
Abstract
Objective
Coronary tortuosity may affect epicardial coronary arterial blood flow. This study aimed to investigate the effect of coronary tortuosity on coronary flow reserve and the coronary microcirculation in patients without apparent coronary atherosclerosis.
Methods
Prospective patients (n = 8, 3 men, mean age: 58 ± 6.0 years) with coronary tortuosity and without apparent coronary atherosclerosis were enrolled. Coronary tortuosity was defined by the finding of ≥three bends (defined as a ≥45° change in vessel direction) along the main trunk of the left anterior descending artery or left circumflex artery. Coronary flow reserve and the index of microcirculatory resistance were measured by the thermodilution technique.
Results
A total of eight coronary arteries with coronary tortuosity were analyzed. The mean fractional flow reserve was 0.98 ± 0.007. The mean coronary flow reserve was 1.5 ± 0.3, which is much lower than that in the normal coronary artery as reported in the literature. The mean index of microcirculatory resistance was 26.7 ± 2.3, which is much higher than that in the normal coronary artery.
Conclusions
Coronary tortuosity is associated with decreased coronary flow reserve and an increased index of microcirculatory resistance.
Keywords
Introduction
Although coronary tortuosity is a common finding in coronary angiography, the effects of CT on cardiovascular prognosis1,2 and myocardial ischemia3,4 remain to be determined. Whether coronary tortuosity is related to microvascular dysfunction, which can cause angina symptoms and increase the incidence of adverse cardiovascular events in some patients without severe coronary stenosis, is unclear.3,5
The index of microcirculatory resistance (IMR) and coronary flow reserve (CFR) can be used to define microvascular dysfunction.6–8 Because coronary tortuosity may have some limited effect on epicardial coronary arterial blood flow,9–12 we tested the hypothesis that coronary tortuosity is closely related to the coronary microcirculation. Therefore, the present study aimed to clarify the effect of coronary tortuosity on CFR and the IMR as derived by invasive measurement.
Methods
Patient population
Prospective patients who underwent coronary angiography owing to chest pain were included. Patients with acute coronary syndrome, previous myocardial infarction or coronary revascularization, myocardial diseases, tachycardia, diabetes, hypotension, or heart failure were excluded. The study was approved by the ethics committee of Zhongda Hospital, Southeast University (2018-01; NCT No: ChiCTR2000033671). All enrolled patients signed informed consent.
Coronary angiography
Coronary angiography was performed using standard techniques. Coronary tortuosity was evaluated by special angulations. Coronary tortuosity was identified by ≥three bends (defined as a ≥45° change in vessel direction) along the main trunk of the left anterior descending artery or left circumflex artery (Figure 1).

Left circumflex coronary artery tortuosity.
Coronary physiological assessment
Coronary physiology was assessed as previously described.8,13 In brief, we calibrated 0.014-inch coronary pressure to equalize the pressure of the guiding catheter with a sensor positioned at the ostium of the coronary artery. The guiding catheter was then advanced to the distal coronary artery. CFR, the IMR, and fractional flow reserve (FFR) were measured as described below. The transit time of room temperature saline that was injected down from the coronary artery was determined by the thermodilution technique. A volume of 3 mL of room temperature saline was injected three times down the coronary arteries, and the resting mean transit time (Tmn) was measured. Hyperemia was induced on the basis of a reduction in average blood pressure by 20% through intravenous infusion of adenosine (140 μg/kg/minute), and the hyperemic Tmn was also measured. Mean aortic pressure (Pa) and mean distal coronary pressure (Pd) were measured in the maximal hyperemic states. FFR was calculated by the ratio of Pd/Pa at maximal hyperemia. CFR was calculated by resting Tmn/hyperemic Tmn. The uncorrected IMR was calculated by Pd × Tmn during hyperemia (Figure 2).
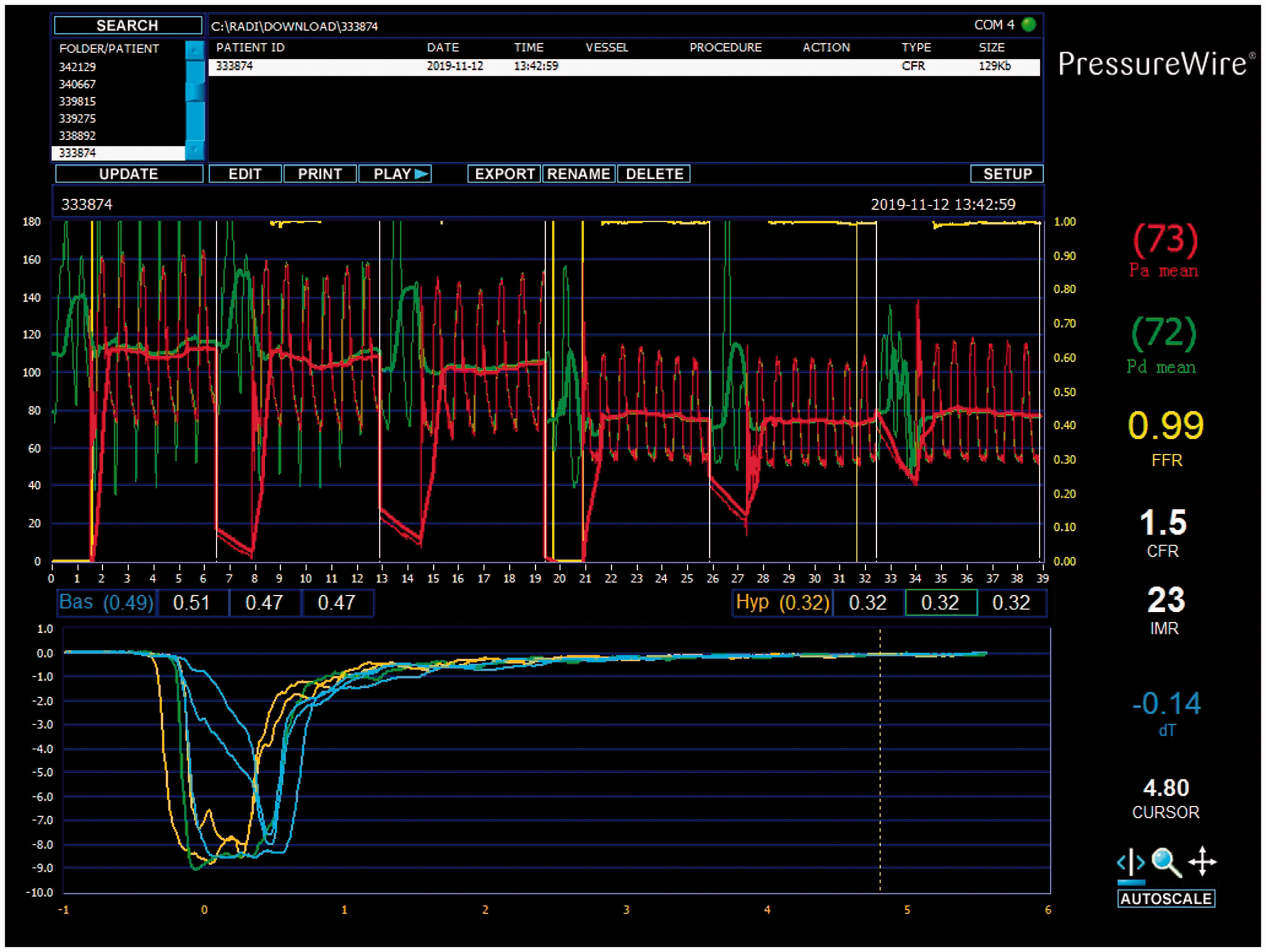
Measurement of CFR and the IMR.
Statistical analysis
SPSS version 15.0 for Windows (SPSS Inc., Chicago, IL, USA) was used to perform all statistical calculations. Continuous variables are expressed as arithmetic mean ± standard deviation.
Results
A total of eight patients (three men, mean age: 58 ± 6.0 years) with coronary tortuosity and without apparent coronary atherosclerosis were enrolled. Two patients had hypertension. A total of eight coronary arteries with tortuosity were evaluated. The mean FFR was 0.98 ± 0.007. The mean CFR was 1.5 ± 0.3, which is lower than that in the normal coronary artery (not measured in the current study, see normal data in the Discussion below). The mean IMR was 26.7 ± 2.3, which is higher than that in the normal coronary artery.
Discussion
To the best of our knowledge, this is the first study to clarify the effect of coronary tortuosity on coronary microcirculation. The relationship between coronary tortuosity and coronary artery disease is controversial.2,14–16 The effect of coronary tortuosity on coronary atherosclerosis may be due to altered distribution of endothelial shear stress.11,12,17,18 Our results highlight the association between coronary tortuosity and disturbed coronary microcirculation. Because coronary microvascular dysfunction is an important cause of myocardial ischemia, 19 our data suggest that coronary tortuosity might be a reason for coronary microvascular dysfunction in patients without apparent coronary atherosclerosis. Structural and functional abnormalities are involved in the mechanism of coronary microvascular disease.19–21 Patients with chest pain and nonobstructive coronary artery disease have a high prevalence of coronary microvascular abnormalities, but these are poorly associated with conventional cardiovascular risk factors. 22 Obstructive coronary artery disease, myocardial diseases, iatrogenic causes, and diabetes are associated with coronary microvascular disease.21,23–25 Patients with ischemia and no obstructive coronary artery disease are associated with an elevated risk of major adverse cardiovascular events.26,27 A number of invasive and noninvasive methods, including intracoronary Doppler flow velocity wires, positron emission tomography, and cardiac magnetic resonance imaging, can be used to accurately assess microvascular function. The thermodilution-derived method for assessing coronary flow can be used for measuring CFR and the IMR.6,7,20,21 Non-endothelium-dependent microvascular dysfunction is defined as CFR < 2.5 in response to adenosine. Endothelium-dependent microvascular dysfunction is defined as a change in coronary blood flow in response to acetylcholine by <50%.22,27 Guidewire-based CFR and IMR are recommended in the diagnosis of microvascular angina. 28 CFR and the IMR can provide additional diagnostic and prognostic values for patients with ischemic heart disease, and a low CFR with a high IMR are associated with a poor prognosis. 29 The IMR is the reciprocal of distal coronary pressure divided by the mean conduction time in the maximum congestive state. 8 A CFR ≤2.0 or IMR ≥25 are indicative of abnormal microcirculatory function. 28 Therefore, our data on a low CFR and a high IMR indicate the presence of coronary microcirculatory dysfunction.
Our previous simulation and experimental studies showed that coronary tortuosity resulted in a greater decrease in coronary blood pressure dependent on the severity of tortuosity, but this decrease may be limited to a certain extent.10,12 A previous study showed that the effect of coronary tortuosity on coronary blood supply at rest was minimal. 9 However, coronary arteries with coronary tortuosity might lack the ability to sufficiently adjust for distal resistance to compensate for the extra resistance generated by tortuosity during exercise. Therefore, coronary tortuosity might lead to ineffective regulation of the blood supply during stress. In line with this finding, a maximum increase of 96% in mean diastolic driving pressure was observed in a coronary tortuosity model during exercise. 11 Our previous case study showed that vessel wall pressure of a tortuous coronary artery was decreased in the bend section, and the maximum curvature was >1 mm−1 in this region. 19 Therefore, this may lead to inadequate blood supply in the downstream vessels. Our study showed that coronary tortuosity led to a reduction in CFR and an increase in the IMR, which indicated that coronary tortuosity was related to microcirculatory dysfunction. We speculate that the mechanism involved in our finding is related to endothelial dysfunction and ineffective regulation of blood supply.9,30
This study has some limitations. One limitation is that the sample size of the study was small. A larger sample size will be measured in a future study. The long-term effects of coronary tortuosity-related changes on a reduced FFR and high IMR should also be tested in a larger patient cohort.
Conclusion
Coronary tortuosity can lead to a decrease in CFR and an increase in the IMR. Therefore, coronary tortuosity is related to microcirculatory dysfunction and may be related to myocardial ischemia during exercise. Future studies are required to validate if coronary tortuosity is the mechanism involved in patients with microcirculatory dysfunction.