
Abstract
Objective
To study the role of vitamin E in stroke-associated pneumonia.
Methods
We selected 183 patients with stroke-related pneumonia who were divided into different nutrition groups according to the Mini Nutritional Assessment score. Patients were then administered different doses of vitamin E.
Results
CD55 and CD47 levels in patients taking vitamin E across different nutrition score groups were better than those in patients who did not use vitamin E. The levels of CD55 and CD47 and the duration of hospitalization were better in the high-dose vitamin E group than in the low-dose vitamin E group.
Conclusion
Vitamin E may have an auxiliary therapeutic effect in patients with stroke-associated pneumonia.
Keywords
Background
Hilker 1 first proposed the concept of post-stroke-associated pneumonia (SAP) in 2003. SAP is a clinically diagnosed acute stroke characterized by cough, fever, expectoration, and other symptoms. Pneumonia is diagnosed according to standard diagnostic procedures. Poor immune function caused by malnutrition is an important factor in the course of SAP. According to the aforementioned information, SAP differs from community-acquired pneumonia because stroke has essential negative effects on the immune characteristics of leukocytes. 2
Neutrophils play an important role in the pathological process of pulmonary infection. 3 It is intuitive that neutrophil accumulation and migration in tissues are correlated with patient symptoms and disease development. CD47, a cell surface glycoprotein, plays a pivotal role in modulating neutrophil (polymorphonuclear neutrophil [PMN]) migration across epithelial tissue. 3 CD47 positively regulates PMN transmigration by regulating protein–protein interactions via other mechanisms that are more compatible with intracellular signaling events.4,5 CD55, also known as decay-accelerating factor, is believed to promote the release of PMNs to the apical space, implying that CD55 levels can accurately reflect the function of neutrophils. 6
A recent study demonstrated that vitamin E is an effective modulator of the PMN response. In addition, vitamin E is a potential nutritional intervention for treating pneumococcal infection, 7 but few reports have examined the effect of vitamin E against SAP in the immunosuppressed state.
Patients and methods
Ethics approval and consent to participate
The study was approved by the Qingdao Municipal Hospital Research Ethics Committee (Qingdao, China) on December 2, 2018. All patients were fully informed about the purpose and procedures of the study, and the patients provided written consent to participate (No. 2018015). The experiment was successfully registered in October 2019 (http://www.chictr.org.cn/index.aspx, registration number: ChiCTR1900026362).
Subjects
This prospective analysis included patients with acute cerebral infarction who were treated at the Neurology Department of Qingdao Municipal Hospital Group in 2019. This study prospectively assigned participants to different treatment groups randomly (coin tosses). The included patients experienced had cerebral infarction within the previous 72 hours before admission. All patients were ambulatory. All patients with a cough after drinking water were fed using a gastric tube.
The admission criteria for patients who experienced SAP included the presence of at least one of the following findings: fever with a body temperature greater than 37°C; peripheral white blood cell count greater than 10 × 109/L with or without a nuclear left shift; new cough and respiratory purulent secretions with or without chest pain; sputum bacterial smear or culture finding of pathogenic bacteria; or chest X-ray examination finding of new or progressive pulmonary exudation, change, or cavity, or pleural exudation.
The exclusion criteria were as follows: transient ischemic attack; stroke onset more than 72 hours prior to admission or less than 24 hours after admission or death; clinical symptoms of pulmonary infectious diseases (such as tuberculosis, lung cancer, severe heart failure, pulmonary edema, pulmonary embolism, pulmonary atelectasis or infection, and interstitial lung disease); multidrug-resistant bacterial infection; hepatorenal failure or end-stage chronic consumptive disease; Glasgow score of less than 8 points in comatose patients; blood, plasma, or albumin transfusion within 1 month before admission; definite chronic bronchitis and lung infection before disease onset; and serious diseases of the heart, liver, kidneys, lungs or other important organs. Patients with severe pneumonia as indicated using the Pneumonia Severity Index were also excluded.
Subgroups and treatment
Based on the Mini Nutritional Assessment (MNA) score, the patients were divided into three groups: good nutrition group (Group A), nutritional risk group (Group B) and dystrophy group (Group C). Patients in Group A were divided into subgroups A1 (control group), A2 (50 mg/day vitamin E), and A3 (100 mg/day vitamin E). Patients in Group B were divided into subgroups B1 (control group), B2 (50 mg/day vitamin E), and B3 (100 mg/day vitamin E). Patients in Group C were divided into subgroups C1 (control group), C2 (50 mg/day vitamin E), and C3 (100 mg/day vitamin E).
Our group used intestinal nutrients (NCE Group, Hong Kong). The high-energy nutrient solution prepared by a nutritionist and clinician in our hospital according to the patient’s condition, weight nutritional status, and caloric requirement was provided according to the standard of 83.68 to 125.52 kJ/kg·day (1 kcal = 4.184 kJ). Nutrition was supervised by a full-time nurse using the gravity drip method, and the initial drip rate was 40 to 60 mL/hour. If there was no reflux, diarrhea, bloating, and other adverse reactions, the rate was increased to 100 to 125 mL/hour after 2 to 3 days. The dosage was up to 500 mL/day.
The patients in each group received vitamin E through a stomach tube on the day of admission. All patients received conventional treatments for cerebral infarction and infection. In addition, all patients were provided necessary nutritional support under the guidance of the Nutrition Department. The experimental procedure was approved by the Qingdao Municipal Hospital Ethics Committee (Appendix 1).
Experimental measures
CD47 and CD55: Blood flow cytometry analysis was used to measure CD47 and CD55 levels in whole blood at 7:00 a.m. (after 7 hours of fasting) on the second day after admission and on the day before discharge. The length of hospitalization was recorded for each patient in each group. The cerebral infarction volume (cm3) was calculated using the following formula: cerebral infarction volume = (length × width × CT-positive layer × thickness)/2. 7
All data were analyzed using SPSS version 16.0 software (SPSS, Inc., Chicago, IL, USA). Data were normally distributed and expressed as the mean ± SD. The means from two sample groups were compared using a t-test. When data did not meet the requirements for variance analysis, multiple samples were analyzed using the rank-sum test.
The sample size was calculated using the following formula:

CD47:
Using the aforementioned values, n1 and n2 were demonstrated to equal 9.31, which is approximately 10.
Results
The study included 183 patients who developed pneumonia after acute cerebral infarction who met the inclusion and exclusion criteria.
Good nutritional support group
There were no significant differences among subgroups A1, A2, and A3 regarding gender, age, blood pressure, the number of patients with coronary heart disease, cholesterol or very low-density lipoprotein (VLDL) levels, the MNA score, or cerebral infarction volume. The length of hospitalization was shorter in subgroup A2 than in subgroup A1 (P < 0.05). The length of hospitalization did not differ between subgroups A2 and A3 (Table 1).
Clinical data for each subgroup in Group A.

Data are presented as the mean ± SD or number.
VLDL, very low-density lipoprotein; MNA, Mini Nutritional Assessment.
▲ compared with subgroup A1, P < 0.05.
There were no significant differences in CD47 levels among subgroups A1, A2, and A3 before vitamin E administration. After vitamin E administration, CD47 levels were significantly higher in subgroups A2 and A3 than in subgroup A1 (both P < 0.05), and its levels were also higher in subgroup A3 than in subgroup A2 (P < 0.05, Figure 1).

Comparison of CD47 levels before and after administration in Group A.
CD55 levels did not differ among the subgroups before vitamin E administration. After vitamin E administration, CD55 levels were lower in subgroups A2 and A3 than in subgroup A1 (both P < 0.05), and its levels were also significantly lower in subgroup A3 than in subgroup A2 (P < 0.05, Figure 2).

Comparison of CD55 levels before and after administration in Group A.
Nutritional risk group
There were no significant differences among subgroups B1, B2, and B3 regarding gender, age, blood pressure, the number of patients with coronary heart disease, cholesterol or VLDL levels, the MNA score, or the cerebral infarction volume. The length of hospitalization was significantly shorter in subgroup B2 than in subgroup B1 (P < 0.05). The length of hospitalization did not differ between subgroups B2 and B3 (Table 2).
Clinical data for each subgroup in Group B.

Data are presented as the mean ± SD or number.
VLDL, very low-density lipoprotein; MNA, Mini Nutritional Assessment.
▲ compared with subgroup B1, P < 0.05; ◇ compared with subgroup B2, P < 0.05.
CD47 levels were similar among the subgroups before vitamin E administration. After vitamin E administration, CD47 levels were significantly higher in subgroup B than in subgroups B1 and B2 (both P < 0.05), and its levels were also higher in subgroup B2 than in subgroup B1 (P < 0.05, Figure 3).
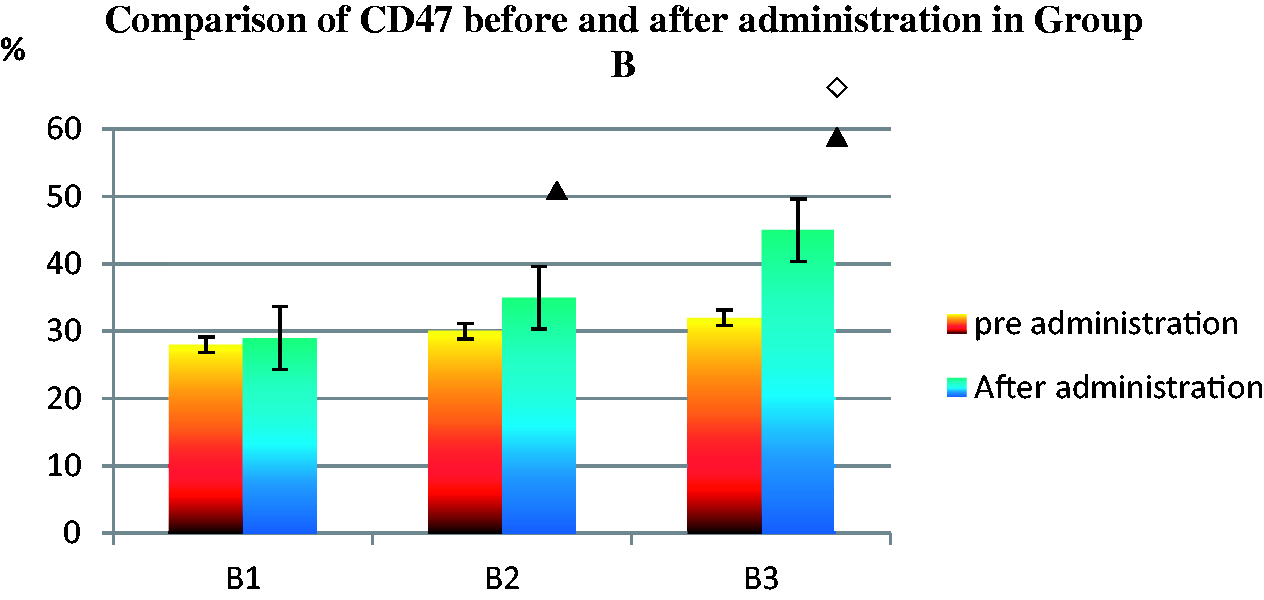
Comparison of CD47 levels before and after administration in Group B.
CD55 levels did not differ among subgroups B1, B2, and B3 before vitamin E administration. After vitamin E administration, CD55 levels were lower in subgroup B2 than in subgroup B1 (P < 0.05). In addition, CD55 levels were lower in subgroup B3 than in subgroups B1 and B2 (both P < 0.05, Figure 4).
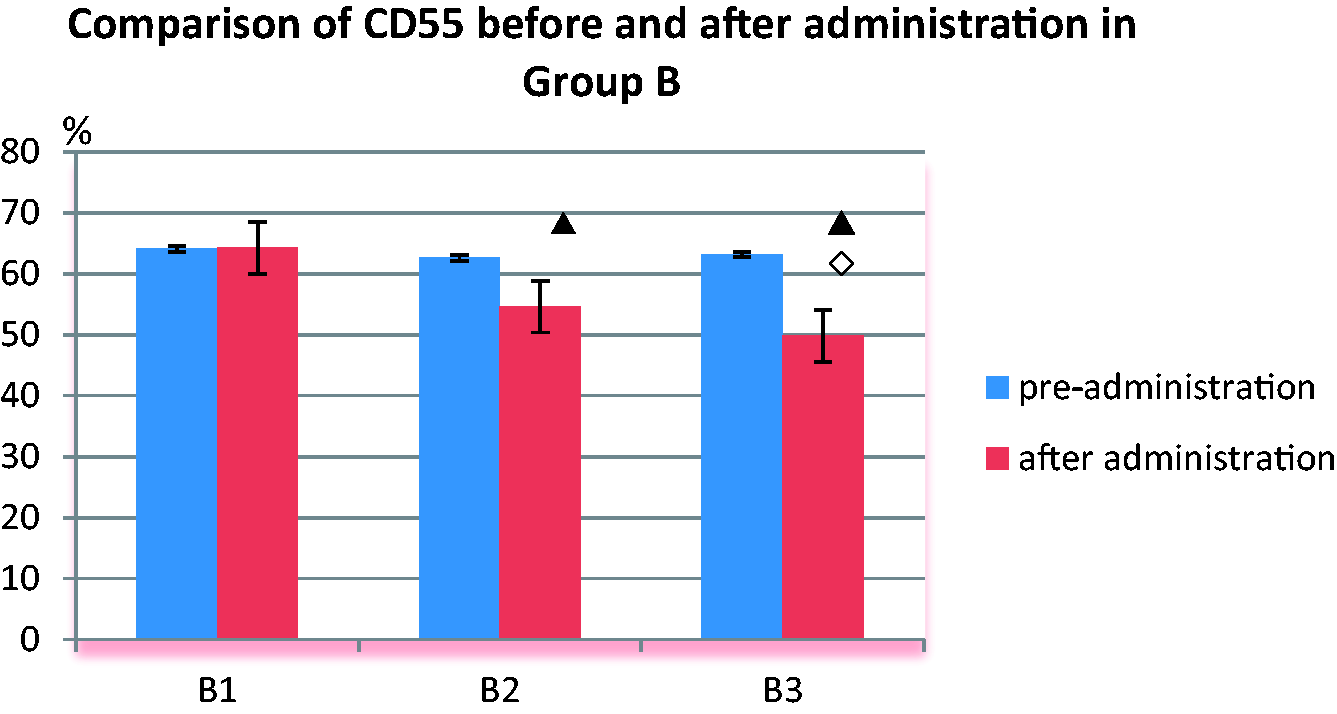
Comparison of CD55 levels before and after administration in Group B.
Dystrophy group
There were no significant differences among subgroups C1, C2, and C3 in terms of gender, age, blood pressure levels, the number of patients with coronary heart disease, cholesterol or VLDL levels, the MNA score, or the cerebral infarction volume. The length of hospitalization was significantly shorter in subgroup C2 than in subgroup C1 (P < 0.05), whereas the length of hospitalization did not differ between subgroups C2 and C3 (Table 3).
Clinical data for each subgroup in Group C.

Data are presented as the mean ± SD or number.
VLDL, very low-density lipoprotein; MNA, Mini Nutritional Assessment.
▲ compared with subgroup C1, P < 0.05; ◇ compared with subgroup C2, P < 0.05.
Although CD47 levels did not differ among these subgroups prior to vitamin E administration, its levels were significantly higher in subgroup C2 than in subgroup C1 after vitamin E administration (P < 0.05). In addition, CD47 levels were significantly higher in subgroup C3 than in subgroups C1 and C2 (both P < 0.05, Figure 5).

Comparison of CD47 levels before and after administration in Group C.
CD55 levels did not differ among subgroups C1, C2, and C3 before vitamin E administration. After vitamin E administration, CD55 levels were lower in subgroup C2 than in subgroup C1 (P < 0.05), and its levels were lower in subgroup C3 than in subgroups C1 and C2 (both P < 0.05, Figure 6).

Comparison of CD55 levels before and after administration in Group C.
Discussion
In the US, more than half of elderly patients develop SAP, which carries high treatment costs. 8 Neutrophils (PMNs) play an important role in defenses against pulmonary infection. Many laboratory and clinical medicine studies have reported that neutrophils play an important role in the control of early pulmonary infection. Furthermore, if poorly controlled, PMN infiltration into the lungs may cause tissue injury and increased mortality. 9
Elderly patients are at high risk of insufficient intake of vitamin E, an antioxidant with potent immunoregulatory functions.10,11 In a mouse model, vitamin E supplementation reversed age-related susceptibility to pneumococcal infection by regulating the lung recruitment of PMNs.10,12 The aforementioned process results in a greatly reduced bacterial lung burden and increased infection control. 9 Vitamin E deficiency may impair humoral and cellular immune responses. 13 Eight forms of vitamin E exist. 14 Vitamin E in elderly patients can enhance adaptive immune responses.11,13,14
CD47 plays an important role in the extracellular matrix with the αVβ3 complex structure, which is involved in neutrophil activation. CD47 deficiency affects the normal activation of neutrophils via an interaction with αVβ3 in the extracellular matrix. 15 CD47, as an adhesion molecule, plays an important role in the migration of neutrophils to sites of damage. 16 A recent study demonstrated that the anti-CD47 monoclonal antibody C5/D5 specifically inhibited neutrophil crossing of the collagen filtration layer, endothelial monolayer, and intestinal epithelium in a concentration-dependent manner without inhibiting β2 integrin-mediated adhesion in vitro. 17 In vivo experiments revealed inhibited neutrophil recruitment, prolonged inflammatory response times, and a weakened role for the integrin oxidative stress reaction in CD47-knockout mice, resulting in increased bacterial lethality after infection. 18 We can infer that CD47 plays an important role in mediating phagocytosis; however, its role in apoptotic PMN phagocytosis is not fully understood. 19
According to the results of the current study, CD47 levels were better in vitamin E-treated subgroups than in control subgroups matched for age, sex, and history of disease. CD47 levels were higher in the high-dose vitamin E subgroups than in the low-dose vitamin E subgroups. The length of hospitalization was higher in the high-dose vitamin E subgroups than in the low-dose vitamin E subgroups. These results demonstrated that high CD47 expression is of great significance for the pulmonary chemotaxis of neutrophils. In addition, the results of prior animal experiments were similar. The recommended dosage of vitamin E for the Chinese population is 50 to 100 mg/day. This dosage is considered safe.
Inhibition of neutrophil apoptosis is of great significance for the treatment of pulmonary infection. It has been reported that CD55 at low levels induces PMN apoptosis in vitro. 20 Our results indicated that CD55 levels were higher in patients who received vitamin E than in untreated patients, and its levels were higher in the high-dose subgroups than in the low-dose subgroups. The length of hospitalization was significantly shorter in patients who received vitamin E than in untreated patients.
Vitamin E can enhance the adaptive immune response in elderly patients. 11 Recent research suggested that vitamin E enhanced the resistance of aged mice to bacterial pneumonia by modulating the innate immune response. 12 This report had potential clinical implications based on the findings that infection could be controlled in elderly mice through specific nutritional support. 12 The incorporation of vitamin E into the cell membrane has been described to alter the localization and function of several molecules involved in signaling cascades.15,21 In fact, recent studies found that in the respiratory epithelium and PMNs, vitamin E affects the expression of cell-surface molecules with key roles in regulating PMN migration. Notably, vitamin E treatment caused significant changes in CD18, CD47, and CD55 expression on the surface of PMNs. 19
Furthermore, the critical dependency on two surface adhesion molecules (i.e., CD18 and CD47) was unique to PMN transepithelial migration induced via gradients of hepoxilin A3 (HXA3). 22 Vitamin E diminished the PMN surface expression of CD18 and CD47, which has notably been demonstrated to promote HXA3-mediated PMN migration across the epithelium. 22
The surface expression of two complement regulatory proteins, namely CD59, an inhibitor of the membrane attack complex, and CD55, an inhibitor of the C3/C5 convertase, was demonstrated on PMNs aged in culture. These two proteins attach to the membrane through glycosylphosphatidylinositol (GPI) anchors, and their loss is closely related to the appearance of apoptotic morphology. 23 Vitamin E may inhibit PMN apoptosis by increasing the binding stability between CD55 and GPI. 24
Regarding the study limitations, this clinical study included only patients with mild SAP, and its sample size was small. This study also examined only one aspect of SAP, but several factors are involved in pulmonary infection. Future research is needed to explore the reasonable dosage and timing of vitamin E application in the elderly Chinese population.
Based on this study's results, we believe that across different nutritional statuses, patients who consume vitamin E experience beneficial results.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060520949657 - Supplemental material for Effect of vitamin E on stroke-associated pneumonia
Supplemental material, sj-pdf-1-imr-10.1177_0300060520949657 for Effect of vitamin E on stroke-associated pneumonia by Hongwei Shen and Bingyan Zhan in Journal of International Medical Research
Footnotes
Availability of data and materials
Anonymized data from the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The paper was supported by the Dean’s fund of the Municipal Hospital.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.