
Abstract
Objective
We aimed to investigate risk factors related to remnant gallbladder (RGB) stones.
Methods
This retrospective study included 73 patients with RGB, in groups with and without RGB calculi. Univariate analyses were used to identify nine variables associated with RGB calculi: sex, age, body mass index (BMI), time to detection, surgical method, length of RGB, angle of RGB and common hepatic duct (CHD), choledocholithiasis, and remnant cholecystitis. Multivariate logistic regression was performed to assess independent predictors of RGB stones. A receiver operating characteristic (ROC) curve was used to estimate model accuracy and determine cut-off values of independent predictors.
Results
We enrolled 73 patients, 33 with and 40 without RGB stones. Univariate analyses showed that age, BMI, time to detection, length of RGB, angle of RGB and CHD were predictors for RGB calculi. Multivariate analyses indicated that time to detection, length of RGB, and angle of RGB and CHD were independent predictors for RGB calculi. The area under the ROC curve of the model was 0.940. Cut-off values of the three indicators were 1.5 years, 2.25 cm, and 22.5°, respectively.
Conclusion
Time to detection, length of RGB, and angle of RGB and CHD were independent predictors of RGB calculi.
Introduction
In approximately 20% of patients, gallstones remain symptomatic, as in biliary colic; for these cases, laparoscopic cholecystectomy (LC) is the preferred treatment.1–3 Although cholecystectomy relieves symptoms of gallstone disease in 85% of cases, the remaining 7% to 15% of patients continue to have similar symptoms after surgery, called post-cholecystectomy syndrome (PCS). 4 , 5 PCS can occur owing to cystic duct stump calculi or gallbladder remnant calculi, 4 , 6 which have recently attracted the attention of surgeons.
To our knowledge, no clinical studies have focused on factors related to remnant gallbladder (RGB) calculi formation. Hence, the aim of this study was to investigate risk factors for RGB stones, so as to prevent the formation of lithiasis.
Materials and Methods
Patients
All consecutive patients with cholecystolithiasis between January 2013 and December 2019 in Shandong Provincial Third Hospital were extracted from a prospectively maintained database. A total of 2678 patients underwent cholecystectomy during this period. All patients received computed tomography (CT) or magnetic resonance (MR) scans within 1 week after surgery. The inclusion criteria were as follows: (I) age ≥18 years and (II) RGB formed after LC or open cholecystectomy (OC). The exclusion criteria were as follows: (I) RGB combined with common bile duct (CBD) tumor, duodenal papillary tumor, or aberrant congenital biliary tract; (II) residual stones found on post-operative imaging within 1 week; and (III) incomplete clinical data. We retrospectively analyzed the clinical data of the included patients (Figure 1).

Flow chart of participants included in this research.
Research methods
Nine variables including sex, age, body mass index (BMI), surgical method (LC or OC), time to detection (time interval between cholecystectomy and diagnosis of RGB or RGB lithiasis), length of RGB, angle of RGB and common hepatic duct (CHD), choledocholithiasis, and remnant cholecystitis were recorded. Information of patients’ sex, age, BMI, time to detection, and surgical approach was collected by reviewing the medical records; the remaining variables were obtained from CT or MR images. A 128-row CT scanner (Brilliance iCT, Philips Medical Systems Best, The Netherlands) and a 3.0-T MR imager (Ingenia, Philips Medical Systems Best) were used in this study. All CT and MR images were reconstructed using Philips Extended Brilliance Workspace v. 4.5 (Philips Medical Systems Best) and independently assessed by two experienced radiologists with 10 and 15 years of experience in abdominal imaging diagnosis. Differences were resolved in discussions until consensus was reached. The following four indicators were selected: length of RGB (the longest diameter of RGB by selecting the maximum section in axial or coronal images) (Figure 2a, 2b), angle of RGB and CHD (the angle between the length of RGB and CHD in coronal images or magnetic resonance cholangiopancreatography [MRCP]) (Figure 2c, 2d), choledocholithiasis, and remnant cholecystitis (wall thickness ≥3 mm, mucosal hyperenhancement, high attenuation of bile, pericholecystic fat stranding and fluid). 7

(a) Computed tomography (CT) image showing length of remnant gallbladder (RGB). (b) T2-weighted imaging turbo spin-echo (T2WI-TSE) coronal measurement of RGB length. (c) CT coronal reconstruction image showing angle of RGB and common hepatic duct (CHD). (d) Magnetic resonance cholangiopancreatography (MRCP) showing angle of RGB and CHD.
Ethics approval and consent
This study was approved by the research ethics committee of Shandong Provincial Third Hospital, Cheeloo College of Medicine, Shandong University on 4 January 2013. Written informed consent was obtained from the patients for publication of this manuscript.
Statistical analysis
Statistical analyses were performed using SAS v. 9.4 statistical software package (SAS Inc, Cary, NC, USA). Univariate analyses, including the t-test or Wilcoxon rank sum test and chi-square test were used to identify variables associated with RGB calculi. After considering variables shown in univariate analysis to be significantly associated, multivariate logistic regression was performed to assess the independent predictors of RGB calculi. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated. The area under the receiver operating characteristic (ROC) curve (AUC) was used to estimate accuracy of the model and to determine the cut-off values of independent predictors. A P value < 0.05 was considered statistically significant.
Results
Data of patients
Seventy-three patients (39 men and 34 women) diagnosed with RGB were included (age 43–84 years) in the study. The 73 patients were divided into an RGB with lithiasis group (observation group, n = 33) and RGB without lithiasis group (matched group, n = 40). There were 17 men and 16 women in the observation group with average age 63.8 ± 10.9 years (range, 43–83) and a BMI 25.0 ± 2.6 kg/m2 (range, 20.7–30.7). Twenty-two men and 18 women were included in the matched group, with average age 68.9 ± 9.5 years (range, 53–84) and BMI 22.1 ± 2.5 kg/m2 (range, 19.4–28.5).
Univariate analyses
Univariate analyses showed that age (63.8 ± 10.9 years vs. 68.9 ± 9.5 years, P = 0.037), BMI (25.0 ± 2.6 kg/m2 vs. 22.1 ± 2.5 kg/m2, P < 0.001), time to detection (3.4 ± 1.7 years vs. 1.8 ± 1.5 years, P < 0.001), length of RGB (2.8 ± 1.0 cm vs. 1.9 ± 0.4 cm, P < 0.001), and angle of RGB and CHD (22.8 ± 7.4° vs. 28.1 ± 7.6°, P = 0.004) were predictors for RGB stones. However, sex, surgical method, choledocholithiasis, and remnant cholecystitis were not significantly associated with RGB calculi (Tables 1 and 2).
Quantitative data comparing observation group and matched group (x‾ ± s).
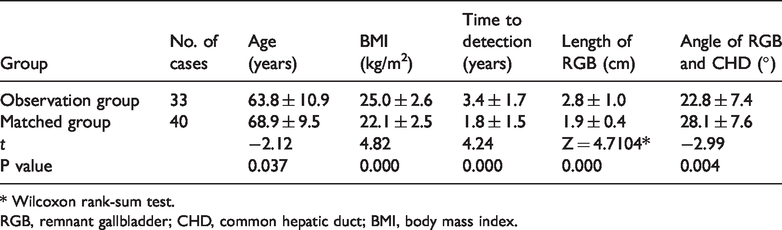
* Wilcoxon rank-sum test.
RGB, remnant gallbladder; CHD, common hepatic duct; BMI, body mass index.
Qualitative data compared between the observation group and matched group, N (%).

LC, laparoscopic cholecystectomy; OC, open cholecystectomy.
Multivariate analyses
According to the results of univariate analyses, significant variables were analyzed using multivariate logistic regression. The results showed that time to detection (OR = 2.042, 95% CI: 1.255–3.323, P = 0.004), length of RGB (OR = 9.470, 95% CI: 1.777–50.475, P = 0.009), and angle of RGB and CHD (OR = 0.851, 95% CI: 0.755–0.959, P = 0.008) were independent risk factors for RGB calculi (Table 3).
Multivariate analysis of gallbladder remnant stones.
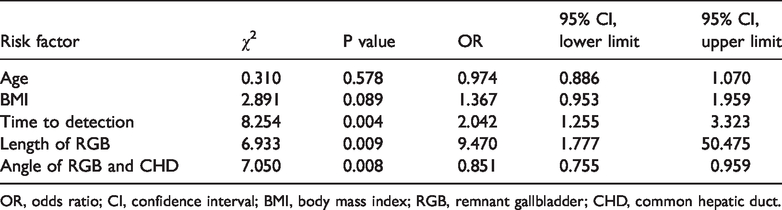
OR, odds ratio; CI, confidence interval; BMI, body mass index; RGB, remnant gallbladder; CHD, common hepatic duct.
ROC curve
ROC curve analysis indicated that the AUC of the model was 0.940, and the cut-off values for time to detection, length of RGB, and angle of RGB and CHD were 1.5 years, 2.25 cm, and 22.5°, respectively (Figure 3).

Receiver operating characteristic (ROC) curve.
Discussion
RGB means that the residual cystic duct is too long after cholecystectomy and grows to form a small gallbladder, or that a part of the gallbladder remains after surgery. 8 Either may be intentional, to prevent injury to important structures in the presence of severe inflammation or portal hypertension, or in cases where it is difficult and dangerous to perform a complete cholecystectomy. 4 , 9 Other times, an RGB may have been left behind unintentionally because of inaccurate identification of the anatomical structures, usually in the presence of inflammation and fibrosis. 10 RGB may be complicated by stones. In this study, the incidence of calculi was 1.232% (33/2678).
Patient's BMI, age, and sex
Because of the thicker subcutaneous fat layer in obese patients, only a portion of the gallbladder that is drawn out of the peritoneal cavity is removed, which can then easily lead to the formation of RGB calculi. This study demonstrated that the BMI was significantly different between the observation group and the matched group (P < 0.001); however, BMI was not an independent risk factor. Age and sex were not associated with RGB calculi.
Surgical method and time to detection
Previous studies show that long-term abdominal symptoms are present in up to 40% of patients after LC,11–14 most cases of which are owing to subtotal cholecystectomy in difficult situations, such as acute cholecystitis or Mirizzi syndrome. 8 There have been suggestions that subtypes of Mirizzi syndrome, stones, or cholecystobiliary fistula will eventually block the bile ducts and increase the difficulty of the operation. 7 Therefore, the likelihood of retained stones in a gallbladder remnant or a cystic duct stump are increased. 15 It has been reported 6 , 9 ,16–18 that the incidence of RGB calculi in LC is higher than that in OC; however, this is controversial. 19 In this study, there was no significant difference between the observation group and the matched group. It may be that to avoid trauma, the small incision used in OC results in incomplete exposure of the gallbladder and a residual cystic duct that is too long. With improved health awareness, most patients can seek medical consultation when they have PCS. In a review by Chowbey et al., 7 the authors summarized data of mean time to detection, with a range 8.3 months to 9.5 years. In this study, the time to detection in the group with RGB stones and the matched group was 3.4 ± 1.7 years and 1.8 ± 1.5 years, respectively. In the observation group, a total of 10 in 33 patients (30.30%) underwent CT or MR examination after more than 5 years; in the matched group, only 4 in 40 patients (10.00%) did so.
Length of RGB, angle of RGB and CHD
There are several reasons for the formation of RGB. The main reason is that the remnant cystic duct is too long. In an ideal scenario, the cystic duct stump should be less than 0.5 cm in length after cholecystectomy, 20 with a more than 1-cm length causing PCS. 21 To prevent massive hemorrhage or damage to the bile duct, subtotal cholecystectomy is necessary during surgery, resulting in residual gallbladder. The larger the RGB, the greater the possibility of calculi formation within the RGB. 19 When cystic ducts that run parallel to the CHD have low insertion, 6 they are all embedded in the same fibrous tissue sheath; 22 if the operator lacks sufficient experience, the cystic duct will remain too long. 18 This study showed that length of RGB and angle of RGB and CHD are statistically significant (P < 0.001, P = 0.004, respectively); the ROC curve showed cut-off values of 2.25 cm and 22.5°. Kohga et al. 23 detected the remnant gallbladder using MRCP in 20 of 35 patients who underwent cholecystectomy; the mean size was 22.6 mm, which is consistent with our research.
Choledocholithiasis and remnant cholecystitis
The literature 7 shows that if the balance of the bile duct is injured after cholecystectomy, the regulating effect of the gallbladder on the pressure of the bile duct is eliminated, the internal pressure of the CBD is increased, and the residual gallbladder duct is expanded and enlarged over a long period, forming a “small gallbladder”. The CBD responds with compensatory dilatation, which can cause choledocholithiasis and inflammation. At the same time, choledocholithiasis can bring about dilation and high pressure in the bile ducts, an enlarged remnant gallbladder, cholestasis, and stone formation. In this study, we found no correlation of RGB calculi with choledocholithiasis and remnant cholecystitis. The reason may be that patients with PCS sought timely treatment, at which time no stones have formed; this finding may also be related to the small sample size.
This study had several limitations. First, this was a single-center study, and the number of patients was relatively small. Second, whether the gallbladder status before surgery may cause recurrence of RGB calculi was not considered; this will be investigated in future studies. Third, further studies are needed regarding the association of the size and density of RGB calculi with respect to the nine variables investigated here.
Conclusion
We comprehensively analyzed patients’ clinical data and imaging to identify potential factors related to the formation of RGB calculi after cholecystectomy. Among nine variables, time to detection, length of RGB, and angle of RGB and CHD may be independent risk factors for RGB calculi.