
Abstract
Objective
To evaluate the efficacy and safety of multiple- versus single-dose gonadotropin-releasing hormone agonist (GnRH-a) addition to luteal phase support (LPS), in patients with a first in vitro fertilization (IVF) failure associated with luteal phase deficiency (LPD).
Methods
Eighty patients with a first IVF failure associated with LPD were randomly assigned into single-dose and multiple-dose GnRH-a groups. In the second IVF attempt, patients in the single-dose group were given standard LPS plus a single dose of GnRH-a 6 days after oocyte retrieval. Patients in the multiple-dose group received standard LPS plus 14 daily injections of GnRH-a. Children conceived were followed up for 2 years.
Results
Pregnancy (67.5% vs. 42.5%), clinical pregnancy (50.0% vs. 22.5%), and live birth rates (42.5% vs. 20.0%) were significantly higher in the multiple-dose versus single-dose GnRH-a group. Patients in the multiple-dose GnRH-a group had significantly higher progesterone levels 14 days after oocyte recovery (35.9 vs. 21.4 ng/mL). No significant difference existed in the status at birth or developmental and behavior assessments of 2-year-old children conceived in both groups.
Conclusions
Daily addition of GnRH-a to standard LPS can achieve better pregnancy outcomes with a sustained safety profile in patients with a first IVF failure associated with LPD.
Keywords
Introduction
Luteal phase deficiency (LPD) is mainly caused by impaired secretory function of the corpus luteum, resulting in low estradiol and progesterone levels and shortening of the luteal phase. 1 In the context of in vitro fertilization (IVF) attempts, LPD is common in follicular stimulation using any kind of ovarian stimulation protocol. Luteal phase support (LPS) is considered essential to correct LPD in infertility treatment. The first LPS modalities were the administration of human chorionic gonadotropin (hCG) and progesterone. 2 However, LPS with hCG increases the risk of ovarian hyperstimulation syndrome compared with progesterone.3,4 Progesterone for LPS can be administered vaginally, orally, or intramuscularly, but the optimal route of administration has not been established. Some other modalities are under investigation; for example, estrogen, steroids, ascorbic acid, and acupuncture. 5
Recent studies have proposed the use of a gonadotropin-releasing hormone agonist (GnRH-a) as LPS. The first report of GnRH-a in LPS by Tesarik et al. 6 retrospectively demonstrated that GnRH-a administration at the time of implantation could significantly improve implantation and birth rates and enhance embryo developmental potential. Several studies have since exhibited a positive effect of GnRH-a as LPS.7,8
LPD is well accepted as one of the first factors contributing to infertility. Moreover, if LPD cannot be diagnosed correctly, it contributes to IVF failure.9,10 The diagnostic criteria of LPD remain a matter of debate. Some studies define LPD as a single progesterone level below 10 ng/mL (31.8 nmol/L) in the mid-luteal phase.11,12 Recent studies have revealed that a cutoff serum progesterone level of 15 ng/mL (47.7 nmol/L) on the day of pregnancy test exhibited 100% sensitivity for detecting LPD.11,13 Zafardoust et al. 14 reported that single-dose GnRH-a in the luteal phase could improve implantation and clinical pregnancy rates in patients with previous IVF-embryo transfer (ET) failure. Mendoza-Tesarik et al. 15 found that GnRH-a treatment for 2 weeks could improve pregnancy and birth rates in patients with a first IVF failure associated with LPD. However, there have been relatively few studies on the effect and long-term safety of GnRH-a as LPS in patients with previous IVF failure. In addition, optimal use of GnRH-a remains undetermined. The present study aimed to explore the efficacy and safety of single-dose and multiple-dose GnRH-a as LPS in patients with first IVF failure associated with LPD.
Materials and methods
Patients
This was a prospective randomized controlled study in a 1:1 allocation ratio conducted in the assisted reproduction technology unit of a tertiary university hospital in Beijing. Patients who underwent a second IVF-ET treatment between January 2013 and January 2016 were considered for participation in our study. Patients were divided into two groups using the random block allocation method. The inclusion criteria were as follows: (1) between 22 and 40 years old; (2) failure to achieve clinical pregnancy in their first IVF attempt with LPD after ET; (3) treatment cycles with controlled ovarian hyperstimulation (COH) and fresh ETs. LPD during the first attempt was defined as a serum progesterone level <15 ng/mL on day 14 after oocyte retrieval in patients receiving standard LPS treatment. Women with an abnormal uterine cavity or with frozen ET cycles were excluded.
The study was approved by the Ethics Committee of Beijing Chaoyang Hospital. All procedures that involved human participants were in accordance with the ethical standards of the Institutional and National Research Committee, with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The Consolidated Standards of Reporting Trials (CONSORT) recommendations were followed in this study. Informed consent was obtained from all participants enrolled for the study.
COH protocol
Ovarian stimulation was carried out using recombinant human follicle stimulating hormone (rFSH; Gonal-F; Merck Serono, Geneva, Switzerland) and human menopausal gonadotropin (hMG, Livzon, Zhuhai, China). Serial transvaginal ultrasound was performed to monitor follicular growth. The doses of rFSH and hMG were adjusted according to follicular development and serum estradiol and luteinizing hormone (LH) levels. When at least three follicles reached a mean diameter of 18 mm, ovulation was induced with a single dose of 10,000 IU of recombinant human chorionic gonadotropin (hCG). After 36 hours, transvaginal ultrasound-guided oocyte retrieval was performed. Fertilization was achieved with intracytoplasmic sperm injection (ICSI) in all couples, and ET was performed on day 3 following ICSI. One or two embryos were implanted depending on maternal age. All women were treated with vaginal 8% progesterone gel, 90 mg/d (Crinone, Merck Serono, Rockland, MA, USA) plus dydrogesterone tablets (Duphaston, Abbott Laboratories, Chicago, IL, USA), 20 mg/d, starting on the day of oocyte retrieval and continuing until the pregnancy test performed 14 days after ET.
Data on participants’ characteristics, COH, and embryology were collected. These included maternal age; type, duration, and cause of infertility; ovarian reserve assessment [cycle day 3 anti-Müllerian hormone (AMH) and FSH levels]; duration and total dose of gonadotropin (Gn) treatment; endometrial thickness on the day of hCG administration; number of retrieved oocytes; and number of embryos transferred.
All participants were randomized into one of two groups by a computer-generated program. Women allocated to the single-dose GnRH-a group received a single dose of 0.1 mg decapeptyl 6 days after oocyte retrieval, whereas women allocated to the multiple-dose GnRH-a group received an additional daily injection of 0.1 mg decapeptyl for 14 days starting from the day of oocyte retrieval. Investigators and participants were not blinded to treatment allocation.
Primary and secondary effect outcome measures
Primary effect outcomes of the study were pregnancy outcomes, including pregnancy rate, clinical pregnancy rate, and live birth rate. Pregnancy was assessed by measuring serum β-hCG levels 14 days after embryo transfer, and clinical pregnancy was confirmed by the presence of an intrauterine gestational sac on ultrasonography 5 weeks after embryo transfer. Clinical pregnancy rate was calculated as the number of clinical pregnancies divided by the number of ET procedures. Live birth rates were defined as the percentage of assisted reproductive technology (ART) cycles started that resulted in a live birth. The outcome “birth defect” was defined as a structural defect of the body that affects quality and viability of life and that requires medical intervention. The secondary effect outcomes were serum progesterone concentrations, measured on day 14 after ET.
Safety outcome measures
Safety outcome was based on measures of motor, cognitive, language, and behavioral development of children conceived by the study cohort. When IVF-ET children were 24 months old, developmental-behavior assessments were performed. The developmental-behavior assessments consisted of four domains: motor, cognitive, language, and behavioral development. The Bayley Scales of Infant Development (3rd ed., Bayley-III), a multidisciplinary battery, was used to assess motor, cognitive, and language development. The motor scale of Bayley-III assesses gross and fine motor skills; the cognitive scale measures non-verbal activities including sensorimotor development, object exploration, and concept formation; and the language scale estimates receptive and communicative skills. The Bayley-III scores were converted to a standardized mean value of 50 and a standard deviation (SD) of 10, with higher scores reflecting better performance. Behavior assessment was assessed using the Child Behavior Checklist (CBCL). The CBCL consists of 100 items describing sleep problems, withdrawal, somatic problems, depression, and aggressive and destructive behavior. Raw scores were normalized into T-scores with a mean value of 50 and an SD of 10.
Statistical analysis
A pilot study at our institution (8 patients per group) demonstrated a 25% difference in pregnancy rates between two groups. Power analysis indicated that a sample size of at least 37 patients per group would provide a power of 80% at an α level of 0.05 (two-tailed test). Thus, we aimed to enroll 40 patients in each group.
Continuous data were expressed as mean ± SD or median (interquartile range) and were compared with the Student’s t test, Mann-Whitney U test, or Wilcoxon rank sum test. Categorical data were expressed as number (percentage) and compared with Fisher’s exact test or the Chi-square test. We performed subgroup analyses in both groups by comparing singleton and multiple pregnancies. Statistical significance was considered at a two-tailed P < 0.05. Statistical analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA).
Results
Participant characteristics at baseline
Eighty patients were enrolled in this study, in two groups: single-dose GnRH-a (n = 40) and multiple-dose GnRH-a (n = 40). The study flowchart is depicted in Figure 1. The baseline characteristics of the patients in the two groups, including maternal age, BMI, menstrual cycle, infertility cause, and duration of infertility, were similar, as shown in Table 1.

CONSORT flow diagram of the study cohort.
Baseline characteristics of the study cohort.

GnRH-a, gonadotropin-releasing hormone agonist; BMI, body mass index.
Fresh cycle characteristics
The fresh cycle characteristics of the patients are depicted in Table 2. We found no differences in AMH level, FSH level, Gn dose, Gn duration, average endometrial thickness, average number of retrieved oocytes, or average number of transferred embryos between the two groups.
Fresh cycle characteristics of the study cohort.

GnRH-a, gonadotropin-releasing hormone agonist; AMH, anti-Müllerian hormone; FSH, follicle-stimulating hormone; Gn, gonadotropin.
IVF-ET pregnancy outcomes
Compared with the single-dose GnRH-a group, patients in the multiple-dose GnRH-a group demonstrated higher rates of pregnancy (P = 0.025), clinical pregnancy (P = 0.011), and live birth (P = 0.030), as shown in Table 3. There were no significant differences between patients in the single-dose GnRH-a and multiple-dose GnRH-a groups regarding delivery outcomes: preterm birth [1/8 (12.5%) vs. 1/17 (5.9%)] and low birth weight [1/8 (12.5%) vs. 1/17 (5.9%)]. All pregnancies resulted in the birth of healthy babies.
Pregnancy outcomes following in vitro fertilization-embryo transfer.

GnRH-a, gonadotropin-releasing hormone agonist.
Serum progesterone levels
There was no difference in serum progesterone level on the day of ET between the two groups. However, on day 14 after ET, serum progesterone levels of patients in the multiple-dose GnRH-a group were significantly higher than those of the single-dose GnRH-a group (P < 0.001; Table 4). In the subgroup analysis (Table 5), both pregnant and nonpregnant patients of the multiple-dose GnRH-a group had higher serum progesterone levels (P = 0.002 and P = 0.003, respectively) than those of the single-dose GnRH-a group.
Luteal phase characteristics of the study cohort.
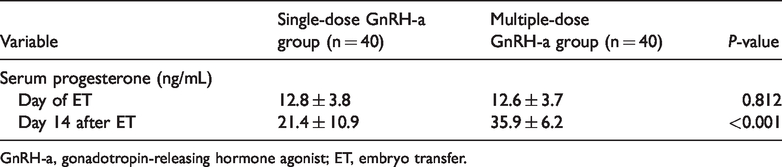
GnRH-a, gonadotropin-releasing hormone agonist; ET, embryo transfer.
Subgroup analysis of luteal phase characteristics.
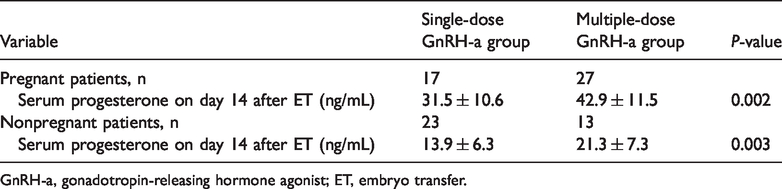
GnRH-a, gonadotropin-releasing hormone agonist; ET, embryo transfer.
Long-term follow-up of children conceived by the study cohort
Table 6 summarizes the results of Bayley-III motor, cognitive, and language assessments and CBCL behavior assessment performed when the children of IVF-ET patients were 24 months old. We observed no significant differences in motor, cognitive, language, or behavioral outcomes between the two groups.
Long-term follow-up of children conceived by the study cohort.
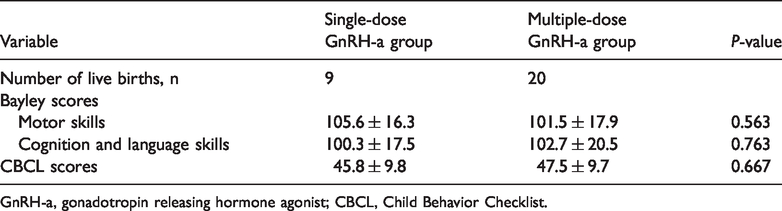
GnRH-a, gonadotropin releasing hormone agonist; CBCL, Child Behavior Checklist.
Discussion
LPD has been identified in all ARTs. To overcome this issue, additional LPS has been routinely used during ART-stimulated cycles to improve pregnancy outcomes. 16 GnRH-a is considered a novel LPS. In 1993, Balasch et al. 17 reported the first study of inadvertent administration of GnRH-a in the mid-luteal phase, which did not compromise pregnancy outcomes but rather enhanced implantation rates. A series of studies have since demonstrated that addition of GnRH-a during the luteal phase can significantly increase rates of clinical pregnancy, ongoing pregnancy, and live births.8,18–21
Although the exact mechanism of GnRH-a in the mid-luteal phase remains unclear, the major beneficial effect of GnRH-a administration in this phase is postulated to work at three levels: the corpus luteum, the endometrium, and the embryo. GnRH-a can support corpus luteum maintenance by activating the secretion of LH by pituitary gonadotropic cells. 22 GnRH-a can directly bind GnRH receptors on the endometrium, simulate the production of angiogenic growth factors, and decrease natural killer cytotoxicity, making the endometrium more favorable for embryo implantation. 23 Additionally, some researchers believe that GnRH-a can have a direct beneficial effect on early embryo development, as indicated by increased hCG, progesterone, and estradiol levels.6,23
Many studies have confirmed that a single administration of GnRH-a can enhance the clinical outcomes of IVF-ET treatment.6,8,9,14 Administration of multiple boluses of GnRH-a in LPS protocols has become more common. Pirard et al. 24 published the results of a prospective, randomized controlled clinical trial, in which daily administration of GnRH-a, as the only LPS for 10 to 16 days, achieved rates of pregnancy, implantation, and clinical pregnancy comparable to the standard LPS with intravaginal progesterone. Bar-Hava et al. 25 showed that daily continuous administration of GnRH-a for 2 weeks, as the only LPS, supported and enabled fresh embryo implantation with satisfactory clinical pregnancy rates. Recently, Mendoza-Tesarik et al. 15 found that daily supplementation of GnRH-a during luteal support for 2 weeks in patients with a first IVF failure resulted in higher pregnancy and clinical pregnancy rates in their second IVF attempts. However, no study has compared single-dose and multiple-dose GnRH-a as LPS for IVF-ET. To the best of our knowledge, ours is the first study to make this comparison. Our data showed that daily repeated GnRH-a administration had pronounced beneficial effects on pregnancy, clinical pregnancy, and live birth outcomes. This improvement over the single-dose regimen probably reflects the short-action duration of GnRH-a, which has a half-life of 3 hours in plasma after a subcutaneous injection of 1.0 mg. 26
Although GnRH-a, as LPS, appears to exert beneficial effects on the achievement of clinical pregnancy, concerns remain regarding the safety of GnRH-a. In 1998, Cahill 27 reported 346 unexpected spontaneous pregnancies in patients exposed to GnRH-a for 10 to 20 days in early pregnancy. Among these pregnancies, congenital abnormality and pregnancy loss rates were 2.5% and 15%, respectively, approximately the same as the rates in the population at large. However, Sahin et al. 28 reported that GnRH-a triggered IVF cycles and had higher ectopic pregnancy rates relative to hCG-triggered cycles, which was probably caused by the decreased receptivity of the endometrium due to insufficient luteal support. Zhou et al. 29 showed that addition of a single dose of GnRH-a to progesterone did not increase the risk of complications during pregnancy, at delivery, or postpartum. A recent study published by Bar-Hava et al. 25 revealed that daily administration of GnRH-a for 2 weeks did not have any long-term adverse effects. Our study used the Bayley-III and CBCL scores to assess the developmental behaviors at 2 years old of children conceived by the study cohort. The Bayley-III and CBCL scores of the study cohort were comparable to those of ART-conceived children reported by Balayla et al. 30 and Zhan et al., 31 which indicates the safety of GnRH-a as LPS.
In this prospective randomized controlled study, we investigated and compared the efficacy and safety of single and multiple doses of GnRH-a with progesterone as LPS on pregnancy, delivery, and postpartum outcomes. We selected patients who had a first IVF failure associated with LPD. Our results indicated that continuous supplementation of GnRH-a could support the luteal phase, as indicated by higher serum progesterone levels in the mid-luteal phase in the multiple-dose GnRH-a group, which resulted in higher rates of pregnancy, clinical pregnancy, and live birth compared with the single-dose GnRH-a group. Additionally, during the 2-year follow-up, children conceived by the study cohort had developmental behaviors similar to those reported in ART-conceived children.
Our study had several limitations. First, the study cohort consisted of a relatively small sample from a single institution. Additional studies with multi-institutional cohorts are warranted to validate the study findings. Second, although we speculate that GnRH-a alone is sufficient for LPS, patients in both GnRH-a groups of the present study were also administered transvaginal progesterone, primarily for ethical reasons. We intend to solve this issue in a future study.
In summary, in the present study, we showed that daily addition of GnRH-a to luteal support achieved better pregnancy outcomes with a sustained safety profile in patients who had a first IVF failure associated with LPD.