
Abstract
Objective
Self-management is beneficial for improving health outcomes in adults with type 1 diabetes. However, there are no validated instruments to assess self-management in Chinese adults with type 1 diabetes. The aim of this study was to develop and validate the Self-Management of Type 1 Diabetes for Chinese Adults (SMOD-CA) scale.
Methods
Qualitative and quantitative methods were used to develop the SMOD-CA.
We conducted a literature review and semi-structured interviews to generate an initial item pool. An expert panel examined the content validity. We conducted a cross-sectional survey to evaluate scale reliability and validity. A total of 243 participants were recruited. Exploratory factor analyses were used to test the construct validity, and internal consistency and test-retest reliability were assessed.
Results
The expert panel determined that the SMOD-CA content validity index was satisfactory. The final 30-item scale consisted of four factors explaining 49.50% of the total variance in the data. Cronbach’s α was 0.901 for the total scale and 0.911 for test–retest reliability.
Conclusions
The SMOD-CA demonstrated good reliability and validity. The scale is a credible and effective instrument that can be used by social workers and health care professionals to assess self-management in Chinese adults with type 1 diabetes.
Introduction
Type 1 diabetes mellitus (T1DM) is a chronic metabolic disease, characterized by hyperglycemia, which develops when the pancreas stops producing insulin owing to autoimmune destruction of β cells. 1 In many countries and regions, the morbidity of diabetes mellitus (DM) is increasing owing to acceleration of urbanization and changes in people's lifestyles. 2 According to data of the International Diabetes Federation, 451 million adults had DM worldwide in 2017, and it is estimated that this number will increase to 693 million by 2045. 3 Adults with T1DM make up less than 5% of the overall population with diabetes, 4 but the prevalence of T1DM is increasing. 5 Living with T1DM requires constant attention. 5 If not managed optimally, T1DM can lead to an increased risk of cardiovascular disease, microvascular complications, 6 and premature death. 7 , 8 By 2017, approximately 5 million adults died from DM worldwide. According to statistics, the medical expenditures of adult patients with DM worldwide reached $850 billion in 2017; by 2045, this figure will be $958 billion. The prevalence and mortality rate of DM as well as the increase in medical expenditures have led to a major global public health burden. 9 , 10
The incidence of T1DM is relatively low in China, but the actual number of patients with T1DM is high owing to the large population of China. 11 Studies have found that patients with T1DM in China have particular sociodemographic characteristics.12–16 Additionally, these patients have many challenges: the age of onset is relatively old, patients’ body condition is thin and weak, blood glucose monitoring frequency is extremely low, insulin treatment schemes are not standardized, blood glucose control does not meet the required targets, and various acute and chronic complications frequently occur.
T1DM is a patient-managed disease that requires consistent patient engagement and educated decision making in real time to manage the disease effectively. Diabetes self-management is essential to the successful management of chronic health conditions and preventing complications from poorly managed diabetes, such as cardiovascular disease and diabetic retinopathy. 17 Studies have shown that effective self-management can improve patients' self-efficacy, emotional well-being, and physical condition and functioning, as well as reducing medical expenses to different degrees. Keeping blood sugar at normal levels in patients with diabetes can reduce the occurrence of complications such as cardiovascular disease, diabetic nephropathy, and sexual dysfunction.18–25
According to relevant studies, four instruments are used to evaluate self-management in adults with T1DM, including the Summary of Diabetes Self-Care Activities (SDSCA), Self-Care Inventory-Revised (SCI-R), Confidence in Diabetes Self-Care (CIDS), and the Diabetes Self-Management Questionnaire (DSMQ).26–28 The SDSCA does not contain items about collaboration and goals in the disease management process, and the SCI-R mainly focuses on the evaluation of patients' self-management behavior. The CIDS lacks an evaluation of patients' management goals, and the DSMQ is only applicable to patients with a long duration and severity of disease, which is not representative of most patients with diabetes.
Treatment of T1DM must incorporate long-term self-management by patients to slow or prevent the occurrence of acute and chronic complications. However, there are no dedicated scales for evaluating self-management of T1DM in adults. We developed the Self-Management of Type 1 Diabetes in Chinese Adults (SMOD-CA) scale to expand the scope of self-management assessment and provide researchers with the option of a self-reporting tool. Any tool must ensure scientifically based evaluation of self-management, for clinicians to evaluate and promote self-management in adults with T1DM. Researchers will also benefit from more comprehensive self-management measures when evaluating the effectiveness of interventions to improve diabetes management. The purpose of the present study was to develop and evaluate a scale for the assessment of self-management in adults with T1DM in China.
Methods
Study design
Qualitative and quantitative methods were used to develop the SMOD-CA. 29 , 30 Scale development comprised several phases, including item generation, content validity testing, exploratory factor analysis (EFA), and reliability testing (Figure 1).
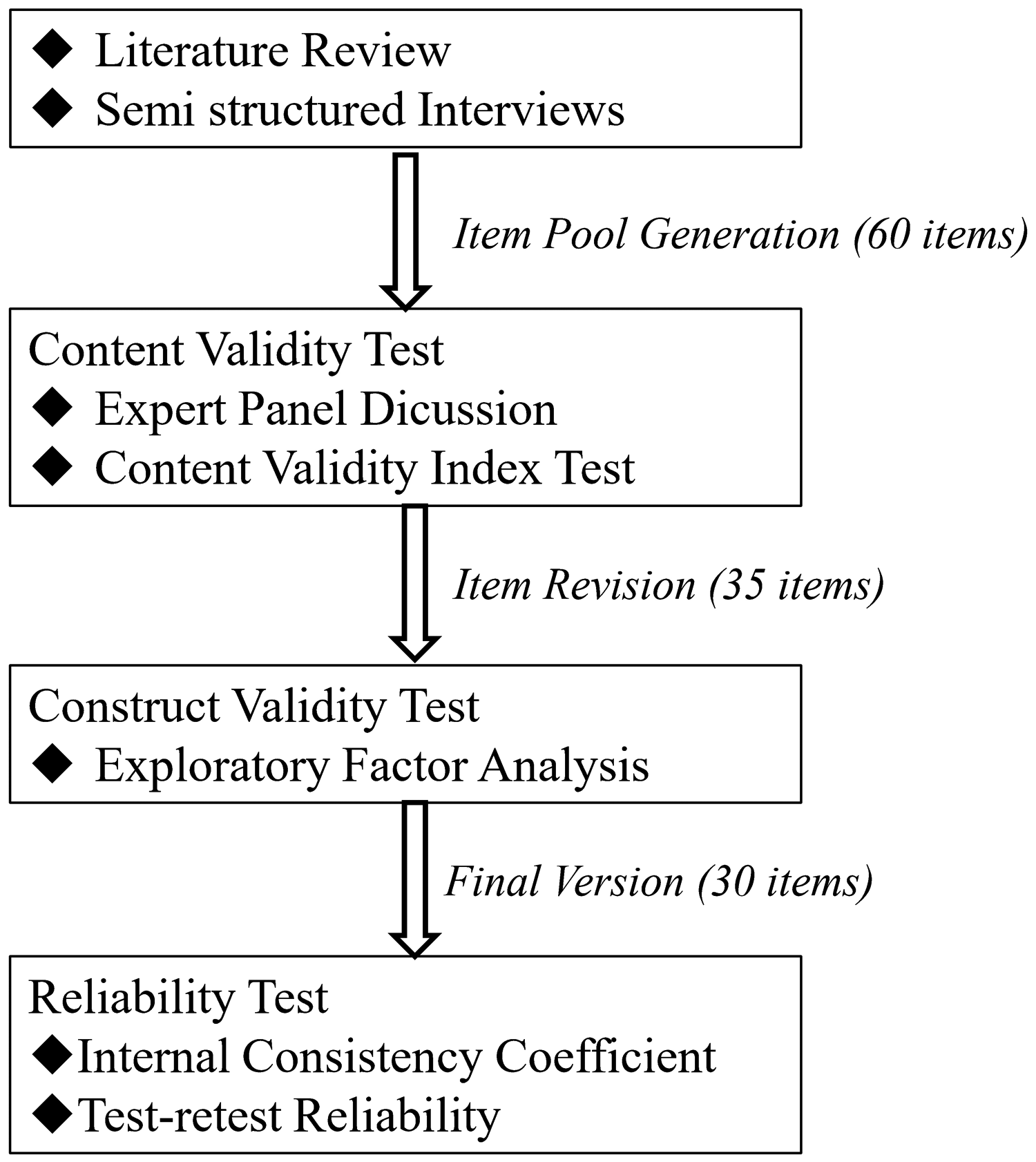
Flow chart of scale development.
Item generation
The content of the scale was informed using qualitative data of self-management from 16 adults with T1DM. In the qualitative descriptive study, semi-structured interviews were conducted among the 16 adults. Participants ranged in age from 18 to 48 years, and they had been diagnosed with diabetes for 1 to 19 years. One author drafted an initial 36-item pool based on participant quotes from interview transcripts, representing all key themes in the data. The key themes included daily performance of self-management, disease management and collaboration, coping with disease-related problems, and goals of self-management. The items were constructed as statements with a five-point Likert response scale (never to always). An additional 24 items were drafted based on items used in existing self-management scales such as Self-Management of Type 1 Diabetes in Adolescents (SMOD-A), 31 SDSCA, SCI-R, CIDS, and DSMQ.26–28 Finally, a 60-item pool was established. The overall score is obtained by summing the scores of all items. Higher scores indicate better diabetes self-management.
Validity testing
In the second phase, the 60 items were reviewed by an expert panel of 10 diabetes professionals and educators. The items were evaluated individually and as a set by the expert panel for clarity and relevance. From the expert panel discussion, the phrasing of each item in the item pool was further revised to make the item more concise and easily understandable. For items with semantic similarity, only the item that was most concise and easier to understand was retained, to avoid redundancy. As a result, 22 items were deleted. This process resulted in a 38-item instrument. Relevance was assessed using a content validity index (CVI) based on a four-point scale: 1 = not relevant/representative; 2 = needs major revision; 3 = needs minor revision; 4 = relevant/representative. The CVI was calculated as the percentage of total items rated by experts as either 3 or 4; a CVI above 0.8 was considered to be valid. 32 For this study, 10 experts returned their rating scales. Three items with CVIs ranging from 0.52 to 0.69 were deleted. This resulted in a revised scale with 35 items. The scale-level CVI was 0.904, indicating universal agreement. The dimensionality of the scale was estimated using EFA.
Reliability testing
Reliability refers to the extent to which a scale consistently and stably measures the attributes it was intended to measure. 33 The internal consistency of the SMOD-CA scale was estimated by computing Cronbach’s α coefficient. According to Nunnally’s research, the estimates of internal consistency should be well above 0.70 for newly developed research tools. 34 The test–retest reliability of the scale was calculated in 20 individuals who repeated the SMOD-CA scale 2 weeks after the first administration.
Participants
We conducted a cross-sectional study using the developed scale at a tertiary hospital in the Hunan region of China between July 2017 and February 2018. We followed the recommendation to enroll 50 participants for each domain (estimated sample = 200). 35 , 36 Further, taking into account invalid questionnaires, we increased the sample size by 20% to n ≥ 240. To ensure construct validity and reliability, we tried to enroll as many participants as possible on the basis of the sample size. The inclusion criteria were (a) having a diagnosis of T1DM for at least 6 months, according to standard criteria; (b) age 18 years or older, and (c) able to complete the questionnaire independently. 37 Patients with severe cognitive impairment and severe psychiatric diseases were excluded.
Data collection
Two data collectors were trained for this study. Data collection was conducted using self-reported questionnaires administered face-to-face with participants. For reliable data collection, the data collectors met with patients to explain the purpose and procedures of this study. All participants completed a form containing sociodemographic information and the SMOD-CA scale.
(1) Demographic and medical characteristics
Demographic variables on the self-report questionnaire included age, sex, education level, marital status, and average monthly income. Medical variables were collected, including duration of T1DM and glycated hemoglobin (HbA1c) levels.
(2) The SMOD-CA scale consisted of 35 items. Participants’ responses to the items were on a five-point scale ranging from 0 to 4.
Ethical considerations
This study was approved by the Institutional Research Boards of Behavioral and Nursing Research in the School of Nursing of Central South University, Changsha City, Hunan Province (IRB NO. 2017030, IRB Approval Date: June 1, 2017). All eligible patients provided their written informed consent prior to participation in this study.
Statistical analysis
We used IBM SPSS Version 24 for all the analyses (IBM Corp., Armonk, NY, USA). Descriptive statistics were used for all study measures and demographic variables. Continuous variables are presented as mean ± standard deviation, and categorical variables are presented as number and frequency (%).
The construct validity of the SMOD-CA was evaluated using EFA, analyzed via the principal component extraction method with varimax rotation. As suggested by various experts, multiple analyses were required to select the solution yielding factors that had adequate internal consistency and were deemed most meaningful by the research team. 38 , 39 The number of factors to be extracted was determined based on a scree plot. The criteria to determine the number of factors to retain were: (a) eigenvalues greater than 1.0 and (b) a factor loading cut-off of 0.40. 40 Pearson’s correlation was used to analyze the relationships between the items and total scale. Cronbach’s α was used to determine the internal consistency of the scale, and test–retest reliability was performed to examine the consistency and reliability of the scale.
Results
Demographic and clinical characteristics
In all, 260 adults with T1DM were eligible for the study, and 243 (123 men and 120 women) of them responded. Thirteen patients declined to participate owing to a lack of interest (n = 5) and not having the time (n = 8). Four participants were excluded as they failed to complete the questionnaire packet. Most participants completed the packet of instruments in 20 minutes or less.
The mean age of the 243 participants was 29.64 years (SD = 9.66). The mean duration of diabetes was 6.34 years (SD = 6.45). The mean HbA1c was 7.92% (SD = 1.98). Other demographic and clinical characteristics are shown in Table 1.
Demographic and clinical characteristics of study participants (n = 243).
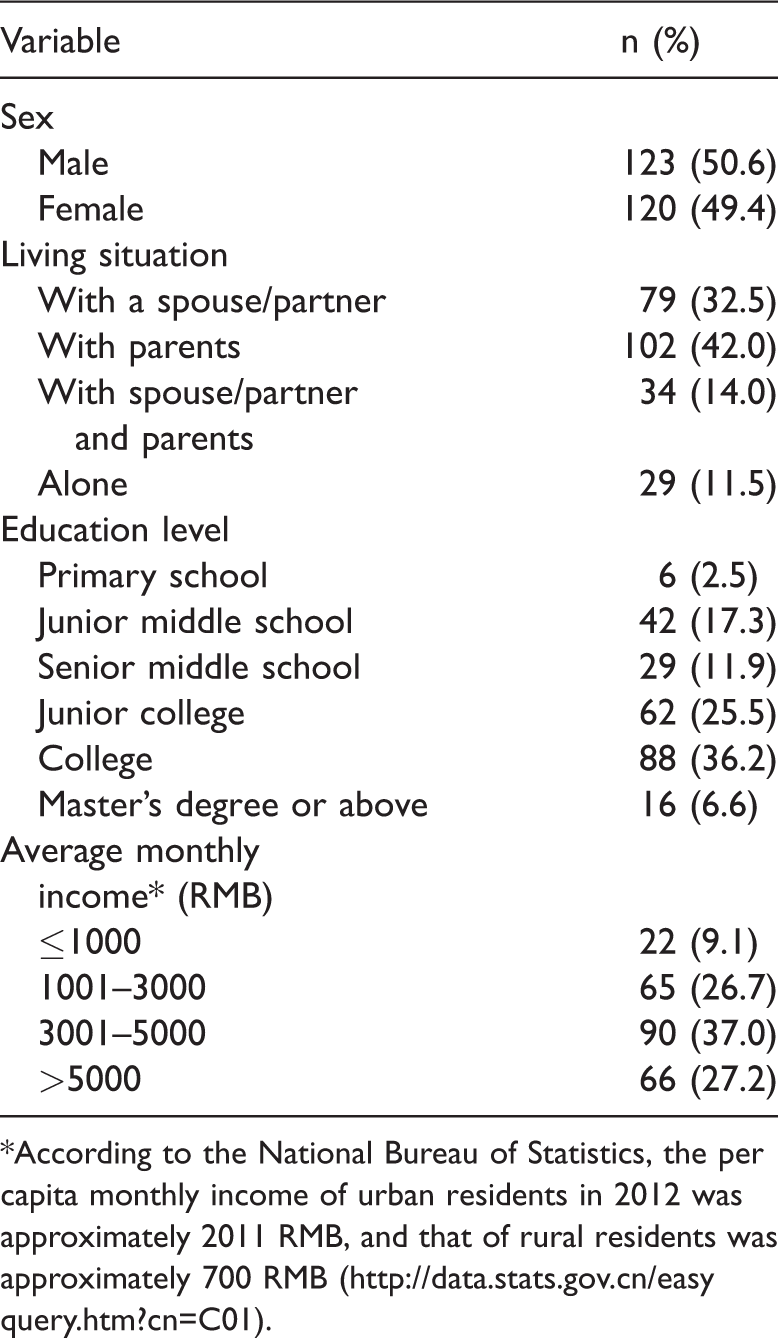
*According to the National Bureau of Statistics, the per capita monthly income of urban residents in 2012 was approximately 2011 RMB, and that of rural residents was approximately 700 RMB (http://data.stats.gov.cn/easyquery.htm?cn=C01).
Construct validity testing
Bartlett’s test of sphericity was significant (χ2 = 3,923.757, df = 595, P < 0.01), indicating that the factor analysis was appropriate for the data. 40 The Kaiser–Meyer–Olkin (KMO) measure of satisfactory sample adequacy is 0.80 and above. 41 For the sample in this study, the KMO measure of sampling adequacy was 0.817, indicating that the sample size was suitable for factor analysis. We performed varimax rotation principal component analysis to determine the underlying factor structure of the 35-item SMOD-CA scale and whether any items should be removed.
The initial principal components analysis yielded 10 factors with eigenvalues >1. All 10 components accounted for 66.29% of the total variance. Upon examining the scree plot (Figure 2), a clear “elbow” was observed for six factors, which directed the subsequent analysis. After three rounds of exploratory factor analysis, because the loadings on the factors were high (>0.40), a solution with four factors was determined to be the best (Table 2). Among the 35 items in the factor analysis, 30 items comprised the four factors and accounted for 49.50% of the total variance. The factors within the instrument were named according to the underlying construct related to the items. These factors were designated as Daily Performance (6 items), Disease Management and Collaboration (11 items), Coping with Disease-Related Problems (7 items), and Goals of Disease Management (6 items).

Scree plot of principal components analysis of the Self-Management of Type 1 Diabetes for Chinese Adults (SMOD-CA) scale.
Variance explained by the 30-Item SMOD-CA scale.

SMOD-CA, Self-Management of Type 1 Diabetes for Chinese Adults.
The construct validity of the 30-item SMOD-CA scale was further evaluated using correlation analysis of the scores among the items, domains, and total scale. The item-total correlation coefficients of the domains varied from 0.436 to 0.862. As shown in Table 2, the interdomain correlation coefficients varied between 0.334 and 0.558, and the domain-total correlation coefficients varied between 0.685 and 0.846, confirming the construct validity of the scale. The correlation between HbA1c and the total score was statistically significant, and the correlation coefficient was −0.416.
Reliability
Cronbach’s α coefficient was 0.901 for the total scale (30 items) in the final version of the SMOD-CA, ranging from 0.773 to 0.857 for the four domains that were considered acceptable. 42 For the item analysis, Table 3 lists the reliability estimates, means, and standard deviations of the domains. Correlations among the domains and the total scale are displayed in Table 4. The test–retest correlation for the total scale was 0.911 (P < 0.01); each dimension ranged from 0.816 to 0.925 in the 2-week interval (n = 20). Thus, the results demonstrated that the total scale and its domains were stable over time.
SMOD-CA domain reliability estimates, means, and standard deviations.

*P < 0.01.
SMOD-CA, Self-Management of Type 1 Diabetes for Chinese Adults.
Correlation among domains and the total SMOC-CA (n = 243).

**P was significantly correlated at the level of 0.01 (two-sided).
Discussion
T1DM is now well recognized as a disease that places a heavy burden on patients and health care systems. 43 Although numerous studies have demonstrated the benefits of self-management interventions for patients with T1DM,44–47 few effective tools are available to assess the self-management status of adult patients with T1DM. The objective of this study was to develop and validate a new self-management scale of T1DM for Chinese adults (SMOD-CA). This scale can contribute to improving self-management interventions for adults with T1DM. Health care providers can gain a better understanding of self-management behaviors in these patients, to develop more effective interventions.
T1DM self-management requires complex tasks that must be integrated into the patient’s daily life. 48 Patients with T1DM must manage their blood glucose, insulin dose, diet, physical activity, complications, and physiological and psychosocial issues, among others. The item pool was based on an extensive literature review of T1DM self-management scales and semi-structured interviews. We also investigated the psychometric characteristics of the SMOD-CA scale.
Psychometric evaluation of the SMOD-CA
Content validity refers to the extent to which a specific set of items reflects a content domain, reflecting the adequacy of item sampling. 33 The expert panel method is the most commonly used, which is a convincing approach for measuring content validity. 49 First, we defined the scope of the contents to be measured. Then, panel experts were asked to evaluate the correlation between the items and domains of interest, to maximize item appropriateness. 33 A CVI value above 0.80 indicates adequate content validity, although some scholars set 0.75 as the acceptable limit. In this study, the acceptable level of the CVI value was set to 0.80.49–51 After generating the item pool through a literature review and semi-structured interviews, the initial version of the scale was developed in an evaluation of the item pool by an expert panel (n = 10) consisting of diabetes professionals and educators. The overall CVI value in the initial version of the scale was 0.904, suggesting that the scale has good content validity.
Exploratory factor analysis is a useful analytic method to empirically determine how many constructs or latent variables or factors underlie a set of items, in a way that reliability coefficients cannot. 42 After EFA, four common factors were extracted from the 30 items in the revised version, and the cumulative contribution rate was 49.50%. The correlation coefficients between the scores for each factor and the total scale score ranged from 0.658 to 0.846 and were greater than the correlation coefficients for each individual factor (0.334–0.558), indicating that the scale has good construct validity. The results of the factor analysis for the revised version of the scale showed that self-management in adults with T1DM included four aspects, namely, Daily Performance, Disease Management and Collaboration, Coping with Disease-Related Problems, and Goals of Disease Management. The HbA1c is a widely used measure of T1DM self-management. The SMOD-CA total score was negatively correlated with HbA1c, with a correlation coefficient of −0.416, indicating good criterion validity of the SMOD-CA scale.
In this study, Cronbach’s α coefficient and the test–retest reliability of the scale ranged from 0.773 to 0.925, indicating that the scale has good reliability.
Study limitations
There are several limitations in this study. First, the SMOD-CA was developed and validated only in the Hunan region of China. Further studies are needed to evaluate applicability of the scale for other ethnicities and countries. Another possible limitation is social desirability bias, which tends to exaggerate good behaviors when answering survey questions. This bias may lead to overestimation of patients’ ability to manage their diabetes.
Our data highlight that the SMOD-CA is a reliable, valid, and sensitive tool for evaluating the self-management status of adults with T1DM. The scale provides clinicians and researchers with a tool to assess self-management in adults with T1DM. This study demonstrated that self-management, as measured by the SMOD-CA, is a multidimensional construct. This scale may be a useful complement for assessing how adults with T1DM are managing their disease and can serve as an important tool to evaluate and improve self-management among adults with T1DM in China.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060520947588 - Supplemental material for Development and validation of a self-management scale of type 1 diabetes for Chinese adults
Supplemental material, sj-pdf-1-imr-10.1177_0300060520947588 for Development and validation of a self-management scale of type 1 diabetes for Chinese adults by Song Zhu, Fang Liu, Jina Li, Yuzhu Guan, Meng Meng, Xia Li, Zhiguang Zhou, Rong Xu and Lezhi Li in Journal of International Medical Research
Footnotes
Acknowledgements
The authors thank all the participants who contributed to the study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by National Key Research and Development of China (grant number 2017YFC1309604) and the Clinical Nursing Research Fund Project of the Second Xiangya Hospital (grant number 2017-YHL-03).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.