
Abstract
Objective
To evaluate the clinical performance of cantilevered resin-bonded fixed partial dentures (CRBFPDs) in single tooth replacement in elderly patients at Qingdao Stomatological Hospital.
Methods
In total, 186 CRBFPDs in 153 patients were made from cobalt-chrome alloy. Panavia F 2.0 was used as a luting agent after air-abrasion. Restoration were evaluated at 3-month intervals with regard to function, esthetics, and possible complications.
Results
CRBFPDs were evaluated after intervals of 12 to 40 months. The average clinical service time (i.e., length of time in situ at examination, including re-cementation after debonding) was 26.2 ± 13.6 months. Among these CRBFPDs, 87 (46.8%) were bridges in the maxilla, while 99 (53.2%) were bridges in the mandible. Most CRBFPDs (184, 98.9%) survived throughout the study period, while two (1.1%) were regarded as failed. The majority of debonded bridges had been used to replace the maxillary central incisor (60%).
Conclusion
Our findings confirm the successful clinical performance of CRBFPDs with tooth preparation designs involving mesial and distal vertical grooves in elderly patients.
Introduction
Resin-bonded bridges were first introduced in the 1970s, but initial implementation attempts failed. 1 Because of the continuous development of adhesives and retention designs, the clinical survival rate of resin-bonded fixed partial dentures has reached nearly 88% and continues to increase. 2 Resin-bonded fixed partial dentures have been accepted as an alternative fixed restorative treatment option for the replacement of a missing single tooth, in contrast to traditional fixed partial dentures that involve extensive preparation of abutment teeth. For cantilevered resin-bonded fixed partial dentures (CRBFPDs), the pontic generally moves with the single abutment tooth, particularly during protrusive and lateral movements under tooth contact. 3 Because of advancements concerning materials and resin cements with improved bonding capacity, CRBFPDs might constitute an alternative treatment for replacement of a missing single tooth.4–7
Djemal et al. 8 reported that the risk of failure for a fixed-fixed partial denture was nearly twofold greater than the risk for a cantilevered fixed partial denture. Furthermore, with each additional abutment, the likelihood of debonding was found to increase. Botelho et al. 9 reported that two-unit CRBFPDs have significantly better success and survival than fixed-fixed three-unit resin-bonded bridges design for the replacement of a maxillary incisor. To the best of our knowledge, no study has described the clinical performance of CRBFPDs for restoration of single tooth loss in elderly patients. Therefore, the present study evaluated the clinical effectiveness of CRBFPDs in single tooth replacement in elderly patients.
Methods
Patient and abutment selection
This study included elderly individuals with single-unit edentulous spans bounded by sound teeth, all of whom were patients at Qingdao Stomatological Hospital during the period from September 2015 to January 2019. The study was conducted in accordance with the tenets of the Declaration of Helsinki; the study protocol was approved by the Ethics Committee of our hospital (No. 2020-2022). Written informed consent was obtained from each participant.
The selected abutment teeth were healthy, unrestored or minimally restored, free of caries and periodontal disease, and had adequate enamel height and width (clinical crown >4 mm). All patients underwent simple restorative clinical treatment. In addition, replacements of missing molars were limited to a premolar-sized pontic.
Clinical and laboratory procedures
Tooth preparation comprised maximization of the surface area for bonding and enhance of resistance. When possible, retention was improved by preparation of 1-mm deep mesial and distal vertical grooves. All tooth preparations were conservative at the lingual aspect with a supragingival finish line; the incisal margin of preparation was 1 mm shorter than the incisal edge in the anterior region (Figure 1a, b).
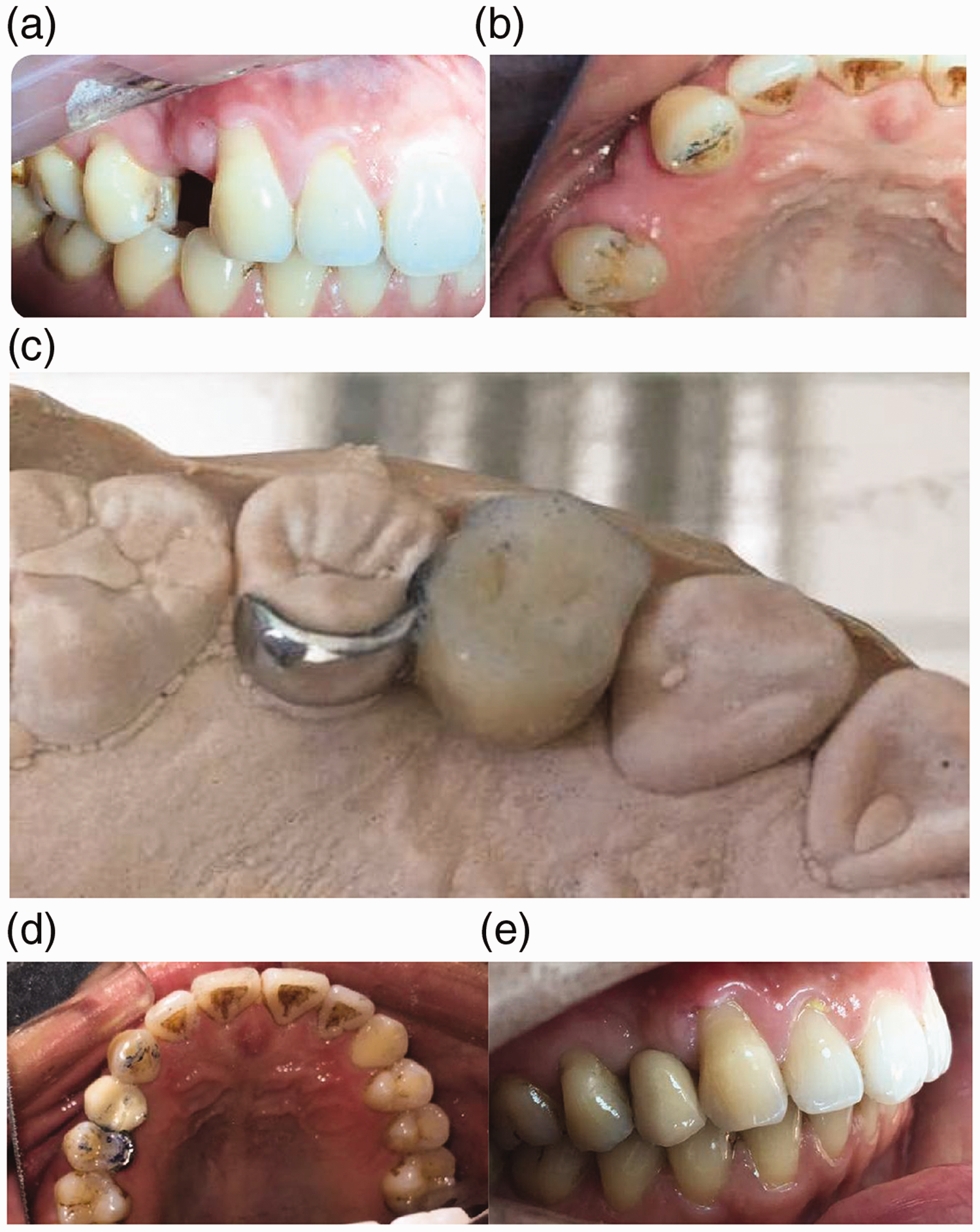
Clinical photographs of teeth involved in this study.
After preparation, a full-arch working impression was made with polyvinylsiloxane impression material in a custom tray. The outline of the bridge framework was drawn on a working cast by a single technician. A cobalt-chrome alloy (Bondiloy, Austenal, Inc., Chicago, IL, USA) suitable for porcelain bonding was used. The minimum dimensions of the connector were 2 mm labiolingually and 4 mm cervicoincisally. The minimum thickness of the metal retainer wings was 1.0 mm. During the fitting process, pontic occlusion was adjusted to prevent occlusion contact or allow slight contact in the centric occlusion, and to provide protection from occlusion during lateral and protrusive excursions. After a satisfactory try-in, bridges were returned to the laboratory for glazing and polishing; the retainer surfaces were subjected to grit blasting with 50 μm of aluminum oxide powder at a pressure of 520 kPa. CRBFPDs were cemented with Panavia F 2.0 (Kuraray Medical, Okayama, Japan) in accordance with the manufacturer’s instructions (prepared enamel was etched with 37% phosphoric acid for 15 s prior to bonding) under rubber dam isolation (Figure 1c–e).
Recall and evaluation
Recalls and evaluations were conducted at 3-month intervals. Patients who did not attend clinical assessments were contacted by telephone to acquire information regarding the performance of their bridges. “Survival” of a CRBFPD was defined as any restoration that remained in situ. Complications were recorded when bridges were debonded on ≥2 occasions. To determine the degree of patient satisfaction with the bridges, the scale was subdivided into units from 0 to 100, where 0 represented “very dissatisfied” and 100 represented “very satisfied.” 10
Statistical analysis
Comparisons were performed using analysis of variance, the chi-squared test, and the t-test, as appropriate. P<0.05 was considered statistically significant.
Results
In total, 153 patients (186 bridges) were included in the present study. Sixty-eight patients (44.4%) were men and 85 patients (55.6%) were women; their median age at the time of bridge insertion was 67.7 years. CRBFPDs were evaluated after 12 months of use. The average clinical service time (i.e., length of time in situ at examination, including re-cementation after debonding) was 26.2 ± 13.6 months (Table 1). Furthermore, 87 bridges (46.8%) were in the maxilla, while 99 bridges (53.2%) were in the mandible.
Distribution of replaced teeth.

Most CRBFPDs (88%) survived throughout the study period. Most instances of debonding involved bridges that had replaced the maxillary central incisor (60%). Three CRBFPDs that replaced maxillary central incisors require re-cementation after debonding; one bridge exhibited debonding on more than one occasion (25%). However, after re-cementation, these were functioning appropriately at the end of the study census date. One prosthesis that replaced posterior teeth exhibited debonding after 25 months. Excessive occlusal contacts and pontic overload were the presumed causes of debonding of the prosthesis that replaced posterior teeth; after debonding, the patient selected a removable partial denture instead of re-cementation due to the loss of additional teeth. In total, two prostheses (1.1%) were regarded as failed. None of the abutments had a depth of ≥3 mm. The bridges that replaced mandibular teeth and maxillary premolars exhibited optimal performance without debonding. There was no statistically significant association between pontic position and debonding.
No secondary caries or obvious change in abutment mobility occurred. The degree of satisfaction with CRBFPDs was high (92.6 ± 6.1); this was not influenced by the occurrence of failure. Overall, only one score was <70; the lowest score was given for a bridge that had debonded more than twice.
Discussion
In a prior in vitro study, debonding was found to result from cohesive failure within cement at the filler–resin interface. 11 Another in vitro study revealed that the use of Unifix and airborne-particle abrasion (50-µm aluminum oxide) provided the strongest physical bond. 12 In the present study, cobalt–chrome alloy was chosen as the framework material because the application of nickel–chromium alloy is decreasing in China. 13 Bond strength could be significantly improved through the airborne-particle abrasion of the alloy. Furthermore, the cement and alloy material were limited to reduce the number of clinical variables in the present study.
Locations of pontics and/or abutments
It has been suggested that a larger enamel surface area for cement is associated with greater bridge retention. 14 In our study, the bridges that replaced mandibular teeth and maxillary premolars exhibited optimal performance, without debonding. In contrast, bridge debonding occurred at sites involving maxillary incisors, maxillary canines, and maxillary molars. When compared with bridges that replaced other teeth, bridges that replaced maxillary central incisors exhibited greater likelihood of debonding. In the present study, all central incisor pontics were cantilevered from the neighboring maxillary central incisor. When a tooth with an equivalent palatal surface area is used, the bridge is cantilevered across the midline. The clinical effectiveness of this approached remains unknown and requires further investigation.
Periodontal outcomes
None of the abutments had a probing depth of ≥3 mm. The periodontal receptors of abutment teeth were presumed to prevent pontic overloading during mastication, thereby minimizing the risks of movement or tilting of the abutment tooth. Botelho 14 also warned against the use of abutment teeth with bone loss in patients with uncontrolled periodontitis because of possible drifting. It was found that there was no difference in periodontal response (e.g., swelling or pain) between CRBFPDs and a fixed-fixed resin bonded bridge. 11
Tooth preparation
Tooth preparation can increase the thickness of metal retainers and reduce the shear–peel force on the cement junction. Priest 15 recommended enhancing the resistance of abutment teeth through the use of grooves. Abuzar et al. 16 reported that the survival rates of anterior resin-bonded bridges with tooth preparation involving mesial and distal vertical grooves were 98% at 5 years, 97.2% at 10 years, and 95.1% at >12 years. The placement of supragingival retainer margins might facilitate good oral hygiene to control dental plaque and prevent gingivitis, periodontitis, and dental caries. Furthermore, this placement may simplify the impression and finishing procedures.
There were some limitations in this study. Because of the limited data, no Kaplan–Meier survival curve could be generated in this study; this analysis requires a larger sample size in a future study. Moreover, additional prospective studies are needed to observe the long-term performance of CRBFPDs in elderly patients, and to compare this performance against other bridge designs.
Conclusion
In this study, CRBFPDs demonstrated a high survival rate with short longevity. Thus, CRBFPDs constitute a conservative treatment suitable for both young and elderly patients.