were observed in the right frontal and left occipital lobes of the brain on MRI; however, no metastasis to the intraorbital or intracranial optic nerve was noted on MRI. Bronchoscopy biopsy demonstrated that the lesion was adenocarcinoma, a sub-type of non-small-cell lung carcinoma. Then, she received chemotherapy with carboplatin and pemetrexed in the thoracic tumor department at other general hospital for 20 months. However, the patient did not visit any ophthalmologist during chemotherapy. She returned to our eye hospital after chemotherapy after complaining of vision loss. On examination, her visual acuity was no light perception, and severe cataract was found in her right eye (Figure 2a). Ultrasonography demonstrated that the tumor metastasized to the vitreous body (Figure 2b). However, the condition of the patient was too poor to permit ophthalmic surgery or radiotherapy. The patient died of multiple organ failure 25 months after chemotherapy.
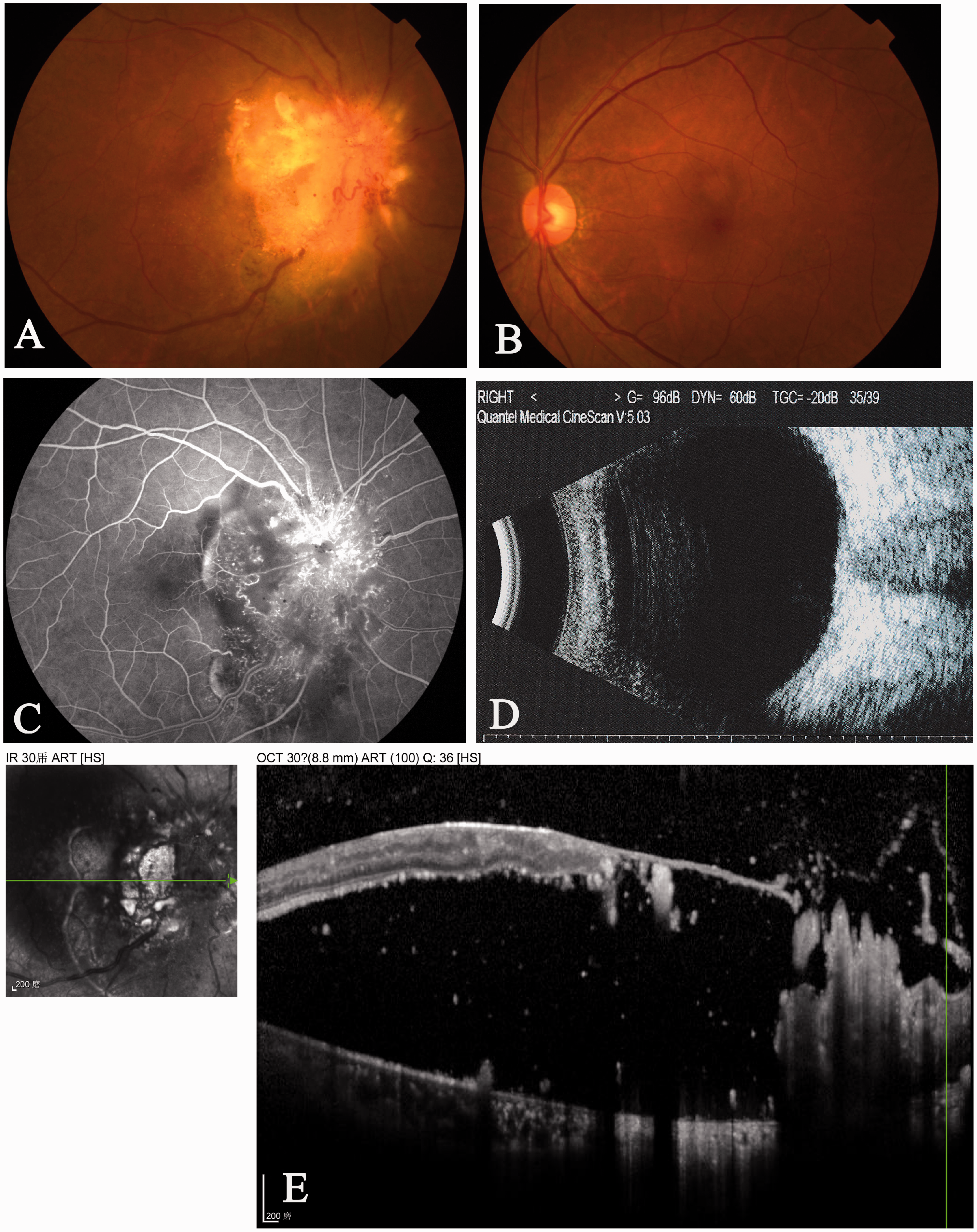
Optic disc metastasis in the right eye of a 57-year-old woman with non-small-cell lung cancer. (a) Color fundus photography revealed irregular yellow-white thickening of the optic disc as well as venous congestion. (b) Color fundus photography uncovered no metastasis in the left eye. (c) Fundus fluorescein angiography highlighted the hyperfluorescence of the optic disc together with abnormal extension of the adjacent capillaries in the arterial and early venous phases. (d) B-scan ultrasonography revealed elevation of the optic disc together with high reflectivity of the adjacent vitreous body in the right eye. (e) Detachment of the retina and numerous high reflective dots in the sub-retinal space were observed via optic coherence tomography.

Follow-up 20 months after chemotherapy with carboplatin and pemetrexed. (a) The patient developed cataract in her right eye. (b) Ultrasonography revealed that the tumor likely metastasized to the vitreous body.
Discussion
Most intraocular metastases arise in the uveal tract. 2 To our knowledge, metastatic tumors in the optic disc are extremely rare, and few case reports have been published.3–14 Previously published studies on involving optic disc metastasis are listed in Table 1. Specifically, in these published cases, the diagnosis of optic disc metastasis was easily established because all patients already had a clear history of primary tumors (Table 1). Differing from most previously published papers, the patient in this case report presented with visual impairment because of optic disc metastasis as the first sign before the diagnosis of cancer, which might be misdiagnosed as infectious or inflammatory retinitis. 1 Interestingly, MRI of the affected eye illustrated that no intraorbital or intracranial optic nerve was involved, suggesting that the lesion was an isolated optic nerve head metastasis. In fact, with the development of multimodal imaging, ophthalmologists can easily identify optic disc metastasis. This case report reminds ophthalmologists to consider ocular metastasis even when the patient has no systemic symptoms on her/his first visit to the ophthalmology department.
A summary of previously published studies involving optic disc metastasis.

Footnotes
Authors’ contributions
KL contributed to the conduct of the study, data collection, data analysis, and manuscript writing. LL and YG contributed to patient followup and data acquisition. CJ contributed to the design of the study, data interpretation, and manuscript revision. All authors have read and approved the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
This case report was approved by the Institutional Review Board of Sun Yat-sen University and conducted in accordance with the tenets of the Declaration of Helsinki. Written informed consent was obtained from the patient.
Funding
This study was supported by grants from Project 5010 of Clinical Research of Sun Yat-sen University (2013007), Key Projects of Guangzhou Science and Technology Plan (201707020008), National Natural Science Foundation of China (81670866, 81600741), Fundamental Research Funds for the Central Universities (Sun Yat-sen University, 19ykpy152), the Natural Science Foundation of Guangdong Province (2020A1515011099), and Basic Research Plan of Guangzhou Science and Technology Plan Project (202002030380). The funding sponsors had no roles in the design of the study; collection, analysis, and interpretation of data; or drafting of the manuscript.