
Abstract
Objectives
This study presented the feasibility of oxycodone as the sole opioid for general anaesthesia in minor/moderate surgery.
Methods
In this prospective, observational, descriptive study, 62 patients were enrolled and received intravenous oxycodone as the sole opioid for the induction and maintenance of general anaesthesia. We observed all of these patients to determine whether oxycodone alone could provide sufficient intraoperative and postoperative analgesia, as well as to record the extubation times and adverse events.
Results
A total oxycodone dose of 0.316 ± 0.05 mg/kg was used for induction and maintenance of general anaesthesia. The dose could maintain haemodynamic stability during surgery and good postoperative analgesia. Oxycodone caused deep sedation (nine patients had Ramsey sedation scores ≥4), leading to respiratory depression and long stays in the post-anaesthesia care unit (PACU). The extubation time (16.9 ± 6.4 minutes) increased with increasing oxycodone doses.
Conclusion
Oxycodone can be used as the sole opioid for general anaesthesia in minor/moderate surgery. However, care should be taken because of its deep sedation effect.
Introduction
Opioids are used to reduce perioperative pain, which is beneficial to recovery. In clinical practice, different opioid analgesics are commonly used for induction (fentanyl and sufentanil1–3), maintenance of general anaesthesia, and postoperative analgesia (morphine, hydromorphone, and oxycodone).4–6
Oxycodone is a strong mu opioid and kappa opioid receptor agonist that is normally used to relieve moderate to severe pain.7–9 Recently, it was reported that intravenous (IV) oxycodone could be used for induction of anaesthesia to prevent the haemodynamic response to laryngoscopy and tracheal intubation.10–12
Because oxycodone has a short onset time (peak time of approximately 5 minutes) and the same duration of action as morphine (approximately 4 hours), 6 it might provide sufficient analgesia for 4 hours when administered during induction. Therefore, we speculated that a sufficient dose of oxycodone at induction could provide sufficient analgesia in minor/moderate surgery (operation time of approximately 4 hours). In China, compound opioids are used for general anaesthesia, as follows: fentanyl and sufentanil for induction, remifentanil continuous infusion during surgery, and other analgesics (tramadol, dezocine, hydromorphone, or oxycodone) for postoperative analgesia at the end of surgery. Compared with these compounded opioids, sufficient use of oxycodone alone for induction and maintenance of general anaesthesia might be easier for the anaesthesiologist to administer. High doses of long-acting opioids can prolong extubation time and increase adverse events (such as respiratory depression, vomiting, and dizziness). However, it is unknown if oxycodone alone can be used for general anaesthesia. Only one report found that oxycodone was safe to be used for induction and maintenance during general anaesthesia without clinically significant effects on haemodynamic and respiratory parameters. 13 However, owing to the low dose of oxycodone that was used, it could not provide sufficient analgesia. There is insufficient information about the use of oxycodone alone for general anaesthesia and whether it could provide ideal intraoperative and postoperative analgesia or cause adverse events. Therefore, additional research is required to answer the following questions: can oxycodone be used as the sole opioid for general anaesthesia; and what are the extubation times and adverse events?
To answer these questions, we designed a study to determine the effective dose of oxycodone for induction and to observe the use of oxycodone alone for general anaesthesia in different minor/moderate surgeries (operation times of approximately 4 hours). In our previous prospective study, we determined the median effective dose (ED50) of IV oxycodone (0.254 mg/kg for women and 0.324 mg/kg for men) for anaesthetic induction. 12 In this study, we determined the feasibility of using oxycodone as the sole opioid for general anaesthesia in different minor/moderate surgeries.
Materials and methods
This study was approved by the ethics committee at the First Affiliated Hospital, College of Medicine, Zhejiang University (2016-383, Hangzhou, Zhejiang, China) on 6 September 2016, and was registered with the Chinese Clinical Trial Registry (www.chictr.org.cn, ChiCTR-opc-16009175) on 8 September 2016. Written informed consent was obtained from all of the patients.
Patients
All patients who were undergoing minor/moderate surgery (duration of less than or approximately 4 hours) that required general anaesthesia and tracheal intubation were enrolled into this observational, descriptive study. We included patients aged 18 to 64 years old whose status was classified as class I or II in accordance with the American Society of Anesthesiologists (ASA). Patients were excluded if they: (1) had a body mass index >30 kg/m2 or ≤18.4 kg/m2; (2) had a severe cardiovascular or respiratory disease; (3) had an expected difficult intubation; (4) had renal, liver, or haematological disorders; (5) had a high risk of aspiration or regurgitation; (6) were taking narcotics for chronic pain; or (7) had contraindications to oxycodone and flurbiprofen.
Treatments
All of the patients were transferred to the operating room without pre-medication. Standard monitors were used for pulse oximetry (SpO2), electrocardiography (ECG), and blood pressure (BP), and bispectral index (BIS) measurements. The baseline BP and heart rate (HR) were recorded.
As described in our previous report, 12 an IV bolus of oxycodone (Hamol Limited, Nottingham, U.K., 0.2–0.37 mg/kg) was administered 5 minutes before propofol (AstraZeneca, Milan, Italy, 2 mg/kg) and rocuronium (N.V. Organon, Oss, the Netherlands, 0.8 mg/kg) for induction, and tracheal intubation was performed approximately 2 minutes after induction. The oxycodone dose for induction was altered to determine the ED50 of oxycodone using Dixon’s up-and-down method. 12
Before surgery, 50 mg of flurbiprofen (Beijing Tide Pharmaceutical Co., Ltd., Beijing, China) and 0.25 mg of palonosetron (Qilu Pharmaceutical Co., Ltd., Jinan, China) were administered. General anaesthesia was maintained through continuous infusion of propofol to maintain the BIS within 40 to 60. Cisatracurium was injected as needed. Additional propofol was administered if the anaesthesiologist questioned the adequacy of the anaesthesia, and oxycodone (0.03 mg/kg) was added when the anaesthesiologist determined that there was insufficient analgesia.
A dose of 0.5 mg of atropine was administered IV when severe bradycardia occurred (HR <50 beats/minute), 6 mg of ephedrine was administered for hypotensive events (change in systolic blood pressure [SBP] <30% of baseline value or SBP <90 mmHg), and 10 mg of urapidil was administered IV for hypertensive events (change in SBP ≥30% of baseline value).
At the end of surgery, propofol infusion was stopped. The anaesthesiologist patted the patient’s shoulder gently and called the patient’s name continuously. After waking up, the patient was extubated and then transferred to the post-anaesthesia care unit (PACU) and later to the ward. Patients were transferred to the ward with stable haemodynamic parameters and respiration, NRS ≤3, and no malaise. An additional 50 mg of tramadol (Grunenthal Co., Ltd., Aachen, Germany) was administered gradually if patients reported pain and required medication until NRS ≤3, no other drugs for pain were given.
Assessment
Haemodynamic parameters (BP and HR) were recorded at the following time points: T0, arrival in the operating room; T1, before intubation; T2, 3 minutes after intubation; T3, beginning of the operation; T4, end of the operation; and T5, extubation time. The extubation time (the time from the cessation of propofol infusion to extubation), the anaesthesia time (the time from injection of oxycodone to extubation), and the PACU time (total time in PACU) were also recorded.
Blinded observers assessed the adverse events, sedation, and pain scores. The Ramsey sedation score (RSS) was used to assess the sedation state at admission to the PACU as follows: 1, the patient is anxious, agitated, or restless; 2, the patient is cooperative, oriented, and tranquil; 3, the patient responds to commands; 4, the patient gives a brisk response to a light glabellar tap or loud auditory stimulus; 5, the patient gives a sluggish response to a light glabellar tap or loud auditory stimulus; and 6, the patient does not respond to stimuli. Pain at rest was assessed based on a numerical rating scale (NRS) in the PACU and at 4, 8, and 24 hours after surgery, with 0 denoting no pain and 10 denoting the worst possible pain. Adverse events were recorded in the PACU and at 24 hours after the operation. Respiratory depression was defined as mask inhalation of oxygen and a respiratory rate of less than 8 breaths/minute. Patient satisfaction was ranked by the patient as follows: 1, satisfactory; 2, neutral; and 3, unsatisfactory.
Statistical analysis
The sample size was based on our previous study. 12 In that study, we determined the ED50 of oxycodone for induction using Dixon’s up-and-down method (seven crossover points). Here, we observed each of these patients.
Statistical analyses were performed using SPSS software, version 22.0 (IBM Corp., Armonk, NY, USA). The distribution of continuous variables was analysed for normality using the Shapiro–Wilk test. The data are presented as the number or the mean ± standard deviation (SD) for variables with normal distributions or as the median (range) for variables with non-normal distributions. Normally distributed data were compared using a t-test. Non-normal distributions were compared using the Mann–Whitney U test. Linear regression was used to analyse the relationship of extubation time with oxycodone dose and operative time. P values <0.05 were considered to be significant.
Results
Sixty-five patients were enrolled, but three patients were excluded. Two patients were excluded because oxycodone infusion caused hypertension, and one patient was excluded because of bleeding during the operation. Therefore, 62 patients were included in the final analyses. The average age of the patients was 43.9 ± 11.8 years, and 34 were men and 28 were women. The patients’ demographic data and surgical profiles are shown in Table 1.
Baseline demographic data and surgical profiles.

The data are presented as the mean ± SD or as the median (range).
Anaesthesia time means the time from injection of oxycodone to extubation.
Extubation time means the time from the cessation of propofol infusion to extubation.
PACU time means time in the post-anaesthesia care unit
BMI, body mass index; PACU, post-anaesthesia care unit; SD, standard deviation.
The patients underwent several types of operations in this study, including orthopaedic surgery (femoral resection and internal fixation), gynaecological surgery (conization of the cervix, laparoscopic ovarian cystectomy, laparoscopic hysterectomy), general surgery (quadrant mastectomy, radical mastectomy, great saphenous vein high ligation and exfoliation, laparoscopic cholecystectomy, laparoscopic indirect hernia repair, thyroidectomy), urological surgery (laparoscopic renal cyst unroofing, laparoscopic ureteropelvic orthotics), and ear, nose, and throat (ENT) and maxillofacial surgery (laser for laryngeal cancer, modified radical mastoidectomy, tonsillectomy, parotidectomy, partial mandible resection, internal fixation for condylar fracture) (Table 1).
During surgery, haemodynamic parameters (BP and HR) changed at different time points (Figure 1) but most remained within the clinically stable range (the changes were less than 20% of the baseline). The extubation time increased with increasing doses of oxycodone (R = 0.35, P = 0.005) but did not significantly decrease with longer operative times (R = −0.14) (Figure 2).

Blood pressure and heart rate at different time points. Panel A: blood pressure; Panel B: heart rate. The data are presented as the mean ± SD. * indicates P < 0.05; ** indicates P < 0.01.

Relationships among oxycodone dose, operation time, and extubation time. Linear regression of the effect of oxycodone dose (a) and operation time (b) on extubation time. The lines represent the correlations.
Oxycodone provided good sedation and pain management in the PACU (Figure 3). Nine patients were in the deep sedation group (RSS ≥4) (Figure 3a). The PACU time in the deep sedation group (RSS ≥4) was 51.1 (25–120) minutes, which was longer than that in the less sedation group (RSS <4) (35.6 [15–80] minutes, Z = 2.02, P = 0.043). There were no differences in total oxycodone dose (0.32 [0.19–0.42] mg/kg vs. 0.33 [0.25–0.37] mg/kg, Z = 0.06); operation time (53 [29–114] minutes vs. 77 [24–249] minutes, Z = 1.479), and anaesthesia time (88 [47–142] minutes vs. 114 [48–297] minutes, Z = 1.449) between the deep sedation group (RSS ≥4) and the less sedation group (RSS <4). The NRS was 0 (0–6) in the PACU (Figure 3b). Four patients felt pain and required additional tramadol in the PACU. NRS was 0 (0–5), 1 (0–5), and 1 (0–5) at 4, 8, and 24 hours after the operation, respectively (Figure 3b). Only one patient required tramadol on the ward.
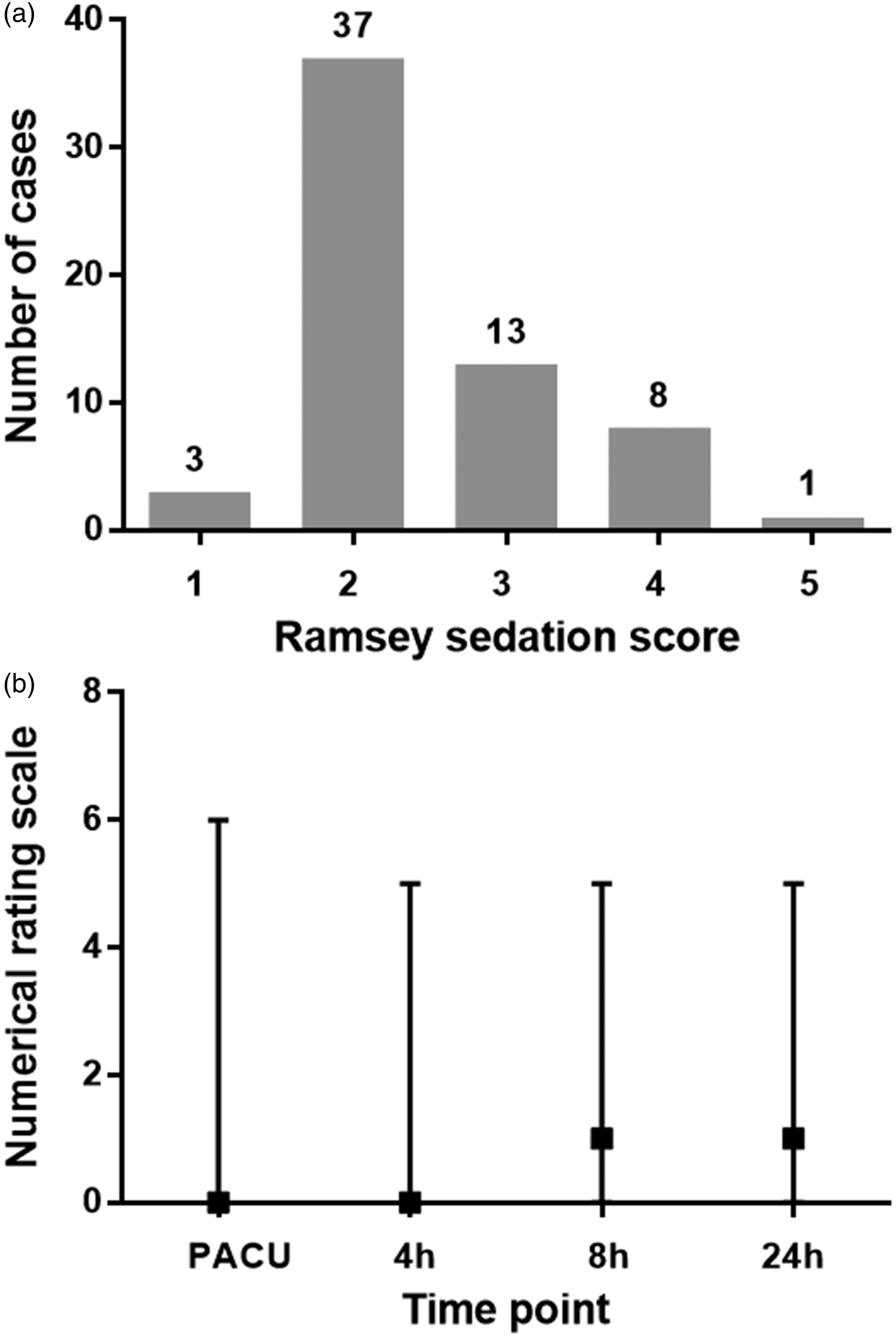
Ramsey sedation score (RSS) and numerical rating scale (NRS) scores for pain in the post-anaesthesia care unit (PACU) and at 4 to 24 hours after the operation. Panel A: RSS in the PACU; Panel B: NRS scores in the PACU and at 4 to 24 hours after the operation. The data are presented as the number of cases with each score (a) or the median (range) at each time point (b). Grey squares represent the median, and the straight lines represent the range (b).
Adverse events that are associated with oxycodone (seen in the dispensatory), such as respiratory depression, vomiting, and dizziness, were recorded in the PACU and within 24 hours after surgery (Table 2). Three patients had respiratory depression in the PACU due to deep sedation. Fifty-nine patients (95%) had a satisfactory experience, two patients (3%) had a neutral experience, and one patient (2%) had an unsatisfactory experience due to severe vomiting.
Incidence of adverse events in the PACU and within 24 hours after surgery.

The data are presented as the numbers (percentages).
PACU, post-anaesthesia care unit.
Discussion
Oxycodone could be used as the sole opioid for general anaesthesia and could maintain haemodynamic stability and provide good intra- and postoperative pain management in minor/moderate surgery.
Compound opioids (fentanyl and sufentanil for induction, remifentanil for maintenance, and other analgesics for postoperative analgesia) are widely used in current clinical practice for general anaesthesia. Calculation, conversion, and determination of the administration time between multiple opioids requires an experienced anaesthesiologist. Oxycodone is an opioid with a short onset time and long duration of action that can be used for anaesthesia induction or maintenance or postoperative pain management maintenance.10–14 We speculated that a sufficient dose of oxycodone given at induction might provide sufficient analgesia for the operation and would be easier for the anaesthesiologist to administer. There is insufficient information about the use of oxycodone alone for general surgery. It is unknown whether oxycodone could be used as the sole opioid for general anaesthesia or if it causes more adverse events due to its long duration of action, especially in shorter operations. Therefore, we performed this observational, descriptive study of minor (such as conization of the cervix, laser treatment of laryngeal cancer, quadrant mastectomy) and moderate (such as laparoscopic hysterectomy, laparoscopic pyeloureteroplasty, thyroidectomy) surgeries with operation times ranging from 24 to 249 minutes to observe the feasibility of oxycodone as the sole opioid for general anaesthesia.
HR was more sensitive than SBP/DBP to simulation. Because we defined no intubation reaction as SBP/DBP and HR increases of <20% from baseline values, we used more oxycodone doses for induction than other reports, 10 , 11 which defined no intubation reaction only for SBP/DBP changes, as explained in a previous report. 12 Because the study was designed to determine the ED50 of IV oxycodone for anaesthetic induction using Dixon’s up-and-down method, some inefficient oxycodone doses were used and caused the BP and HR to increase at T2 (3 minutes after intubation) and T3 (beginning of the operation) (Figure 1). After providing deeper anaesthesia by infusing more propofol under BIS monitoring, oxycodone (0.03 mg/kg) was added when the anaesthesiologist detected insufficient analgesia. Finally, we used large total doses of oxycodone (approximately 0.316 ± 0.05 mg/kg) and observed its feasibility and adverse events.
We found that oxycodone alone combined with propofol for general anaesthesia could maintain the haemodynamic stability during the operation (BP and HR changes were less than 20% of the baseline), which is a basic requirement of general anaesthesia. Oxycodone can efficiently prevent postoperative urinary catheter-related discomfort, 14 and this seemed to be the same with tracheal tubes because there was no increase in HR and blood pressure during extubation in our study (Figure 1). This outcome was similar to other reports, 13 which used smaller oxycodone doses (0.075 mg/kg during induction and 0.05 mg/kg during maintenance), causing slight HR changes (previous intubation to recovery, 72.5 beats/minute vs. 78.3 beats/minute) and no obvious BP changes. We used larger doses of oxycodone to better maintain haemodynamic stability during extubation.
By exploring the extubation time with oxycodone doses and operation times, we found that extubation time increased with increasing doses of oxycodone (R = 0.35, P = 0.005), but it did not obviously decrease with operation times (R = −0.14) (Figure 2). Based on the estimation of the correlation equation, the extubation time was approximately 16 minutes with a dose of 0.3 mg/kg oxycodone or for a 2-hour operation. As shown in Figure 3b, the extubation times fluctuated sharply in short operations (less than 60 minutes), and they were all less than 20 minutes in longer operations (longer than 120 minutes). It seems that oxycodone that was used as the sole opioid for general anaesthesia is suitable for moderate surgery (operation time from 2 to 4 hours). Because the data on operation time was not normally distributed and there were fewer data for long operations (longer than 2 hours), the extubation time for long operations requires more research.
The total dose of oxycodone that was used in this study was approximately 0.316 ± 0.05 mg/kg (Table 1), which could be equivalent to the induction dose of fentanyl (3–5 µg/kg) because the potency ratio of fentanyl to oxycodone is approximately 1:75 to 1:100. 15 Therefore, a sufficient dose of oxycodone for induction might provide sufficient analgesia in minor/moderate surgery and might be easier for the anaesthesiologist to provide.
In this study, oxycodone that was used as the sole opioid for general anaesthesia provided good postoperative analgesia. In the PACU, only four patients required additional tramadol to reduce pain. In one case, the operation time was 249 minutes (approximately 4 hours), but the anaesthesia time was 297 minutes, which exceeded the action time of oxycodone, and an additional analgesic was required. Although the analgesic intensity decreased with time during the 24 hours after surgery (median NRS increased from 0 to 1) (Figure 3b), most of the patients had good pain management. Only one patient required additional medication for pain control within 24 hours after surgery on the ward.
The use of large doses of oxycodone as the sole opioid for general anaesthesia might cause excessive sedation. Nine patients had deep sedation (RSS ≥4) in the PACU (Figure 3a), which led to longer PACU times (51.1 [25–120] minutes) and three cases of respiratory depression in the PACU (Table 2). Oxycodone might cause sedation, which we found at induction time, 12 and more adverse events than fentanyl. 16 Although the operation time and anaesthesia time in the deep sedation group (RSS ≥4) were not different from those in the less sedation group (RSS <4) (53 [29–114] minutes vs. 77 [24–249] minutes and 88 [47–142] minutes vs. 114 [48–297] minutes, respectively), the operation time in the deep sedation group tended to be less than 2 hours. Because of the limitations of this study (fewer cases of long operations), more research is required to determine whether oxycodone can cause less deep sedation in long operations (longer than 2 hours).
The three respiratory depression patients recovered after 5 to 10 minutes with PACU nurses continuously calling their names to keep them breathing with oxygen masks; no mask positive pressure ventilation or intubation was required. One patient had a long PACU stay (80 minutes) due to dizziness. All of these patients were transferred to the ward safely.
Nausea and vomiting are common adverse events with oxycodone. 15 , 16 To prevent nausea and vomiting, we administered 0.25 mg of palonosetron to the patients before surgery. No patient experienced nausea and vomiting in the PACU, but 17.7% of the patients experienced nausea, and 14.5% of the patients experienced vomiting during the 24 hours after surgery (Table 2). One patient reported an unsatisfactory experience due to severe vomiting. Nausea and vomiting can be associated with many risk factors, such as age, gender, a previous history of motion sickness or postoperative vomiting, and the type and duration of the surgical procedure. 17 Thus, the occurrence of nausea and vomiting in this study could be due to a variety of reasons and not only to oxycodone. This point requires further study including limiting other factors to determine whether oxycodone causes more serious nausea and vomiting than other opioids.
Rare adverse reactions were observed in two male patients who experienced very severe hypertension after oxycodone injection, which was discussed in the previous report. 12 This event might not be due to an oxycodone reaction, and it was not reported in other studies. These two patients were excluded from this study.
This study has several limitations. (1) The study explored whether oxycodone could be used as the sole opioid in general anaesthesia for minor/moderate surgery. We could not compare oxycodone with other opioids that are normally used for general anaesthesia. (2) This study involved minor/moderate surgeries that were less than or approximately 4 hours in length and that required tracheal intubation, but the types and times of the operations were not limited. The operation time was not normally distributed and was less for long cases (operation time from 2 to 4 hours). Different types of operations can cause different levels of acute pain and can require different doses of opioids. Thus, the oxycodone dose used in this study might not be sufficient for all types of operations, especially major operations. (3) Although we determined the extubation time when a high dose of oxycodone was used for general anaesthesia, administration of additional oxycodone during general anaesthesia could affect the extubation time. (4) We obtained these results by observing all of the patients from our previous study, 12 and a larger sample size might have provided clearer and stronger evidence. (5) We did not compare the extubation time that was associated with oxycodone to that associated with other opioids. Therefore, further cohort studies are required to evaluate the feasibility of oxycodone that is used as the sole opioid for general anaesthesia.
Oxycodone can be used as the sole opioid for general anaesthesia in minor/moderate surgery for pain management. However, care should be taken because of its deep sedation, which might cause respiratory depression and a long stay in the PACU.
Footnotes
Acknowledgements
All authors thank Duo Lyu, MD (Statistician, Institute of Clinical Trials, the First Affiliated Hospital, College of Medicine, Zhejiang University).
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received grants from the Medical Scientific Research Foundation of Zhejiang Province, China (2016KY104 and 2020KY626).