
Abstract
Gallbladder cancer is a relatively rare malignancy that is generally diagnosed at an advanced stage. Palliative chemotherapy, radiotherapy, or immunotherapy may be appropriate options for advanced gallbladder cancer, instead of radical surgery. In the present report, we describe an extremely unusual case of a 59-year-old man diagnosed with advanced primary squamous cell carcinoma of the gallbladder, according to imagological and pathological examinations. The symptoms of the patient were atypical. Preliminary data indicated that not only the systemic inflammatory biomarkers neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and lymphocyte-to-monocyte ratio but also jaundice might be correlated with the prognosis. Although the patient was treated with the best supportive care, overall survival time was only about 2 months. Advanced primary squamous cell carcinoma of gallbladder is incurable and highly lethal.
Keywords
Introduction
Gallbladder cancer, a relatively rare malignancy in China, has multiple histopathologic subtypes. 1 Primary squamous cell carcinoma of gallbladder (SCCG) accounts for only 2% to 3% of gallbladder cancers and is the rarest histopathologic subtype of gallbladder cancer. 2 Because of its concealed symptoms and aggressive biological behavior, most patients with SCCG are diagnosed at an advanced stage and have a poor prognosis. 1 , 2 Some studies suggest that systemic inflammatory biomarkers3–6 or jaundice 7 may have predictive efficacy for the prognosis of patients with gallbladder cancer. Here, we report an extremely unusual case of advanced SCCG.
Case report
A 59-year-old man visited our hospital on 6 May 2019, with a 10-day history of moderate epigastric pain radiating to the back, fever, and vomiting. No jaundice, decreased appetite, or weight loss was noted. He denied a history of cholelithiasis. Several years before, he had undergone a splenectomy because of traffic accident injuries. His body mass index (BMI) was 23.7, with an Eastern Cooperative Oncology Group (ECOG) performance score of 2.
A tentative diagnosis of acute cholecystitis and gallbladder neoplasm was made based on clinical symptoms; physical examination; abnormal increases of leukocytes, neutrophils, and C-reactive protein level; and irregular thickening of gallbladder wall (18 mm) observed by abdominal ultrasonography examination. Liver function tests were normal. Antibiotic therapy was administered immediately but the efficacy was not satisfactory. A computed tomography (CT) scan of the chest, abdomen, and pelvis was conducted, which revealed a large gallbladder mass measuring 50 × 40 mm with solid and cystic components, suggesting gallbladder malignancy. The mass had infiltrated the liver (Figure 1), with multiple liver metastases, several enlarged hepatic hilar region lymph nodes (with the largest node measuring 30 × 22 mm), and retroperitoneal lymph nodes (Figure 2). The pancreas, in contrast, appeared normal, with no biliary obstruction or strictures observed. Tumor tissue was obtained by percutaneous needle biopsy, guided by B-ultrasound. Histopathological examination revealed poorly differentiated pure squamous cell carcinoma. Immunohistochemical results were as follows: Heppar-1 (±), glypican-3 (−), Ki-67 (60%+), cytokeratin (CK)19 (+), CK7 (+), P40 (+), and P63 (+) (Figure 3). Endoscopy was performed and no tumors of the esophagus, stomach, and duodenum were found. The patient was diagnosed with pure poorly differentiated squamous cell carcinoma of gallbladder, invading all layers of the gallbladder with infiltration of the liver, accompanied by multiple liver and lymph node metastases, staged IVB: cT3N2M1, G3, according to the American Joint Committee on Cancer (AJCC) TNM Staging for Gallbladder Carcinoma (8th ed., 2017). Unfortunately, the patient could not tolerate palliative chemotherapy, radiotherapy, or immunotherapy due to the poor performance status (BMI = 20.3, ECOG = 3). Thus, the best supportive care was given. One week later, the epigastric pain worsened and could not be alleviated without morphine. One month later, the patient had decreased appetite, weight loss, jaundice, yellow urine, and pale stools. The patient’s alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase, direct bilirubin, total bilirubin (Figure 4), and CA199 levels began to increase continuously and rapidly and he experienced osteodynia. Bone scans showed multiple nuclear aggregations in the sternum and several vertebrae. The patient refused an invasive bone biopsy so the pathology could not be assessed. A CT scan and endoscopy examination excluded other primary tumor sites, such as lung or prostate.

Abdominal computed tomography scan examination revealed a large gallbladder mass measuring 50 × 40 mm with solid and cystic components and infiltrating the liver.

Abdominal computed tomography scan examination showed several enlarged hepatic hilar lymph nodes (with the largest node measuring 30 × 22 mm) and retroperitoneal lymph nodes. The pancreas appeared normal and no biliary obstruction or stricture was observed.
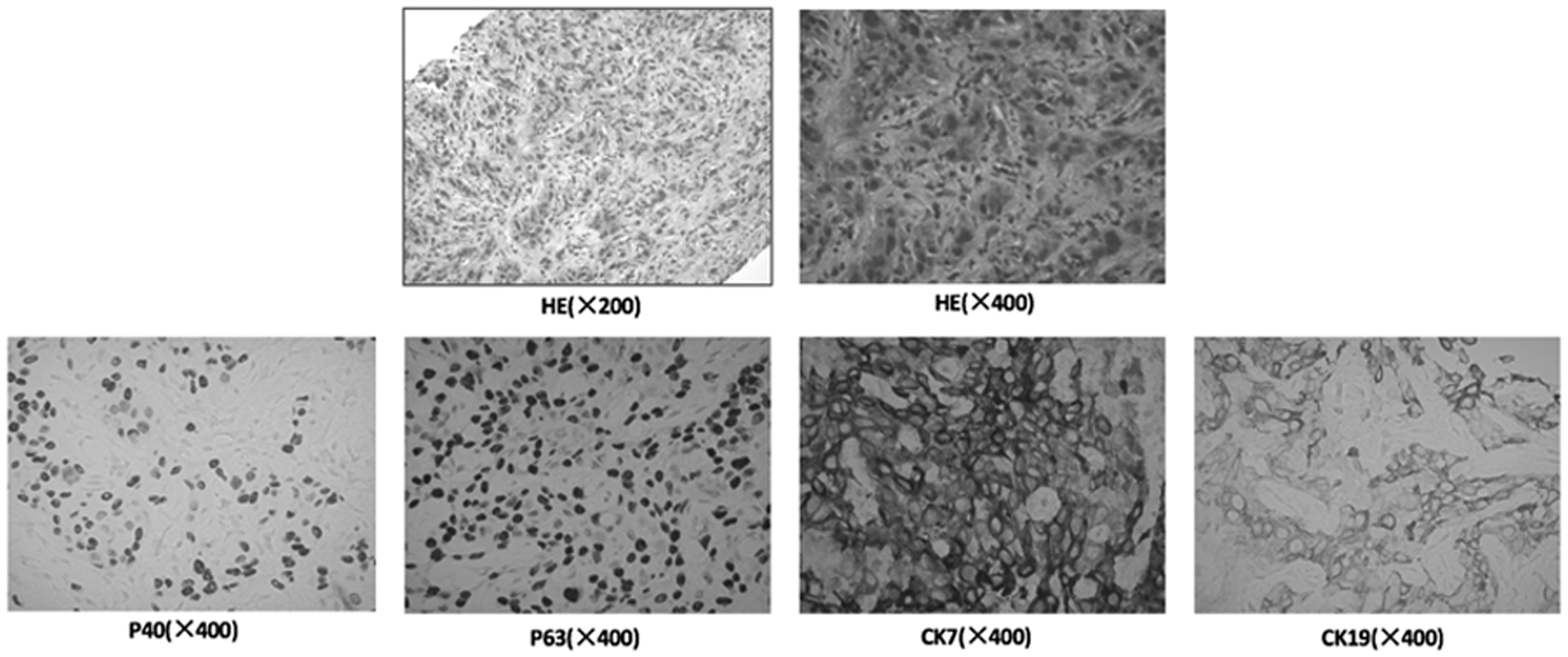
Histopathological examination of the tissue biopsy revealed poorly differentiated pure squamous cell carcinoma. Immunohistochemical results showed strongly positive expression of cytokeratin 19 (CK19), cytokeratin 7 (CK7), P40, and P63.

Serum bilirubin levels increased continuously and rapidly in the last month of the patient’s life.
Another B-ultrasound examination followed, which showed that the metastatic liver masses, hepatic hilar region lymph nodes, and retroperitoneal lymph nodes had increased in size (the largest node measuring 42 × 31 mm), indicating that the cancer had progressed rapidly. The patient’s performance status worsened further (BMI = 19.6, ECOG = 4). Systemic inflammatory biomarkers, such as NLR, PLR, and LMR, were investigated, and results showed that all of these biomarkers were related with poor prognosis (Figure 5, Table 1). Despite the best supportive care and anti-infective therapy, the patient died of biliary obstruction and related infection, which had led to multiple organ failure, on 30 June 2019 (an overall survival time of about 2 months).

According to the predictive nomogram made by Deng et al., 11 NLR and PLR values higher than the cut-off values (2.61 for NLR; 145.33 for PLR) or LMR lower than the cut-off value (2.66) indicate a poor prognosis for gallbladder cancer.
Patient’s blood data used to derive the systemic inflammatory biomarkers NLR, PLR, and LMR.

NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio.
Discussion
Gallbladder cancer has an extremely low morbidity but a high mortality. SCCG has the poorest prognosis of all histologic subtypes, with a median survival time of 7 months and a 5-year survival rate less than 12%. 8 The highly malignant biological behavior of squamous cell carcinoma is characterized by rapid proliferation and early dissemination to local and distant sites, including the regional lymph nodes, distant hepatic parenchyma, and peritoneal surfaces. 9
The therapeutic strategy of SCCG may be complex but essentially relies on surgical resection. If SCCG is identified early, surgical resection is potentially curative and can improve the prognosis. 10 Unfortunately, only a small population of patients with localized disease benefit from surgical resection. Most patients with gallbladder carcinoma are diagnosed at an advanced stage and do not have the opportunity to undergo the radical surgical operation. Palliative treatments such as chemotherapy, radiotherapy, immunotherapy (such as pembrolizumab only for MSI-H gallbladder cancer), and best supportive care are the appropriate recommendations. Even so, SCCG remains highly lethal because of its rapid progression and short overall survival time. In the current report, a patient with primary SCCG was diagnosed at an advanced stage (cT3N2M1, cIV stage) and surgery was not appropriate. Furthermore, chemotherapy, radiotherapy, or immunotherapy were not administered because of the patient’s abnormal liver function and poor performance status. Ultimately, the patient was treated only with supportive care. Along with continuous rapid elevations in levels of transaminases and bilirubin, the rapid growth of the metastatic liver masses and lymph nodes indicated that the cancer was progressing rapidly.
Definitive prognostic factors in SCCG have not yet been reported. It is currently recognized that the systemic inflammatory microenvironment plays a significant role in carcinogenesis, tumor proliferation, invasion, and metastasis.3–5 A recent study suggested that prognosis of patients with malignancy is correlated not only with tumor-related factors but also with the host response to systemic inflammation. 6 A study revealed that preoperative NLR, PLR, and LMR, which are significant and powerful prognostic indicators for patients undergoing radical gallbladder cancer surgery, are significantly related to overall survival. 11 We investigated the same systemic inflammatory biomarkers (NLR, PLR, and LMR) in our patient and showed that these biomarkers were correlated with prognosis, consistent with previous findings. Thus, systemic inflammatory biomarkers may have predictive efficacy for prognosis in patients with advanced-stage gallbladder cancer.
As an indicator of advanced malignancy, jaundice predicts advanced disease and early mortality in patients with gallbladder cancer. Jaundice is not an independent predictor of survival, but it is highly correlated with advanced-stage disease, positive surgical margins, and a significantly lower median disease-specific survival compared with patients without jaundice (6 vs. 16 months). 7 The incidence of bone metastasis of gallbladder carcinoma is very low and usually associated with advanced disease. Singh et al. 12 reported a case in which bone was the only site of distant metastasis of a gallbladder carcinoma, which precluded radical surgery. The patient in this report developed jaundice eventually, along with multiple bone metastases and enlarged gallbladder mass and hepatic hilar region lymph nodes. He died shortly thereafter of biliary obstruction and related infection, which led to multiple organ failure, with an overall survival time of about 2 months.
Conclusion
In this report, we described the case of a 59-year-old man with acute-onset epigastric pain radiating to the back. According to imaging tests, tissue biopsy, and pathological examination, advanced-stage primary poorly differentiated squamous cell gallbladder carcinoma was diagnosed, although the clinical symptoms were atypical. The systemic inflammatory biomarkers NLR, PLR, and LMR and jaundice have potential predictive efficacy for prognosis in patients with advanced gallbladder cancer but further study is needed. Advanced-stage primary SCCG is a highly lethal cancer, being incurable and having a poor prognosis, and palliative therapies may be appropriate options instead of radical surgery.
Footnotes
Author contributions
JL, YM, YW, PC, JL, and HW participated in study design, data collection, and literature search. The manuscript was written by JL. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics and consent
This study was approved by the Scientific Research Ethics Committee of the Fourth Affiliated Hospital of Nantong University [reference number: 2020(K-019)]. Written informed consent was obtained from the patient’s family for publication of this case report.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.