
Abstract
A pelvic accessory spleen is uncommon and most patients with this condition are asymptomatic. Ureteral calculus is a common disease and can cause acute abdominal pain. We report a 51‐year‐old male patient who presented at our hospital with acute right lower abdominal pain and gross hematuria. A large mass on the right side of the pelvis was detected on an ultrasound examination, as well as a calculus in the lower segment of the right ureter. Computed tomography angiography showed the presence of a long vascular pedicle with an artery originating from the splenic artery and a vein that joined with the splenic vein. Laparoscopy was carried out and it showed a solid mass covered with omentum on the right lower abdomen. The mass was then removed surgically. Histopathological examination of the resected specimens confirmed splenic tissue. We speculate that the accessory spleen and ureteral calculus caused right lower abdominal pain in our case. However, the ureteral calculus might have played a much more important role in causing acute right lower abdominal pain than the accessory spleen.
Keywords
Introduction
An accessory spleen (AS) may form owing to failure of fusion of the primordial splenic buds in the dorsal mesogastrium during the fifth week of fetal life. An AS is usually asymptomatic, and therefore, it is discovered incidentally. 1 An AS is commonly located in the splenic hilum and seldom is found in the pelvis. 2 Although AS affects 10% to 30% of the population, 3 its preoperative diagnosis remains challenging because of the rare incidence of AS located in the pelvis and the asymptomatic pattern of its manifestation. AS may resemble an abdominal or pelvic tumor, such as a metastatic lymph node, or mimic a uterine adnexal mass.4–6 However, AS can also become symptomatic owing to torsion, hemorrhage, or rupture. 7 Physicians should be aware of the presence of AS in certain situations. 8
On computed tomography angiography (CTA) scans, an AS appears as a well‐defined round mass that is homogeneous, it always differs greatly in size, and most ASs are smaller than 2 cm. 9 A feeding artery from the splenic artery displayed by CTA can be helpful for diagnosing AS. We report here a case of an AS and ureteral calculus, which caused right lower abdominal pain.
Case presentation
A 51‐year‐old male patient with sudden onset of acute right lower abdominal pain and gross hematuria was admitted to the Emergency Department on 1 June 2019. An abdominal examination showed tenderness in the right side of pelvic cavity, as well as a huge mass. The pain radiated to the right side of the lower back, along with percussion pain over the right kidney region. A routine blood test showed normal findings. Urinalysis showed that the red blood cell count was 61.50/µL. Tumor biomarkers, including α-fetoprotein, cancer antigen 125, and carcinoembryonic antigen, were within normal limits. The patient had no medical history of splenectomy or trauma.
During the first check-up, an ultrasonographic examination showed a pelvic mass of 7.0 × 6.5 cm in size and it was situated directly in front of the iliac blood vessels. The mass was grossly well circumscribed by a capsule, and the interior echo of the mass was solid and homogeneous. Color Doppler ultrasonography showed large vessels entering the mass, but tracing the origin of these vessels was difficult because of the influence of intestinal gas (Figure 1d, e). A calculus in the lower segment of the right ureter was also detected, as well as mild hydronephrosis of the right renal pelvis (pyelic separation of 18 mm, Figure 1a, b). The spleen was in the regular site and was normal in size in the left upper abdomen.

Ultrasound and color Doppler sonographic images. A calculus in the lower segment of the right ureter (a) and mild hydronephrosis of the right renal pelvis can be seen (b). At the second check-up using an ultrasonographic examination, the calculus has disappeared, but mild hydronephrosis remains (c). Cross-section of the right pelvic area showing a solid, homogeneous, pelvic mass (d). Color Doppler sonogram showing large vessels entering the mass (e).
On the third day of admission, magnetic resonance imaging (MRI) (1.5T; Signa GE Healthcare, Milwaukee, WI, USA) showed a 6.8 × 6.0-cm round mass on the right side of the pelvis (Figure 2d, e, f). On the fourth day of admission, a computed tomography (CT) scan showed a well‐defined, homogeneous, round mass in the pelvic space (Figure 2a). The mass was approximately 6.7 cm in diameter and adjacent to the right iliac blood vessels. A normal‐sized spleen was detected in the left upper abdomen. CTA clearly showed large vessels originating from the mass and ascending to the splenic hilum. CTA also showed the presence of a long vascular pedicle with an artery originating from the splenic artery and a vein that joined with the splenic vein (Figure 2b, c). On the fifth day of admission, a second check-up by ultrasonographic examination showed that the calculus had disappeared, but mild hydronephrosis remained (pyelic separation of 12 mm, Figure 1c). On the seventh day of admission, laparoscopy was carried out, and it showed a solid pediculated mass covered with omentum in the right lower abdomen (Figure 3a, b). The vascular peduncle was isolated and ligated during surgery and the mass was then removed. A definitive histological examination subsequently confirmed accessory splenic tissue (Figure 3c).On the tenth day of admission, a third ultrasonographicic examination showed no hydronephrosis. The patient had an uneventful postoperative course and was discharged 2 days later.
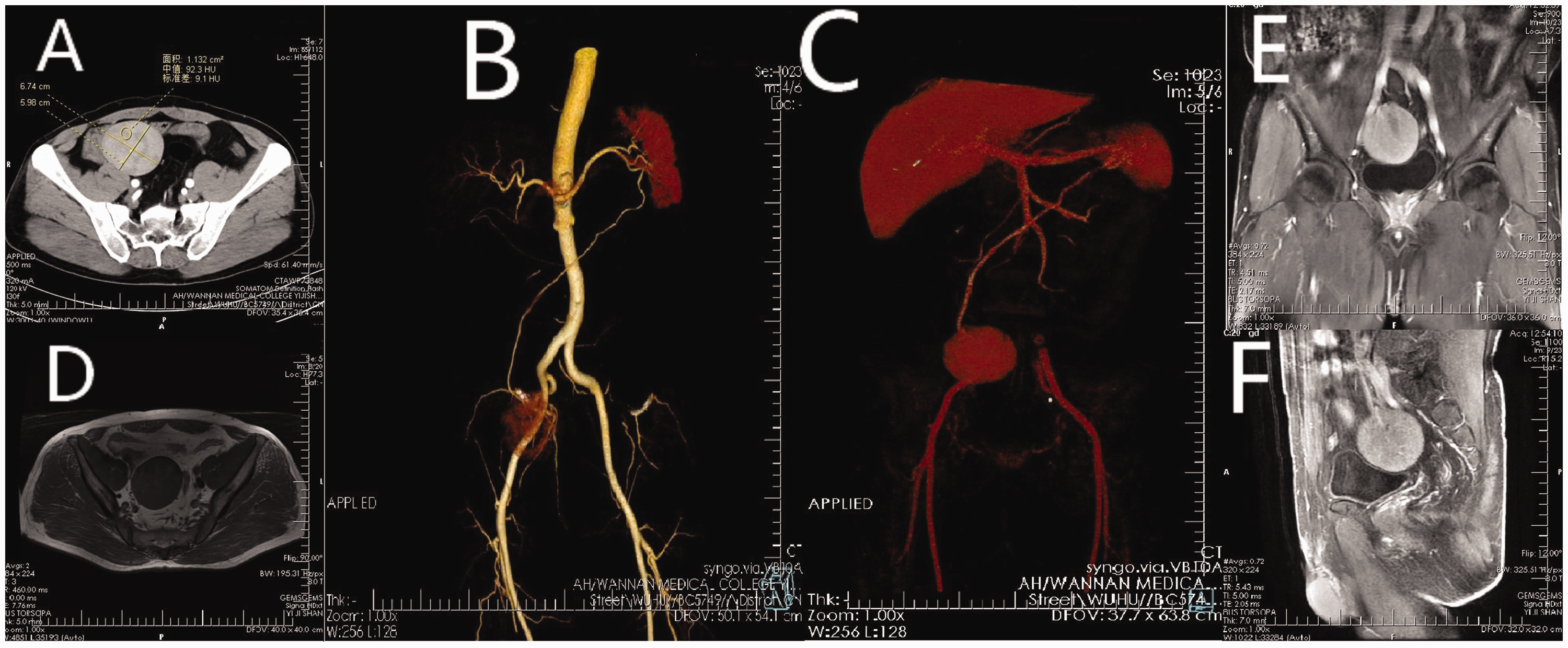
Computed tomography, magnetic resonance imaging, and computed tomography angiography images. Computed tomography and magnetic resonance imaging show a well-marginated mass in the right pelvic space (a, d, e, f). Computed tomography angiography shows the presence of a long vascular pedicle with an artery originating from the splenic artery (b) and a vein that joins with the splenic vein (c).

Inspection of the pelvis using laparoscopy shows a solid pediculated mass covered with omentum in the right lower abdomen (a). A definitive histological examination subsequently confirmed accessory splenic tissue (b, c).
The study was approved by the ethics committee of The First Affiliated Hospital of Wannan Medical College on 4 September 2019. The patient provided consent for publication of this case report. All data have been de-identified.
Discussion
AS refers to one or more ectopic splenic tissue masses with a similar structure to that of the spleen, which is in the normal position. The location of an AS widely varies and it may be found in the splenic hilum and/or the tail of the pancreas, but is rarely found in the lower abdomen and pelvis.2–4 In the clinic, AS is usually asymptomatic and is thus detected incidentally. However, AS can also cause slight discomfort or even severe acute abdominal pain due to torsion, spontaneous rupture, hemorrhage, or cyst formation, In atypical cases, preoperative diagnosis of AS is difficult. The present report describes a pelvic large AS combined with an ureteral calculus in a 51-year-old man. To the best of our knowledge, this is the first case of a patient presenting with a pelvic AS and ureteral calculus simultaneously.
In female patients, when the AS is located in the adnexal area, differential diagnoses comprise different causes of adnexal masses, including a sub-serous fibroid, ovarian tumor, enlarged lymph node, tubo-ovarian abscess, and organized hematoma. 10 , 11 The majority of cases with a pelvic AS involve female patients, while our case was an adult man; therefore, the categories of adnexal masses do not need to be taken into consideration. However, other lesions, such as gastrointestinal tumors or retroperitoneal tumors, cannot be ruled out if the nature of the mass cannot be confirmed by radiological imaging. AS is rarely symptomatic with a requirement for surgical treatment. In our patient, a second check-up using an ultrasonographic examination showed that the calculus had disappeared, but mild hydronephrosis remained. Additionally, a postoperative ultrasonographic examination showed no hydronephrosis, which indicated that the pelvic AS might have impinged upon the pelvic section of the right ureter. We speculate that the AS and ureteral calculus caused the right lower abdominal pain in the patient. However, the ureteral calculus might have played a more important role in causing acute right lower abdominal pain than the AS.
In our case, a gray‐scale and color Doppler sonographic examination provided preliminary suspicion of an accessory pelvic spleen. A CT scan with intravenous contrast was useful in delineating the vascular pedicle originating from the mass and ascending to the splenic hilum, and MRI was also used to evaluate tissue aspects of the mass. 11
Awareness of the possibility of an AS is extremely important in clinical practice. Patients with hematological disease requiring splenectomy should also undergo removal of the accessory spleen. However, the AS should be conserved where it is the only splenic tissue in the body. 12 In our case, there was no need to worry about removing the AS in the pelvis because we had preoperatively confirmed the presence of a spleen in its natural anatomical position.
In conclusion, physicians should be aware of the rare possibility of an AS in patients who present with lower abdominal or pelvic pain or a mass. Pelvic AS is diagnosed by radiological investigations, and ultimately confirmed by a histopathological examination following an open or laparoscopic operation.
Footnotes
Authors’ contributions
Concept/design: Guobing Hu; drafting of the article: Xia Zhang, Biaohu liu, and Xiangming Zhu; critical revision of the article: Guobing Hu; and approval of the article: Guobing Hu, Xia Zhang, Biaohu Liu, and Xiangming Zhu.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by funding of the “Peak” Training Program for Scientific Research of Yijishan Hospital, Wannan Medical College (KGF 2019G14).