
Abstract
Objective
This study aimed to compare the results of different graft materials in type I tympanoplasty for patients with a large perforation of the tympanic membrane.
Methods
We performed a retrospective study on 180 patients with type I tympanoplasty. The patients were divided into three groups according to the repair materials used. Age, sex, pre- and postoperative hearing levels, mean air–bone gap, rate of graft success, hearing gain, and the postoperative graft failure rate were evaluated. We continued to follow-up the patients to 1 year after surgery.
Results
The air conduction threshold was significantly higher before the operation than after the operation in the temporalis fascia, partial-thickness cartilage, and full-thickness cartilage groups. Although the hearing gain in the temporalis fascia group and the partial-thickness cartilage group was higher than that in the full-thickness cartilage group, there was no significant difference in the graft success rate among the groups.
Conclusions
Temporalis fascia, partial-thickness cartilage, and full-thickness cartilage can be used as appropriate transplantation materials for tympanoplasty type I in patients with a large perforation. Temporalis fascia and partial-thickness cartilage may be best for improvement of hearing.
Keywords
Introduction
Type 1 tympanoplasty is a surgical technique for closing tympanic membrane perforation and reconstructing the tympanic membrane. This technique is limited to repair of the tympanic membrane. In this technique, the ossicular chain is intact and mobile, without other surgical manipulations in the middle ear. The goal of type 1 tympanoplasty is to obtain an intact tympanic membrane to prevent contamination of the middle ear and fix hearing loss. Frequent upper respiratory tract and middle ear infections, Eustachian tube dysfunction, and immaturity of the immune system contribute to failure of tympanoplasty.
Since tympanoplasty was introduced by Zollner in the 1950s, 1 various types of graft materials and surgical techniques have been developed for repairing tympanic membrane perforations. Although the number of patients with chronic otitis media has been decreasing because of advances in antibiotic treatment, tympanic membrane perforations are common in the otolaryngology clinic. Temporalis fascia and cartilage remain the most widely used graft materials.2–4 However, there is still controversy about which repair material and technology are best.5–8 This study aimed to compare the results of different graft materials in type I tympanoplasty for patients with large tympanic membrane perforations.
Materials and methods
Patient population and grafts
We performed a retrospective study on patients who underwent type I tympanoplasty in our hospital from January 2015 to May 2018. All of the patients had a large perforation of the tympanic membrane (>50%) present at least 3 months before surgery. The patients included in the study were divided into three groups on the basis of the graft material used in type I tympanoplasty. Temporalis fascia was used as the graft material in the temporalis fascia group, partial-thickness cartilage (approximately 1/2 thickness) was used as the graft material in the partial-thickness cartilage group, and full-thickness cartilage was used as the graft material in the full-thickness cartilage group. Before this study, there was a lack of sufficient comparative research on the advantages and disadvantages of these three materials. Surgeons chose graft materials according to their own experience and patients’ aesthetic requirements for the operative area. Patients had temporalis fascia or tragal cartilage used as the graft material. The operations were performed by senior surgeons. Age, sex, the side of the operated ear, the surgical approach, the graft material used, pre- and postoperative audiological results, hearing gain, and the status of the graft at the postoperative period were recorded.
Exclusion criteria were as follows: (1) audiometric loss was not consistent with sole involvement of the tympanic membrane and we excluded patients with a preoperative air–bone gap >45 dB; (2) myringoplasty was a reintervention; (3) patients with perforation for <3 months; (4) patients with a dry ear for <3 months; (5) patients with inadequate ossicular chain function; and (6) patients with other middle ear diseases. All of the patients were informed about the choice of graft material to be used in the operation. All of the patients were informed about this study and provided written informed consent. The study protocol was approved by the ethics committee of Shanxi Provincial People’s Hospital Affiliated to Shanxi Medical University.
Surgery
In the temporalis fascia group, the temporalis fascia was shaped after it had dried, and it was placed over the malleus and under the anterior annulus. The graft was supported by gelfoam medially and laterally. In the partial-thickness cartilage group, the cartilage was thinned to half of its thickness. In the full-thickness cartilage group, tragal cartilage was used as the graft material without thinning. The perichondrium was peeled at the convex side. This technique is called the cartilage perichondrium composite island technique. Otherwise, the surgical procedure was similar to the first group. The graft was supported by a gelatin sponge from the outside. The status of the tympanic membrane and audiometric tests were recorded at the first, third, sixth, and twelfth months postoperatively. Surgical success was defined as an intact graft without perforation or retraction, and a dry ear on the operated side.
Statistical analysis
SPSS version 25.0 software (IBM Corp., Armonk, NY, USA) was used for statistical analyses. The collected data are shown as mean and standard deviation. Statistical analysis with the chi-square test, independent samples t-test, and F-test for a large sample size was performed to examine parameters regarding grafts and hearing improvement, and comparisons were made among the three groups. Statistical significance was considered as P<0.05.
Results
Patient population
A total of 180 patients (88 women, 92 men) who met the criteria were included in this study. The number of patients was the same in each group (60 in each group). The mean age, sex, and onset time were not significantly different among the three groups (Tables 1 and 2).
Distribution of sex among the three groups.

Age and onset time of tympanic membrane perforation among the three groups.

Values are n or mean ± standard deviation.
Audiometric analysis
The preoperative air conduction threshold was significantly higher than the postoperative air conduction threshold in all of the groups (all P<0.001) (Table 3). There was no significant difference in the bone conduction threshold before and after the operation in any of the groups (Table 4). There was a significant difference in hearing gain among the three groups (P<0.001). The hearing gain in the temporalis fascia and partial-thickness cartilage groups was significantly higher than that in the full-thickness cartilage group (both P<0.01), with no difference between the temporalis fascia and partial-thickness cartilage groups (Table 5).
Air conduction before and after the operation in each group.
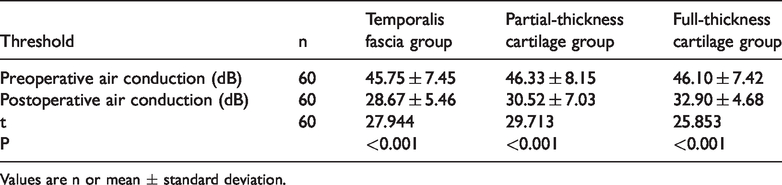
Values are n or mean ± standard deviation.
Bone conduction before and after the operation in each group.

Values are n or mean ± standard deviation.
Comparison of intergroup hearing gain.

Values are mean ± standard deviation. F = 12.763, P<0.001. Multiple comparisons were performed with the least significant difference t-test.
a vs b, P = 0.107.
a vs c, P = 0.000.
b vs c, P = 0.001.
Success rates
The success rate was 96.7% in the partial-thickness cartilage and full-thickness cartilage groups, and >90% in the temporalis fascia group. There was no difference in the success rate among the groups (Table 6).
Success rate among the three groups in each period.

In the temporalis fascia group, there were four cases of infection within 3 months after operation, which led to failure of the operation. In the same period, there were three cases of infection in the partial-thickness cartilage group and four cases in the full-thickness cartilage group, but the operation was not affected by these infections. We observed that, after healing, a normal translucent appearance of the neotympanum in the postoperative period was achieved only in the temporalis fascia group. Two patients in the temporalis fascia group had graft failure because of retraction of graft materials. Graft failure in the partial-thickness cartilage and full-thickness cartilage groups was caused by graft displacement.
Discussion
Tympanic membrane perforation is common in the otolaryngology clinic. Since tympanoplasty was introduced by Zollner in the 1950s, 1 various types of graft materials and surgical techniques have been developed for repair of tympanic membrane perforations.9,10 Which type of graft material provides the most benefit to patients is a matter of concern to surgeons. Whether the success rate of surgery or improvement of hearing is more important needs to be determined. Different patients have different priorities. The results of our study will hopefully lead to surgeons and patients clearly understanding the advantages of various graft materials and making more appropriate choices. Many studies have reported that the success rate of cartilage grafts for closing tympanic membrane perforations is higher than that of other graft materials.11–13 The success rate of using temporalis fascia ranges from 75% to 85%,14–16 and that using cartilage ranges from 91.1% to 95.2%. 17 , 18 However, little attention has been paid to the effect of cartilage thickness on surgical prognosis. In our study, although the success rate of the cartilage groups was higher than that in the temporalis fascia group, there was no significant difference between these groups. We believe that both of these graft materials are suitable for type 1 tympanoplasty in terms of the surgical success rate.
The thickness of cartilage has different effects on improvement of postoperative hearing. 19 We found a significant difference in hearing gain among the three groups The hearing gain in the temporalis fascia group and partial-thickness cartilage group was higher than that in the full-thickness cartilage group. However, there was no significant difference in hearing gain between the temporalis fascia and partial-thickness cartilage groups. This may be related to compliance of the graft materials.
In the temporalis fascia group, there were four cases of infection within 3 months after operation, which led to failure of the operation. In the same period, there were three cases of infection in the partial-thickness cartilage group and four cases in the full-thickness cartilage group, but the operation was not affected by these infections. Therefore, we consider that cartilage as a graft material may have better resistance to infection than temporalis fascia.
Our study has some limitations. Partial-thickness cartilage cannot be accurately measured and needs to be achieved by the experience of the surgeons. Although there was no significant difference in the distribution of patients, the operation was performed by multiple surgeons, and the experience of surgeons may have had an effect on the operative results. The thickness of full-thickness cartilage may vary from patient to patient, which may have an effect on the patient’s hearing. However, we believe that this issue did not affect the conclusion of this study. The success rate of tympanoplasty decreases with time. 20 , 21 The success rate of tympanoplasty with long-term follow-up is lower than that with short-term follow-up. 17 , 22 As the follow-up time increases, more patients have surgical failure.
Conclusions
This study shows that temporalis fascia, partial-thickness cartilage, and full-thickness cartilage can be used as appropriate transplantation materials for tympanoplasty type I in patients with a large perforation of the tympanic membrane. However, temporalis fascia and partial-thickness cartilage may be better for improvement of hearing than full-thickness cartilage. Cartilage as a graft material may have better resistance to infection than temporalis fascia.