
Abstract
Objective
This study aimed to examine the clinical value of a decrease in hemoglobin concentration (HC) after the onset of sepsis for predicting occurrence of necrotizing enterocolitis (NEC) in preterm infants with late-onset sepsis.
Methods
We performed a retrospective cohort study between January 2015 and January 2020. Premature neonates (gestational age <37 weeks) with late-onset sepsis (age >3 days) were enrolled. According to the degree of reduction in HC, neonates were divided into the non-decrease group, mild decrease group, and severe decrease group. Demographic data, perinatal conditions, blood cell count analysis, blood culture, and treatment measures were compared.
Results
Eighty premature infants with sepsis were studied. The mortality rate and incidence of NEC were significantly higher in the severe decrease group than in the non-decrease and mild decrease groups. Significant differences were observed in the decrease in HC, red blood cell transfusion, and ventilator application between the NEC and non-NEC groups. A significant decrease in HC was an independent risk factor for NEC in preterm infants with sepsis.
Conclusion
A significant decrease in HC is an independent risk factor for NEC and may predict the occurrence of NEC in preterm infants with sepsis.
Keywords
Introduction
Neonatal necrotizing enterocolitis (NEC) is one of the most common gastrointestinal diseases of newborns, and it mostly occurs in premature infants and in those with low birth weight. NEC is a main cause of neonatal death, with a mortality as high as 20% to 30%. 1 Even surviving children with NEC often have short-term and long-term complications, such as intestinal stenosis, short bowel syndrome, and neurological sequelae,2–4 which seriously affect their quality of life. The etiology and pathogenesis of NEC are still unclear. Many factors are closely related to occurrence of NEC and infection plays an important role in NEC.5,6 A total of 34% to 57% of children with NEC suffer from sepsis before onset.7,8
Studies have shown that sepsis is often complicated by anemia. 9 Therefore, the occurrence of sepsis is often accompanied by varying degrees of a reduction in hemoglobin concentration (HC). A decrease in HC may cause ischemic and hypoxic damage to the body, causing redistribution of blood and microcirculation disorders. This may eventually have an adverse effect on the intestinal tract of children, but this is limited to theoretical speculation. Regrettably, there has been no research on the effect of the degree of a reduction in HC on the occurrence of NEC in preterm infants.
Therefore, this study aimed to examine effective indicators, including HC, of secondary NEC in preterm infants with sepsis. We also hoped to identify effective indicators that are easily available and cause little damage to children in clinical work. Our current research is novel because it mainly focused on whether the degree of a reduction in HC affects the occurrence of NEC in preterm infants with sepsis.
Materials and methods
Participants
This was a retrospective cohort study that was conducted in the neonatal intensive care unit. Premature neonates (gestational age <37 weeks) with late-onset sepsis (age >3 days) who were diagnosed by a neonatal specialist at the Southwest Hospital of the First Hospital Affiliated to Army Medical University, China between January 2015 to January 2020 were enrolled in this study. Diagnosis was made in accordance with the Guidelines for the Diagnosis and Treatment of Neonatal Sepsis (2003). 10 The diagnostic criteria for sepsis were neonates with fever or a low body temperature, less crying, a poor mental response, poor feeding, and other clinical manifestations. An additional criterion was that a blood culture or sterile body cavity cultured pathogenic bacteria. Furthermore, for the diagnosis of sepsis, neonates needed to have the above-mentioned clinical manifestations and at least two of the following: (1) white blood cell (WBC) count < 5 × 109/L or an increased WBC count (age ≤3 days, WBC >25 × 109/L; age > 3 days, WBC >20 ×109/L); (2) immature neutrophils/total neutrophils ≥0.16; (3) platelet count < 100 ×109/L; and (4) C-reactive protein levels ≥8 mg/L. Based on the degree of reduction in HC, patients were divided into the non-decrease group, mild decrease group (HC decrease <15 g/L), and severe decrease group (HC decrease ≥15 g/L). Based on whether NEC developed after sepsis, premature infants were divided into the NEC and non-NEC groups. For diagnosis of NEC, we referred to the fourth edition of Practical Neonatology. 11 NEC was diagnosed using the following criteria: neonates with bloating, bloody stools, vomiting, drowsiness, unstable body temperature, apnea, bradycardia, and other symptoms; and a X-ray suggested signs of accumulation of intestinal wall gas, accumulation of portal vein gas, or intestinal perforation. None of the included cases used probiotics. Patients were excluded for the following reasons: (1) intrauterine infection led to early-onset sepsis (age ≤3 days), meconium aspiration syndrome, and neonatal scleroderma; (2) presence of genetic metabolic diseases and congenital deformity; (3) anemia caused by intracranial hemorrhage (when the HC was significantly reduced, we performed a brain ultrasound examination of the neonate to determine whether there was intracranial hemorrhage), gastrointestinal hemorrhage, or pulmonary hemorrhage; and (4) incomplete case data.
This study was approved by the Ethics Committee of the First Hospital Affiliated of Army Medical University (Chongqing, China; KY2020065, April 2020). Informed consent for participation in the study was obtained from the legal guardians. All methods were performed in accordance with the relevant guidelines and regulations.
Data collection
Demographic data were obtained from electronic medical records and included the mother’s prenatal condition, such as whether there was maternal hypertension, diabetes, meconium contamination of amniotic fluid, and premature rupture of the membranes. Additionally, information of children, such as sex, gestational age, birth weight, age of onset, blood cell count analysis, blood culture, and treatment measures, were recorded. When patients first showed the symptoms of sepsis (e.g., fever, poor mental response, and poor feeding), blood samples that were collected for the first time were examined. Laboratory parameters, such as the WBC count, HC, platelet count, decrease in HC, and blood culture results, were measured. A decrease in HC was the result of comparing the most recent HC before sepsis with the HC at the time of sepsis.
Statistical analysis
SPSS 20.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Categorical variables are presented as absolute number and percentage, and were compared using the chi-square test and Fisher’s exact test. Measurement data are expressed as mean ± standard deviation. One-way analysis of variance was performed for multi-group comparisons. An F-test was performed in cases of homogeneity of variance and Welch’s t-test was performed in cases of heterogeneity of variance. Logistic regression analysis was used to assess independent factors of NEC. Sensitivity and specificity were determined by analyzing the area under the receiver operating characteristic (ROC) curve. P < 0.05 was considered significant.
Results
Comparison between the non-decrease, mild decrease, and severe decrease groups
Baseline characteristics
Eighty patients were included in the study. There were no differences in the interval of blood sample collection and HC before sepsis between the non-decrease, mild decrease, and severe decrease groups. We analyzed the clinical data of children with sepsis among the three groups. The rates of mortality and NEC were significantly different among the three groups (both P < 0.05). The mortality rate and the incidence of NEC in the severe decrease group were significantly higher than those in the non-decrease and mild decrease groups. The main cause of death was severe complications of sepsis, such as septic shock, multiple organ dysfunction syndrome, and disseminated intravascular coagulation, which occurred before discharge. There were no significant differences in sex, gestational age, birth weight, and age of onset (Table 1).
Baseline clinical characteristics of the non-decrease, mild decrease, and severe decrease groups.
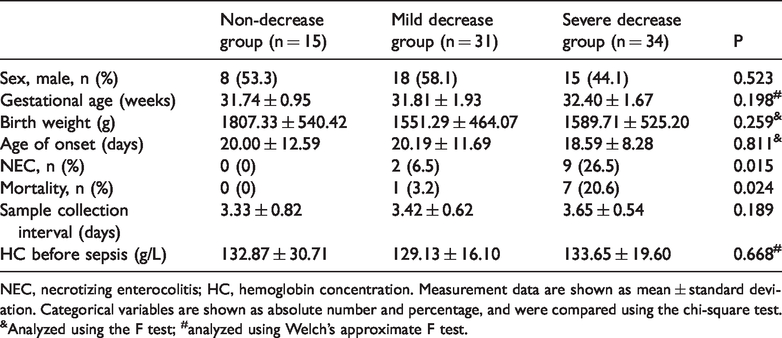
NEC, necrotizing enterocolitis; HC, hemoglobin concentration. Measurement data are shown as mean ± standard deviation. Categorical variables are shown as absolute number and percentage, and were compared using the chi-square test. &Analyzed using the F test; #analyzed using Welch’s approximate F test.
Differences in HC
A significant difference was observed in HC among the three groups (P = 0.003). The HC was lowest in the severe decrease group and highest in the non-decrease group. There were no significant differences in the WBC count, platelet count, and positive rate of blood culture among the groups (Table 2).
Comparison of complete blood count analysis and blood culture among the non-decrease, mild decrease, and severe decrease groups.

WBC, white blood cell; PLT, platelet; HC, hemoglobin concentration. Measurement data are shown as mean ± standard deviation. Categorical variables are shown as absolute number and percentage, and were compared using the chi-square test. &Analyzed using the F test; #analyzed using Welch’s approximate F test.
Comparison between the NEC and non-NEC groups
Baseline characteristics
The mean occurrence time of NEC after sepsis was 4.55 ± 4.71 days. There were no significant differences in the interval of blood sample collection and HC before sepsis between the NEC and non-NEC groups.. There were also no significant differences in other baseline data, such as sex, gestational age, birth weight, age of onset, and the perinatal situation, among the NEC and non-NEC groups (Table 3). There was no significant difference in the number of cases of septic shock between the two groups.
Baseline clinical characteristics of the NEC and non-NEC groups.

NEC, necrotizing enterocolitis; PROM, premature rupture of the membranes > 18 hours; SGA, small for gestational age; HC, hemoglobin concentration. Categorical variables are shown as absolute number and percentage, and were compared using the chi-square test or Fisher’s exact test. *Analyzed by Fisher’s exact test.
Differences in the decrease in HC, red blood cell transfusion, and ventilator application
The decrease in HC, and rates of red blood cell transfusion and ventilator application were significantly lower in the non-NEC group than in the NEC group (all P < 0.05). There were no significant differences in the WBC count, platelet count, decrease in HC, and positive rate of blood culture among the two groups (Table 4).
Comparison of laboratory indicators and treatment measures between the NEC and non-NEC groups.

NEC, necrotizing enterocolitis; WBC, white blood cell; PLT, platelet; HC, hemoglobin concentration. Measurement data are shown as mean ± standard deviation. Categorical variables are shown as absolute number and percentage, and were compared using the chi-square test or Fisher’s exact test. *Analyzed using Fisher’s exact test.
Independent risk factors for NEC in preterm infants with sepsis
Binomial stepwise logistic regression was used to determine independent risk factors for NEC in preterm infants with sepsis. Whether NEC occurred was the dependent variable, and other indicators, including the decrease in HC, red blood cell transfusion, and ventilator application, were used as independent variables to test whether each factor had a significant effect on NEC. We found that a significant decrease in HC (odds ratio = 1.160, P = 0.001) was an independent risk factor for NEC in preterm infants with sepsis (Table 5).
Logistic regression analysis results.

HC, hemoglobin concentration; SE, standard error; OR, odds ratio; CI, confidence interval.
High predictive value of a decrease in HC for NEC in preterm infants with sepsis
ROC curve analysis of sepsis showed that the area under the curve was 0.858 and the negative predictive value was 98% for a decrease in HC. This finding suggests that a decrease in HC may predict the occurrence of NEC in premature infants with sepsis (Table 6, Figure 1).
Receiver operating characteristic curve of the decrease in HC for predicting neonatal necrotizing enterocolitis in sepsis.

HC, hemoglobin concentration; AUC, area under the curve; PPV, positive predictive value; NPV, negative predictive value.
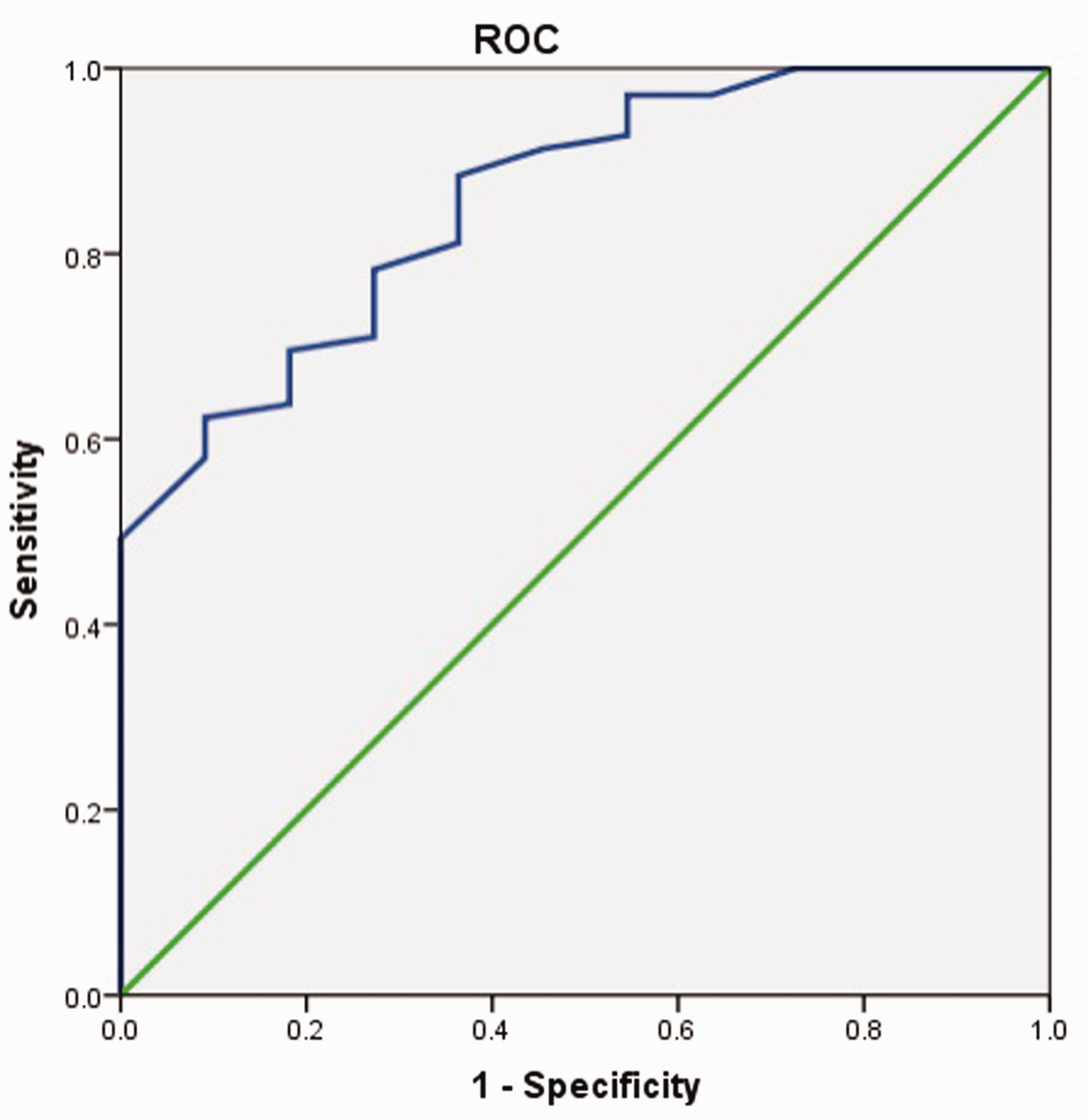
ROC curve of the decrease in hemoglobin concentration for predicting necrotizing enterocolitis in sepsis. ROC, receiver operating characteristic.
Discussion
The neonatal immune system is immature, and sepsis often rapidly develops from subclinical symptoms to severe systemic infection symptoms. This causes systemic system organ involvement and damage, resulting in a variety of complications, which significantly increase the mortality rate in children. NEC is the most common among these complications. Studies have shown that sepsis is a risk factor for NEC and it significantly increases the incidence of NEC.7,8 Therefore, the most important approach is to perform early assessment of the occurrence of NEC in preterm infants with sepsis and intervene as soon as possible to reduce morbidity and mortality.
C-reactive protein, procalcitonin, blood culture, and other indicators have been commonly used clinically to assess the severity and prognosis of sepsis.12,13 Unfortunately, many basic hospitals in developing countries do not carry out monitoring of C-reactive protein and procalcitonin levels. Additionally, these indicators often require repeated collection of venous blood for monitoring, which not only increases the pain of the child, but also the financial burden of the family. Sepsis is often accompanied by anemia, and dynamic monitoring of the above-mentioned indicators may further aggravate the severity of anemia. As a basic test that is performed in all levels of hospitals, blood cell analysis has the characteristics of little blood required and little damage to children. Therefore, effective indicators in whole blood cells analysis are required to predict the occurrence of NEC in preterm infants with sepsis. Our study showed that the incidence of NEC and the mortality rate in the severe decrease group were significantly higher than those in the non-decease and mild decrease groups. Because of the significant decrease in HC, the degree of anemia in the severe decrease group was greater than that in the non-decrease and mild decrease groups. Many studies have confirmed that anemia is a risk factor for NEC.14–17 Another study also showed that the incidence of NEC in children with sepsis combined with anemia was closely related to the degree of anemia. 18 Furthermore, the incidence of NEC in children with moderate or more severe anemia was higher than that in those without anemia or mild anemia. Singh et al. 19 showed that a lower hematocrit was associated with an increased odds of NEC, which is similar to our study. However, these previous studies mainly focused on healthy newborns, not children with late-onset sepsis, and these conclusions are mostly qualitative indicators, which lack quantitative results. In our study, further comparison showed that the decrease in HC in the NEC group was significantly higher than that in the non-NEC group. This finding suggested that a decrease in HC was a risk factor for NEC in preterm infants with late-onset sepsis. This indicator is easy to obtain clinically, which does not require additional drawing of blood and reduces damage to children. Results of HC can also be rapidly obtained, and therefore, children can be treated in time. Furthermore, measurement of HC has the characteristics of economy and convenience.
Logistic regression analysis in the present study showed that a decrease in HC was an independent predictor for NEC in preterm infants with sepsis. By comparing the ROC curve of a decrease in HC, we found that the area under the curve was 0.858, which suggests that a decrease in HC (cut-off value: 15.0) may predict the occurrence of NEC in preterm infants with sepsis. Although the underlying mechanism of this finding is still unclear, a possible pathophysiological explanation is that bacteria and toxins directly damage the intestinal mucosa after occurrence of sepsis. Another possibility is through activation of pro-inflammatory factors, such as platelet-activating factor and tumor necrosis factor, which results in an imbalance of pro-inflammatory and anti-inflammatory mechanisms in the body and causes intestinal damage. A significantly reduced HC causes the blood’s oxygen carrying capacity to fall below the level required for tissue growth, resulting in a large amount of anaerobic metabolism and increase in by-products (e.g., lactic acid). 20 Furthermore, a significant decrease in HC after the occurrence of sepsis will mostly lead to greater anemia in children, which may impair delivery of intestinal oxygen, 21 leading to intestinal mucosal ischemia and hypoxic injury.19,22 Intestinal wall ischemia and hypoxia during anemia can cause an intestinal inflammatory reaction. A large number of inflammatory cytokines are activated, resulting in reduced production of epidermal growth factor and increased production of platelet-activating factors and free radicals. This situation aggravates intestinal mucosal damage, eventually causing NEC. 23
Our study also showed that the rate of red blood cell transfusion in the NEC group was higher than that in the non-NEC group. Many studies have shown that transfusion of red blood cells leads to occurrence of NEC,24,25 and increases the chance of surgery in children with NEC and reduces the survival rate. 26 A study on blood transfusion after sepsis in children showed that after sepsis-related anemia, there was a significantly higher incidence of acute respiratory distress syndrome and acute lung injury in the liberal transfusion group compared with the restrictive strategy group. 27 Moreover, the mortality rate was significantly higher in the liberal transfusion group, and liberal transfusion might have been associated with a worse outcome. Other studies have shown that transfusion of red blood cells may increase the mortality rate of critically ill patients.28,29 Anemia associated with sepsis is not always true anemia, and sometimes it may be caused by blood dilution related to fluid load.30,31 Therefore, after occurrence of sepsis, even if the HC is reduced, clinicians need to determine whether a blood transfusion is required on the basis of the condition of children.
Limitations
This study has some limitations. The incidence of NEC in preterm infants with sepsis in our hospital is not as high as that reported in the literature.7,8 Therefore, the sample size of the NEC group was small, and conclusions must be further validated with larger sample sizes. Additionally, the retrospective nature of the study is a limitation because only blood cell count analysis and blood culture at the initial stage of the disease were performed, and the results of other onset times were not recorded.
Conclusion
Measurement of the decrease in HC in the neonatal intensive care unit is easily accessible, fast, and affordable, and represents a useful tool for predicting the occurrence of NEC in preterm infants with late-onset sepsis.