
Abstract
Aggressive angiomyxoma is an interstitial tumour that is often misdiagnosed and is likely to recur. There have been few reported cases of angiomyxoma in pregnant women. We report a case of a woman who was previously diagnosed with a tumour in her vulva that increased in size during both of her pregnancies and spontaneously decreased postpartum. Local excision was performed and a gonadotropin-releasing hormone agonist was administered. According to a literature review, aggressive angiomyxoma is associated with good maternal and child outcomes. Caesarean section is not the delivery method of choice, but it is indicated if the tumour is preventing vaginal birth. Treatment for angiomyxoma is mainly postpartum local resection supplemented by hormone therapy. This tumour frequently recurs and patients should undergo long-term follow-up.
Keywords
Introduction
Aggressive angiomyxoma (AA) is a rare interstitial tumour that occurs in the vulva, vagina, pelvis, and perineum in women of childbearing age. 1 Because of local invasion and recurrence of AA, it is relatively difficult to treat in women with fertility requirements and those affected during pregnancy. We report a case of AA during pregnancy. We also review AA cases reported to date in pregnant women to contribute to a better understanding of optimal treatment of these tumours.
Case report
A 25-year-old woman presented with a right vulvar tumour in June 2012 in the second month of her first pregnancy. The tumour was approximately 3 cm in size and gradually increased to 5 cm during pregnancy, with no pain or bleeding. Her medical history and physical examination were otherwise normal. No treatment or procedure was performed for the mass during her pregnancy. She delivered a healthy male neonate in March 2013 at 37 weeks’ gestation with the aid of a left lateral episiotomy. The mass was slightly reduced after delivery. In April 2014, the right vulvar mass was found to have increased to 7 cm. The tumour was partially removed under local anaesthesia. Postoperative pathology showed AA. In a follow-up, no tumour was found in her vulva.
In August 2017, at 2 months’ gestation in her second pregnancy, enlargement of the right labium majus was detected. On 30 January 2018, at more than 30 weeks’ gestation, colour Doppler ultrasound showed that the vulvar tumour was 6 × 4 × 3 cm. In March 2018, at 39 weeks’ gestation, the patient was admitted to hospital owing to a reduction in conscious foetal movement. At that time, the right vulvar mass was soft and approximately the size of an egg (Figure 1). A caesarean section was performed owing to foetal distress, and the patient delivered a healthy female neonate. In follow-up in May 2018, no obvious mass was found in the vulva.

Right labium majus mass at 39 weeks’ gestation.
In January 2019, the mass spontaneously increased again, and blood tests showed normal ranges for CA125, CA199, CA153, carcinoembryonic antigen, and alpha fetoprotein levels. Magnetic resonance imaging (MRI) showed irregular, short T1 and long T2 signal shadows on the right side of the vulva. Diffusion-weighted imaging showed uneven, slightly high signal shadows with a range of 5.3 × 5.1 × 4.2 cm. The upper edge of the mass was close to the lower edge of the pubic symphysis. An enhanced scan showed homogeneous enhancement of the lesion (Figure 2). On 21 February 2019, the genital tumour was removed. The swelling of the mass was soft and irregular and a small area was connected to fat. Postoperative pathology suggested invasion of vascular myxoma (Figure 3). Immunohistochemistry showed that the tumour was vimentin +++ (Figure 4), oestrogen receptor ++, progesterone receptor ++, desmin +, Ki-67 + (<1%), S-100 (−), and alpha-smooth muscle actin (−). Postoperatively, three intramuscular injections of the gonadotropin-releasing hormone agonist triptorelin (3.75 mg) were administered, and no recurrence was observed in 9 months of follow-up.

Postpartum magnetic resonance imaging scan. In coronal fat-suppressed T2-weighted imaging sequences, lesions with a high signal (white arrow) are located in the deep part of the right vulva. The boundary is clear, the internal signal is not uniform, and a strip-shaped low signal shadow (black arrow) can be seen.

Histopathology of the tumour. Haematoxylin and eosin staining (×100) shows spindle to stellate cells in a loose myxoid matrix (labelled as M) with variable sized blood vessels (labelled as V).

Immunohistochemistry of the aggressive angiomyxoma. The tumour cells are positive for vimentin (×200).
The study was approved by Fujian Provincial Maternity and Children’s Hospital, Affiliated Hospital of Fujian Medical University, Fuzhou, Fujian, China. Details were de-identified to protect the identity of the patient. Verbal consent from the patient was obtained for publication of data and images.
Discussion
The first case of AA in pregnancy was reported in 1995, and only 16 cases have been reported in pregnancy to date (Table 1).2–15 The cause of AA is unknown. Our case was similar to most cases of AA in pregnancy. Our patient was asymptomatic and the mass was usually painless. These tumours tend to expand during pregnancy.
Characteristics of reported cases of aggressive angiomyxoma in pregnancy.
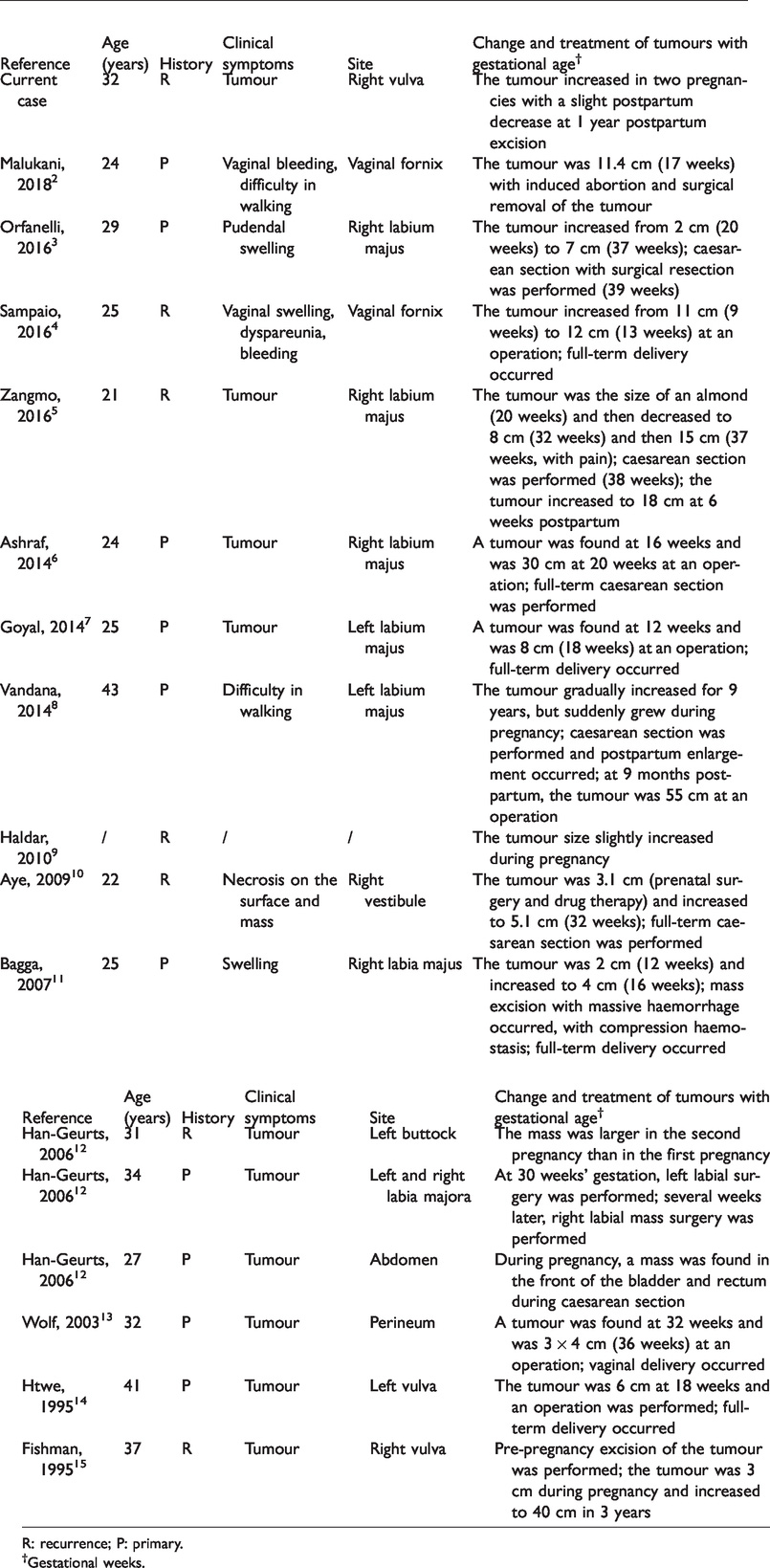
R: recurrence; P: primary.
†Gestational weeks.
AA is often misdiagnosed as Bartholin’s gland cyst, lipoma, or a vaginal wall cyst. MRI is the preferred examination method of AA and it can show the scope of the tumour and its relationship with the pelvic diaphragm and surrounding organs. AA has certain characteristics on MRI, such as multiple twisted strip shadows, showing “whirlpool” or “stratified” changes. AA may also be confused with spindle cell lipoma, myxoid neurofibroma, intrauterine myxoma, and myxoid liposarcoma. Pathology is the preferred standard for diagnosing AA. This tumour can be variable in size, and its general characteristics usually include a lobulated or spherical appearance, soft texture with no capsule or a partial capsule, and frequently an unclear boundary within the surrounding tissue is observed. The tumour section is translucent, grey white, or grey brown, and it has a homogeneous jelly-like consistency, with cystic changes and a bleeding area. Microscopically, the tumour comprises short fusiform cells, with a uniform size and without obvious heteromorphism. The stroma is rich in an oedematous mucoid and collagen matrix, and there are many thin-walled and thick-walled vessels. Although there is no specific immunohistochemical marker in AA, vimentin and CD34 are strongly positive, and desmin, oestrogen receptor, and progesterone receptor are moderately positive. Additionally, S-100 is not generally expressed and Ki-67 has a low proliferation index (<1% tumour cells). These characteristics are helpful during differential diagnosis.
Most AAs are located in the vulva or vagina, and a tumour is the main clinical manifestation. Pain or bleeding are uncommon, but pain may occur if the tumour is significantly enlarged, 5 and vaginal bleeding may be noted with sexual intercourse. 4 In most cases, AA is found in the early and middle stages of pregnancy (n=11), and a few are found in late pregnancy. 13 The extent of tumour enlargement during pregnancy varies from a slight increase 9 to growth of several times the original tumour size. 5 Similar to most pregnancies with AA, our patient had full-term delivery at both pregnancies, and had a good maternal and neonatal outcome. Although the majority of patients with AA choose caesarean section, vaginal delivery is feasible. 13 In our patient, the lateral perineum was used for vaginal delivery in the first pregnancy.
AA has an abundant blood supply, and there is a risk of massive bleeding during pregnancy. If there is no pain or bleeding, tumours can be treated postpartum and may even be spontaneously reduced after delivery, as in our case. Surgical resection is the main treatment for AA. For AA with extensive and deep infiltration of pelvic organs, incomplete resection is recommended if complete resection is not feasible or may cause serious surgical injury. Studies have shown that surgical margins have no effect on recurrence of AA. 16
The prevalence of AA in women of childbearing age, tumour growth during pregnancy, and the majority of cases with oestrogen and progesterone positive receptors suggest that AA tumours may be hormone-dependent. Therefore, hormone therapy is considered a possible effective treatment option. Some scholars believe that hormone therapy should be administered to patients with postoperative residual disease or in treatment of initial small lesions. 17 However, whether long-term use of a gonadotropin-releasing hormone agonist can cure the disease or whether there is recurrence after stopping the drug is unclear.
Usually, the recurrence site is consistent with the initial site of AA. However, there is no clear relationship between the patient’s age, tumour size, number of pregnancies, and recurrence rate. Because the tumours are soft and can invade the pelvic organs, they may be missed on a clinical examination. Follow-up for AA should be supplemented by MRI studies.
In summary, the main clinical feature of AA in pregnancy is enlargement of the tumour. The outcomes for the mother and child are good. Although birth in most cases is by caesarean section, this is not the delivery method of choice. Caesarean section is indicated only if the tumour is preventing vaginal birth. Surgical resection is still the most important treatment and hormone therapy can be used as adjuvant therapy for AA. Although metastasis is rare, AA is prone to recurrence. Therefore, long-term, regular follow-up is important for this tumour.