
Abstract
Splenic infarction is rare, resulting from occlusion of the splenic artery or its branches. Its aetiology is complex and multifactorial involving various vascular and thrombotic diseases, thus, misdiagnosis or missed diagnosis is common. Here, the case of a 45-year old male patient diagnosed with splenic infarction caused by secondary erythrocytosis associated with obstructive sleep apnoea/hypopnoea syndrome (OSAHS) is reported. The patient presented with 10 days of abdominal distension and pain that worsened after eating, and had developed to include nausea, vomiting and fever. The patient had a history of night snoring for over 10 years without treatment, a diagnosis of chronic pulmonary heart disease and secondary polycythaemia 5 years previously, and diagnosis of OSAHS 1 year previously. He had not received previous non-invasive ventilation or oxygen therapy. Enhanced upper abdomen computed tomography (CT) showed splenic infarction, bone marrow cytology suggested secondary polycythaemia, and sleep polysomnography revealed severe OSAHS. Low molecular-weight heparin, ceftriaxone, fluid and oxygen treatment gradually relieved abdominal distension and pain. Enhanced CT showed splenic infarction improvement. The present case highlights that splenic embolism should not be ignored as a potential complication of OSAHS.
Introduction
Diseases that cause increased blood viscosity may result in limited tissue perfusion, ischaemia and thrombosis.1,2 In the case of the spleen, embolization related to multiple factors, including intra-splenic thrombosis, arteriosclerosis, or embolism due to various causes, may lead to splenic infarction.1,2 Although splenic infarction is a rare condition, misdiagnoses or missed diagnoses are common. 3
Obstructive sleep apnoea/hypopnoea syndrome (OSAHS) is a sleep-related breathing disorder caused by upper airway collapse during sleep that may be involved in the development of a variety of cardiovascular, cerebrovascular and thrombosis-related diseases.4,5 Here, the case of a patient with splenic infarction caused by secondary erythrocytosis associated with OSAHS is reported
Case report
Ethics approval was not required to publish this case report, and as all patient details were deidentified, informed consent from the patient was not deemed necessary.
A 45-year old male patient was admitted to the Affiliated Hospital of Qinghai University, Xining, China, in October 2019, with abdominal distension and pain below the left costal margin and around the umbilicus for 10 days previously, without obvious cause, and which radiated to the waist and back and became worse after eating. His initial symptoms had not been improved after taking actofructose laxative. Three days following initial symptom onset, the patient had developed persistent stabbing pain in the left lumbar region and back and aggravated abdominal distension, but with no nausea or vomiting, and with normal exhaust and defecation. At this point, the patient was referred to a local county hospital and diagnosed with acute pancreatitis. Pantoprazole (40 mg, once daily, intravenously) and octreotide (100 μg, every 8 h, intravenously) were administered to suppress acid and pancreatic secretion, respectively. The patient then developed abdominal distension and pain accompanied by nausea, vomiting and fever, and was referred to the Affiliated Hospital of Qinghai University. The patient had an over 10-year history of night snoring without any treatment. Five years previously, he had been diagnosed with chronic pulmonary heart disease and secondary polycythaemia due to cyanosis and decreased activity endurance. The patient had been diagnosed with OSAHS 1 year previously, confirmed by sleep polysomnography (PSG), and had not received any prior non-invasive positive pressure mechanical ventilator and oxygen treatment.
Physical examination showed temperature, 37.4 °C; pulse rate, 120 beats per min; respiratory rate, 30 breaths per min; blood pressure, 90/60 mmHg; clear mind; poor mental status; cyanosis; jugular vein filling (suggesting right ventricular dysfunction); symmetrical thoracic cavity (suggesting no thoracic abnormality); moist rales at the bottom of both lungs; normal rhythm; P2 >A2; and tricuspid auscultation area with grade 3/6 systolic murmurs. The patient also showed abdominal distension, drum sound, mild tenderness in inferior xiphoid process and left upper abdomen, no rebound pain and muscle tension, and bowel sounds at a rate of approximately once per minute. Routine blood test showed white blood cells, 11 × 109/l; neutrophils, 77%; red blood cells, 6.15 × 1012/l; haemoglobin, 204 g/l; platelets, 153 × 109/l; D-dimer, 2.1 mg/l; normal liver and kidney function, and normal amylase and lipase levels.
Chest computed tomography (CT) showed consolidation of the lower lobe of both lungs and a small amount of exudate. Pulmonary artery CT angiography showed no obvious pulmonary artery filling defect (Figure 1). Enhanced CT of the upper abdomen showed splenic infarction (Figure 2), and single wedge or irregular low-density lesions were observed in the spleen, with the base at the outer edge of the spleen and the tip pointing to the splenic hilum. The boundary was clear or fuzzy, and the lesion was not strengthened after enhancement. Mesenteric vascular CT showed no obvious embolization. The patient received 8 000 IU low molecular-weight heparin (every 12 h, subcutaneously) for anticoagulant therapy; 4.0 g ceftriaxone (every 12 h, subcutaneously) for anti-infection; rehydration fluids; oxygen and other treatments. Following 1 week of treatment, abdominal distension and pain were gradually relieved. At day 10 following initiation of treatment that included low molecular-weight heparin, enhanced CT of the upper abdomen showed improvement of the splenic infarction (Figure 3).
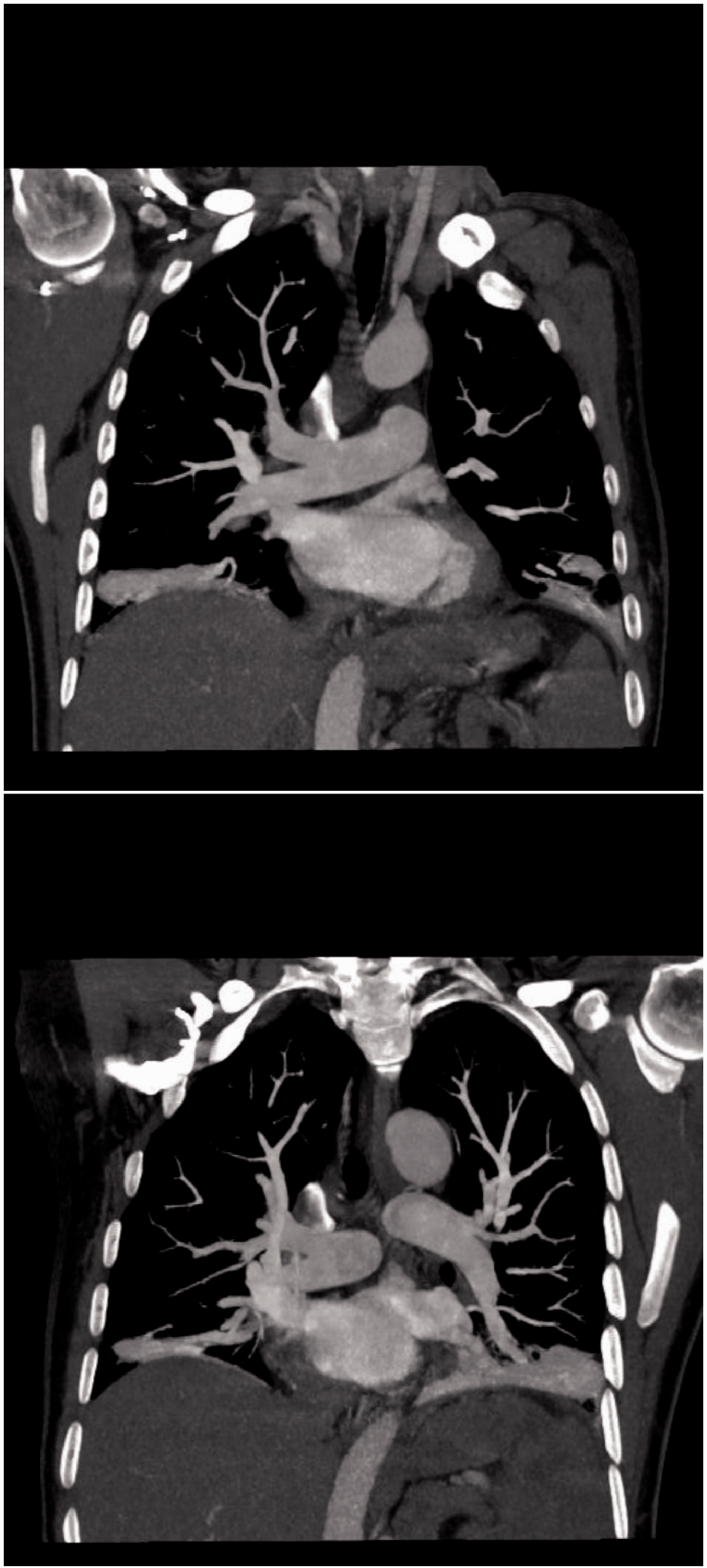
Representative pulmonary artery computed tomography angiography images in a 45-year old male patient diagnosed with splenic infarction caused by secondary erythrocytosis associated with obstructive sleep apnoea/hypopnoea syndrome. Images show no filling defect in the main pulmonary artery and in the left and right pulmonary arteries (upper image, right pulmonary artery; lower image, left pulmonary artery).

Representative enhanced computed tomography images of the abdomen in a 45-year old male patient diagnosed with splenic infarction caused by secondary erythrocytosis associated with obstructive sleep apnoea/hypopnoea syndrome. Images show single wedge or irregular low-density lesions in the spleen, with the base at the outer edge of the spleen and the tip pointing to the splenic hilum (upper image, coronal scan of spleen; lower image, axial scan of spleen).

Representative enhanced computed tomography images of the abdomen in a 45-year old male patient diagnosed with splenic infarction caused by secondary erythrocytosis associated with obstructive sleep apnoea/hypopnoea syndrome. Images show improvement of splenic infarction and a reduction in the splenic infarction area after 10 days of treatment (upper image, arterial phase scan of spleen; lower image, venous phase scan of spleen).
Bone marrow cytology at hospital admission suggested secondary polycythaemia. Assessment of the Janus kinase 2 (JAK2) gene showed the patient was negative for the V617F mutation, and thus polycythaemia vera was excluded. The PSG results revealed severe OSAHS with an apnoea hypopnoea index (AHI) value of 45. Mean oxygen saturation was 82%, and the minimum oxygen saturation was 69%. The percentage of time with an oxygen saturation < 90% was 99.8%. The patient remained in hospital for 2 weeks. A 1-month follow-up revealed that the patient’s abdominal symptoms had resolved.
Discussion
Embolization may occur in noncommunicating end-artery branches of the splenic artery, due to multiple factors mainly related to intra-splenic thrombosis, arteriosclerosis, embolism, microvascular embolization, and ectopic embolus detachment in infective endocarditis. 6 Any disease that causes increased blood viscosity can lead to limited tissue perfusion, ischaemia and thrombosis,1,2 and OSAHS has been associated with a variety of cardiovascular, cerebrovascular and thrombosis-related diseases.4,5 OSAHS provides the three elements of Virchow’s triad that are necessary for thrombosis, namely vascular endothelial damage, venous blood stasis and hypercoagulability. Hypoxaemia and hypercapnia are caused by intermittent hypoxia due to apnoea in patients with OSAHS, which may cause damage to vascular endothelial cells by excessive oxygen free radicals. The release of inflammatory factors, such as C-reactive protein, interleukin-6 and tumour necrosis factor-α, is increased in patients with OSAHS. The increased levels of cytokines and inflammatory transmitters may also cause damage to vascular endothelial cells and lead to further release of inflammatory factors, such as chemotactic cytokines, monocytes, adhesion molecules and growth factors.7,8 Accordingly, the secretory function of vascular endothelial cells may be impaired, making it difficult to regulate vascular tension and permeability, resulting in accelerated thrombosis. 9
The incidence of hyperlipidaemia is high in patients with OSAHS, and increased cholesterol levels may decrease the mobility of red blood cell lipid membranes, which may reduce the deformation ability of red blood cells and increase the adhesion activity, and consequently blood and plasma viscosity, in patients with OSAHS. In addition, nocturnal polyuria, hyperhidrosis and open-mouth breathing in patients with OSAHS often lead to more water loss during sleep, resulting in increased blood viscosity and haemodynamic changes in the morning. 10
In vivo levels of tissue factor, thrombin, fibrinogen, platelets, clotting factors (von Willebrand factor, factor VII, factor VIII, and factor V), and D-dimer content and activity, may be significantly increased in patients with OSAHS. Activated fibre protease and platelets convert fibrin monomer to fibrinogen in the plasma, and fibrinogen becomes a woven net, promoting the formation of a thrombus after platelet aggregation. At the same time, plasminogen activator inhibitor 1 (pai-1) inhibits fibrinolysis and increases thrombosis in patients with OSAHS. 11 Conservative treatment for splenic infarction is a suitable option in most cases. Splenic infarction caused by hypercoagulability may be treated with anticoagulant therapy, and thrombolysis and anticoagulation therapy should be provided in some cases. Splenectomy should be performed as soon as possible in patients with a large infarct area complicated with intra-splenic haematoma, splenic rupture, haemorrhagic shock and splenic abscess. 12 Finally, in patients diagnosed with OSAHS, continuous positive airway pressure (CPAP) treatment should be given as early as possible to reduce the risk of thrombosis and splenic infarction associated with OSAHS. 13
In conclusion, although splenic infarction may be rare, the present case highlights that splenic embolism should not be ignored as a potential complication of OSAHS.