
Abstract
Objective
The spleen is part of the lymphatic system and is one of the least understood organs of the human body. It is involved in the production of blood cells and helps filter the blood, remove old blood cells, and fight infection. Partial splenic artery embolization (PSE) is widely used to treat pancytopenia and portal hypertension. The efficacy of PSE for improving thrombocytopenia has been well demonstrated. In this study, we evaluated the splenic infarction ratio and platelet increase ratio after PSE.
Methods
Forty-five consecutive patients underwent PSE from January 2014 to August 2022. We retrospectively evaluated the splenic infarction volume and ratio after PSE and analyzed the relationship between the splenic infarction ratio and platelet increase ratio after PSE.
Results
The platelet increase ratio was correlated with the splenic infarction ratio after PSE. The cutoff value for the splenic infarction ratio with a two-fold platelet increase was 63.0%.
Conclusion
We suggest performance of PSE in patients with a splenic infarction ratio of 63% to double the expected platelet count.
Keywords
Introduction
The spleen, the largest secondary lymphoid organ in the body, is involved in a wide range of immunological functions alongside its roles in hematopoiesis and red blood cell clearance. The physical organization of the spleen allows it to filter pathogens and abnormal cells from the blood and facilitate low-probability interactions between antigen-presenting cells and cognate lymphocytes. 1 Hypersplenism can occur in association with a variety of conditions, including infectious diseases (such as malaria), infiltrative diseases, and liver disease. The spleen is enlarged in patients with portal hypertension caused by liver cirrhosis, extrahepatic portal obstruction, or Budd–Chiari disease. 2 Extrahepatic portal obstruction occurs in various diseases, such as portal venous thrombosis,3,4 pancreatic carcinoma, 3 or compression by tumors. 3 Hepatic tumors or cysts obstruct hepatic venous flow and cause portal hypertension.3,5 Although the spleen is usually enlarged, the severity of hypersplenism is not directly related to the size of the spleen or the severity of portal hypertension. Hypersplenism usually induces thrombocytopenia. 2 Thrombocytopenia can also make the management of numerous other conditions much more difficult and complex; such conditions include atrial fibrillation, cardiovascular complications, and continuation of tumor-related chemotherapy. 6 Partial splenic artery embolization (PSE) is a minimally invasive procedure that provides an alternative to splenectomy for the treatment of hypersplenism.7–10 PSE has fewer complications and is controllable, and the immune system is not significantly compromised because of sufficient retention of splenic tissue. PSE has been widely used because of its minimal invasiveness. 11 The influence of the splenic infarction rate after PSE remains controversial. 12 In this study, we evaluated the splenic infarction ratio after PSE and determined the appropriate splenic infarction ratio for increasing platelets.
Materials and Methods
This retrospective cohort study involved 45 consecutive patients who underwent PSE for hypersplenism caused by liver cirrhosis from January 2014 to August 2022. We evaluated the splenic infarction volume and infarction ratio and analyzed the relationship between the splenic infarction ratio and the platelet increase ratio after PSE.
We obtained written informed consent from all patients before their participation in this study. Data collection and analysis were performed according to the institutional guidelines and in accordance with the ethical standards of the Declaration of Helsinki. We obtained ethical approval from an accredited ethics committee, the Ethics Committee of Nippon Medical School Hospital (No. B-2021-459), and a consent form was signed by all patients prior to the start of the study. All patient details have been de-identified. The reporting of this study conforms to the STROBE guidelines. 13
Measurement of spleen volume and spleen infarction ratio after PSE
In all cases, the total spleen volume before PSE and the non-infarcted and infarcted spleen volumes after PSE were measured using a SYNAPSE VINCENT analyzer (Fujifilm Medical Co., Tokyo, Japan). 14 Delayed-phase images reconstructed at 5-mm intervals were used for these measurements. After importing pre- and post-PSE images into the SYNAPSE VINCENT analyzer, the splenic artery and regions of non-infarcted and infarcted spleen parenchyma were manually selected with a region of interest in each slice. The percentage of infarcted spleen was calculated as follows: (volume of infarcted spleen/total spleen volume after PSE) × 100% (Figure 1(a), (b)).

Calculation of splenic infarction volume and ratio using the SYNAPSE VINCENT analyzer. (a) Three-dimensional view and (b) Axial view.
PSE procedure
PSE was performed through the common femoral artery with a 4-Fr sheath (Super Sheath; Medikit, Tokyo, Japan) under local anesthesia. A 4-Fr guide catheter (SHC or C-MRT; Medikit) was inserted via the sheath. After celiac artery angiography, a microcatheter (Goldcrest Neo; Goldcrest Medic, Tokyo, Japan) was advanced to the hilum of the splenic artery via the guide catheter with the aid of a 0.018-inch microguidewire (Aqua VIII; Cardinal Health Japan, Tokyo, Japan). Branches of the splenic artery were then embolized with pieces of gelatin sponge (Serescue; Nippon Kayaku, Tokyo Japan), with the aim of achieving approximately 50% to 70% embolization of the spleen. To achieve this, embolization was performed progressively via repeated injections of embolic particles under angiographic control. Angiography was performed immediately after each injection. Supportive care after PSE included appropriate hydroelectrolytic infusion, systemic prophylaxis with antibiotics, and analgesics as needed.
Evaluation factors
We evaluated age, sex, morbidity (Clavien–Dindo grade >III complications), and length of hospital stay after PSE. We also evaluated the following laboratory data before PSE: serum total bilirubin, prothrombin time, platelet count, and white blood cell count. We also evaluated these data from 30 to 90 days after PSE.
Statistical analysis
Statistical analysis was performed using the statistical software package SPSS version 16.0 (SPSS Inc., Chicago, IL, USA). Categorical variables were compared using the χ2 test or Fisher’s exact test. Spearman’s correlation was used to assess the relationship between the splenic infarction ratio and platelet increase ratio from 1 month to 1 year after PSE. A receiver operating characteristic curve was applied to determine the cutoff value of variables for inducing an infarction ratio of ≥63.0%. Results with P values of <0.05 were considered statistically significant.
Results
We focused on patients who underwent PSE for hypersplenism caused by liver cirrhosis. The clinical characteristics of the patients who underwent PSE are shown in Table 1. The mean splenic infarction ratio was 50.9%. The platelet and white blood cell counts were significantly higher after PSE than before PSE. The platelet increase ratio in this study was correlated with the splenic infarction ratio. The correlation coefficient was 0.474, and the P value was 0.001 (Figure 2). According to the receiver operating characteristic analysis, the cutoff value for a two-fold increase in the platelet count was 63.0% (P = 0.001, area under the curve = 0.81, sensitivity = 75.0%, specificity = 75.8%) (Figure 3). We divided the patients into two groups: those with a splenic infarction ratio of > 63% (high infarction ratio group) and those with a splenic infarction ratio of < 63% (low infarction ratio group). The platelet and white blood cell counts were significantly higher in the high than low infarction rate group. There were no significant differences in morbidity between the two groups (Table 2).

Correlation between the splenic infarction ratio and the platelet increase ratio. A significant positive correlation was identified between the splenic infarction ratio and the platelet increase ratio after partial splenic artery embolization. The correlation coefficient was 0.474, and the P value was 0.001.
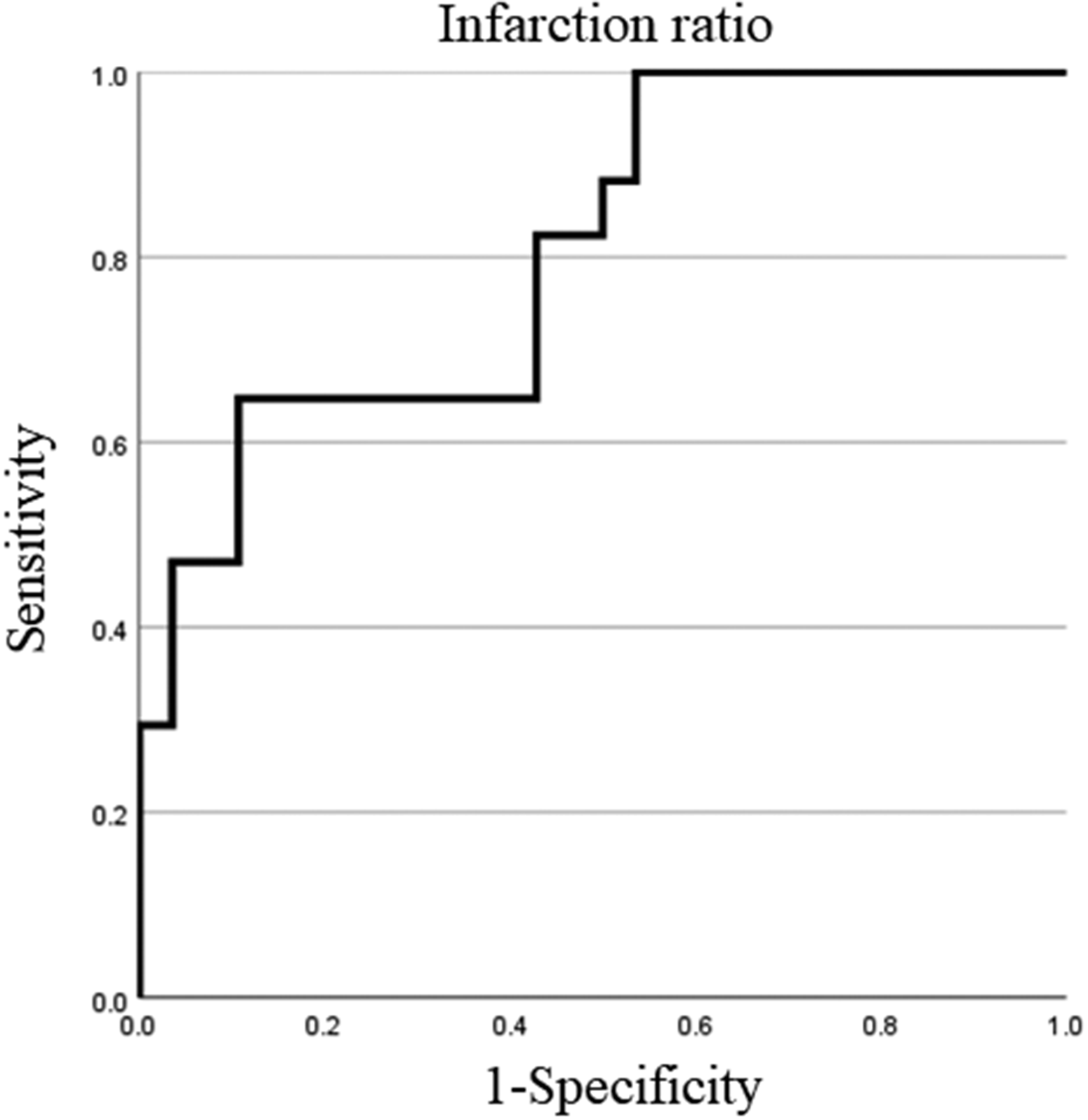
Receiver operating characteristic analysis for a two-fold increase in the platelet count and splenic infarction ratio. The cutoff value was 63.0% (P = 0.001, area under the curve = 0.81, sensitivity = 75.0%, specificity = 75.8%).
Clinicopathological characteristics of patients who underwent PSE (n = 45).
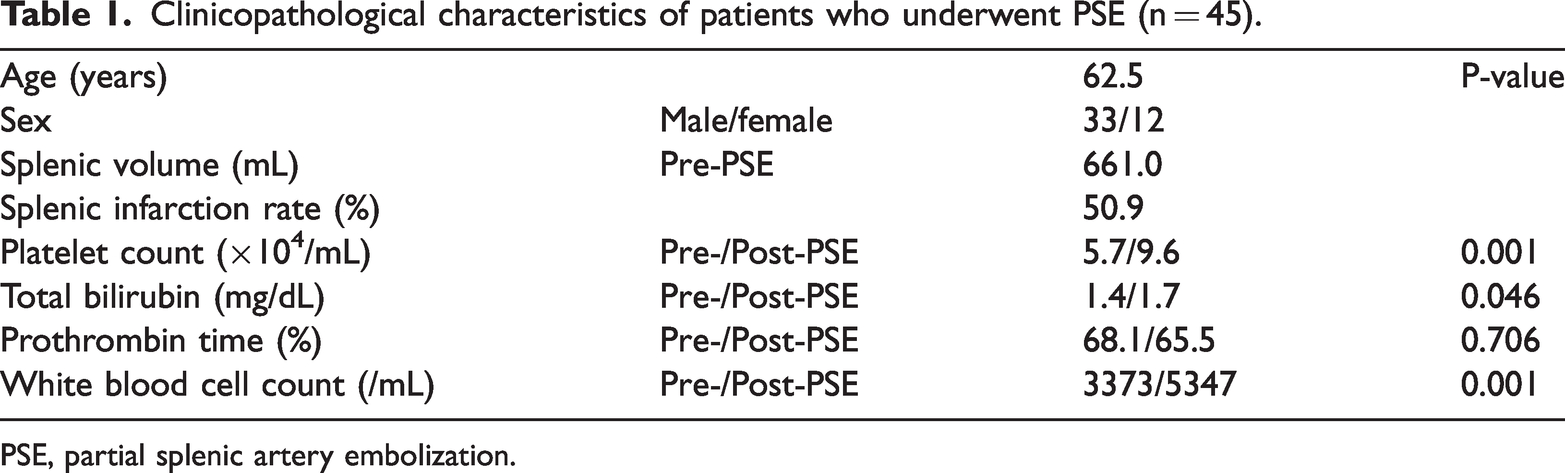
PSE, partial splenic artery embolization.
Clinicopathological findings in the high and low infarction ratio groups.
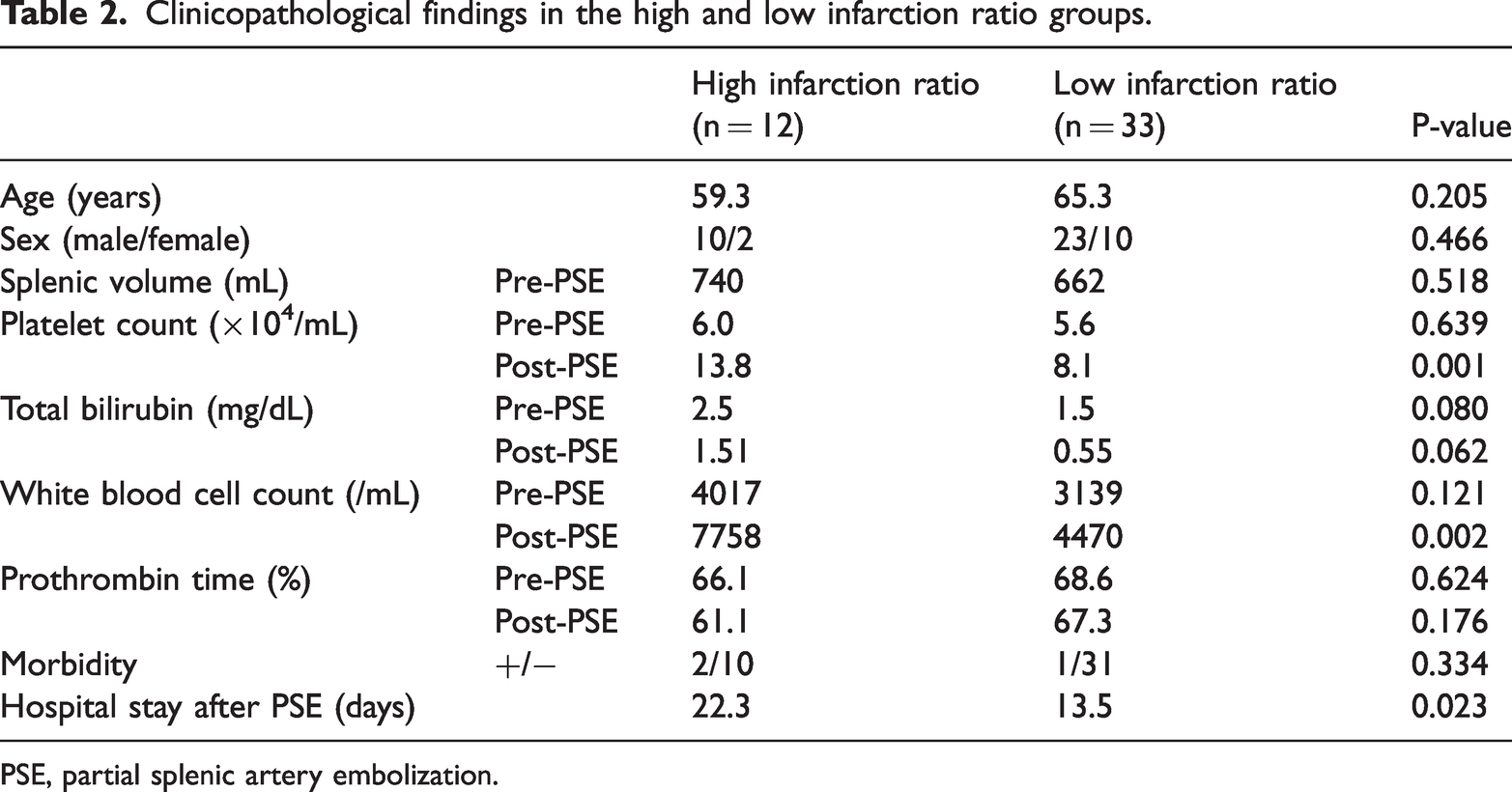
PSE, partial splenic artery embolization.
Discussion
In this study, we focused on PSE for hypersplenism and increases in platelets. Our study revealed that the splenic infarction ratio was correlated with the platelet increase ratio after PSE. The receiver operating characteristic analysis yielded a cutoff value of 63.0% for the splenic infarction ratio to achieve a two-fold increase in the platelet count. Thrombocytopenia in patients with cirrhosis is reportedly caused by an increased platelet pool in the enlarged spleen.15–17 The increase in the platelet count after PSE has been suggested to be caused by a reduction in the platelet pool in the diminished spleen and enhanced platelet destruction in the spleen through immunological mechanisms.18,19 In some studies, the increase in the platelet count was positively correlated with the splenic infarction ratio,18,20 and the splenic infarction ratio was a critical factor for improving thrombocytopenia after PSE. 20 A sufficient increase in the platelet count (≥60.0 × 109/L) at 1 year after PSE was achieved with a splenic infarction ratio of 64.3%. 20 Sangro et al. 21 noted that relapse of hypersplenism was associated with a splenic embolization rate of ≤50%, whereas relapse seldom occurred if the embolization rate was >50%. Some reports have also indicated that the splenic infarction ratio is crucial for long-term improvement of thrombocytopenia.22,23 By contrast, Han et al. 24 reported that there were no therapeutic differences among patients with splenic infarction ratios of 50%, 70%, and 80%. Another report revealed that the increase in the platelet count was dependent on the reduction in splenic volume. 25 A conclusion has not been reached, and these findings remain controversial. The target splenic infarction rate typically ranges from 50% to 80% for PSE procedures. 26 Some reports have revealed that the splenic infarction volume, not the splenic infarction rate, may be a determining factor for an increased platelet count after PSE. 25 In addition, a massive infarcted volume of >540 mL in a single PSE procedure could be a significant risk factor for severe postoperative complications, such as splenic abscess formation, refractory ascites, or pleural effusion. 27
Our study had two main limitations. First, we only investigated the factors correlated with an increase in the platelet count after PSE during a follow-up period of a few months. A further study with a longer-term follow-up observation is needed to confirm our findings. Second, although our study presented suitable cutoff values of the ratio and volume of splenic infarction for an adequate increase in the platelet count, assessing the precise extent of splenic embolization is still difficult.
In this study, we revealed the segmental volume of the spleen and a suitable splenic infarction ratio. We suggest embolizing the lower and middle segments of the spleen to achieve a 63% splenic infarction ratio. Moreover, we suggest calculating the pretreatment segmental volume of the spleen by computed tomographic volumetry and determining the splenic infarction ratio preoperatively.
Conclusion
The increase in the platelet count after PSE is correlated with the splenic infarction ratio. A suitable splenic infarction ratio is 63%, and we suggest performing PSE to achieve a splenic infarction ratio of 63% and thus increase the platelet count by two-fold.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231190967 - Supplemental material for Evaluation of splenic infarction ratio and platelet increase ratio after partial splenic artery embolization
Supplemental material, sj-pdf-1-imr-10.1177_03000605231190967 for Evaluation of splenic infarction ratio and platelet increase ratio after partial splenic artery embolization by Junji Ueda, Yasuhiro Mamada, Nobuhiko Taniai, Masato Yoshioka, Akira Matsushita, Satoshi Mizutani, Youichi Kawano, Tetsuya Shimizu, Tomohiro Kanda, Hideyuki Takata, Hiroyasu Furuki, Yuto Aoki, Manpei Kawashima, Toshiyuki Irie, Takashi Ohno, Takahiro Haruna and Hiroshi Yoshida in Journal of International Medical Research
Footnotes
Availability of data and materials
The datasets used and/or analyzed in the current study are available from the corresponding author on reasonable request.
Author contributions
Junji Ueda and Hiroshi Yoshida designed the study and wrote the report. Yasuhiro Mamada, Nobuhiko Taniai, Masato Yoshioka, Akira Matsushita, Satoshi Mizutani, Youichi Kawano, Tetsuya Shimizu, Tomohiro Kanda, Hideyuki Takata, Hiroyasu Furuki, Yuto Aoki, Manpei Kawashima, Toshiyuki Irie, Takashi Ohno, and Takahiro Haruna summarized the clinical data. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declare no conflict of interest.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Nippon Medical School Hospital (protocol identification number: B-2021-459). We obtained written informed consent from all patients before their participation in this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.