
Abstract
Objective
We aimed to investigate factors associated with nonadherence to antihypertensive medication among middle-aged Taiwanese adults with hypertension.
Methods
We used data from the 2009 Taiwan National Health Interview Survey (NHIS) to identify adults age 40 to 65 years with hypertension. We used logistic regression analyses to investigate factors associated with nonadherence to antihypertensive medication.
Results
A total 1,256 respondents with hypertension taking antihypertensive medication were included in this study. Multiple logistic regression analyses revealed that six factors were significantly and independently associated with nonadherence to medication: younger age (odds ratio, [OR] = 1.85), mean monthly personal income < TWD 20,000 (USD 660) (OR = 1.87), outpatient medical services use in the past month (OR = 0.57), hospitalization in the past year (OR = 1.70), diabetes or dyslipidemia (OR = 0.63), and alcohol use in the past month (OR = 2.38).
Conclusions
This secondary data analysis of the population-based NHIS identified six factors associated with nonadherence to antihypertensive medication. These factors should be considered when planning and implementing blood pressure control interventions among middle-aged adults with hypertension.
Keywords
Introduction
Hypertension is a public health challenge worldwide and is ranked as a leading risk factor in the global disease burden. 1 The estimated total number of adults with hypertension in 2000 was 972 million, and this is projected to reach 1.56 billion by 2025. 2 Nevertheless, awareness about and treatment adherence for hypertension remain suboptimal, particularly among people under 65 years of age. 3
Poor blood pressure control is an important risk factor for morbidity and mortality. 4 A systematic review of 123 studies showed that a 10-mm Hg decrease in systolic blood pressure could lead to a 13% reduction in all-cause mortality. In addition, lowering blood pressure can significantly reduce the risk of major cardiovascular events, coronary heart disease, stroke, and heart failure. 5
Blood pressure control includes the use of antihypertensive medication and lifestyle modifications; however, poor adherence to antihypertensive medication is a key contributor to uncontrolled hypertension;6,7 which is associated with various adverse cardiovascular events, 8 faster progression of chronic kidney disease, 9 and mortality. 10 Therefore, the aim of this study was to investigate those factors associated with nonadherence to antihypertensive medication among middle-aged adults with hypertension, using population-based survey data.
Methods
Data source and study sample
The study protocol was approved by the institutional review board of Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation (No. B10302017). Because the data file used in this study contains only deidentified secondary data, the requirement for obtaining informed consent from patients was waived.
The data source of this study was the 2009 National Health Interview Survey (NHIS), which was a nationally representative, population-based survey conducted jointly by the National Health Research Institutes and Bureau of Health Promotion, both under the Ministry of Health and Welfare in Taiwan. The NHIS used a multi-stage stratified systematic sampling scheme with face-to-face interviews using structured questionnaires. 11
Nonadherence was defined in this study as not regularly taking physician-prescribed antihypertensive medication, based on a question in the NHIS.
We evaluated 15 factors that could potentially be associated with nonadherence: six sociodemographic factors (age, sex, marital status, educational level, living arrangements, and personal income level), five health-related factors (diabetes or dyslipidemia, body mass index, outpatient medical services use in the past month, hospitalized in the past year, and self-perceived health status), and four health behavior factors (exercise in the past 2 weeks, smoking, alcohol consumption, and betel nut chewing).
Statistical analysis
All statistical analyses were performed using IBM SPSS version 24.0 (IBM Corp, Armonk, NY, USA). Univariate and multiple logistic regression analyses were used to evaluate factors associated with nonadherence. The assumption of collinearity was evaluated using variance inflation factors, and goodness of fit was assessed using the Hosmer–Lemeshow test. A two-tailed P value of < 0.05 was considered statistically significant.
Results
A total of 30,528 (1.33%) eligible individuals were sampled from the total population of Taiwan (22,942,706 as of December 31, 2008), and 25,632 individuals completed the survey (84.0% response rate). Among these, 8,639 respondents were aged 40 to 65 years. We further selected 1,366 respondents with self-reported clinically diagnosed hypertension. In addition, we excluded 21 respondents with cancer, 51 with mental illnesses, and 38 respondents with missing data. Therefore, 1,256 respondents were finally included in the analyses.
Of the 1,256 respondents who satisfied the inclusion criteria for this study, 1,039 (82.7%) regularly took antihypertensive medication. Table 1 shows the distribution of the factors evaluated in this study. For demographic factors, 72.8% of respondents were between 50 to 65 years of age, 53.4% were men, 79.1% were either married or living together with someone, 56.1% had an educational level of junior high school or below, 7.6% were living alone, and 56.7% had a mean monthly personal income of < TWD 20,000 (USD 660). Regarding health-related factors, over 71.2% of respondents were either overweight or obese, 51.6% had diabetes or dyslipidemia, 54.0% had used outpatient medical services in the past month, 10.5% were hospitalized in the past year, and 58.0% indicated that their health status was fair or poor. Regarding health behavior factors, 59.2% of respondents had exercised in the past 2 weeks, 79.5% were non-smokers, 71.2% did not consume alcohol in the past month, and 90.0% did not have a betel nut chewing habit.
Univariate logistic regression analyses of nonadherence to antihypertensive medication among middle-aged adults (N = 1,256).
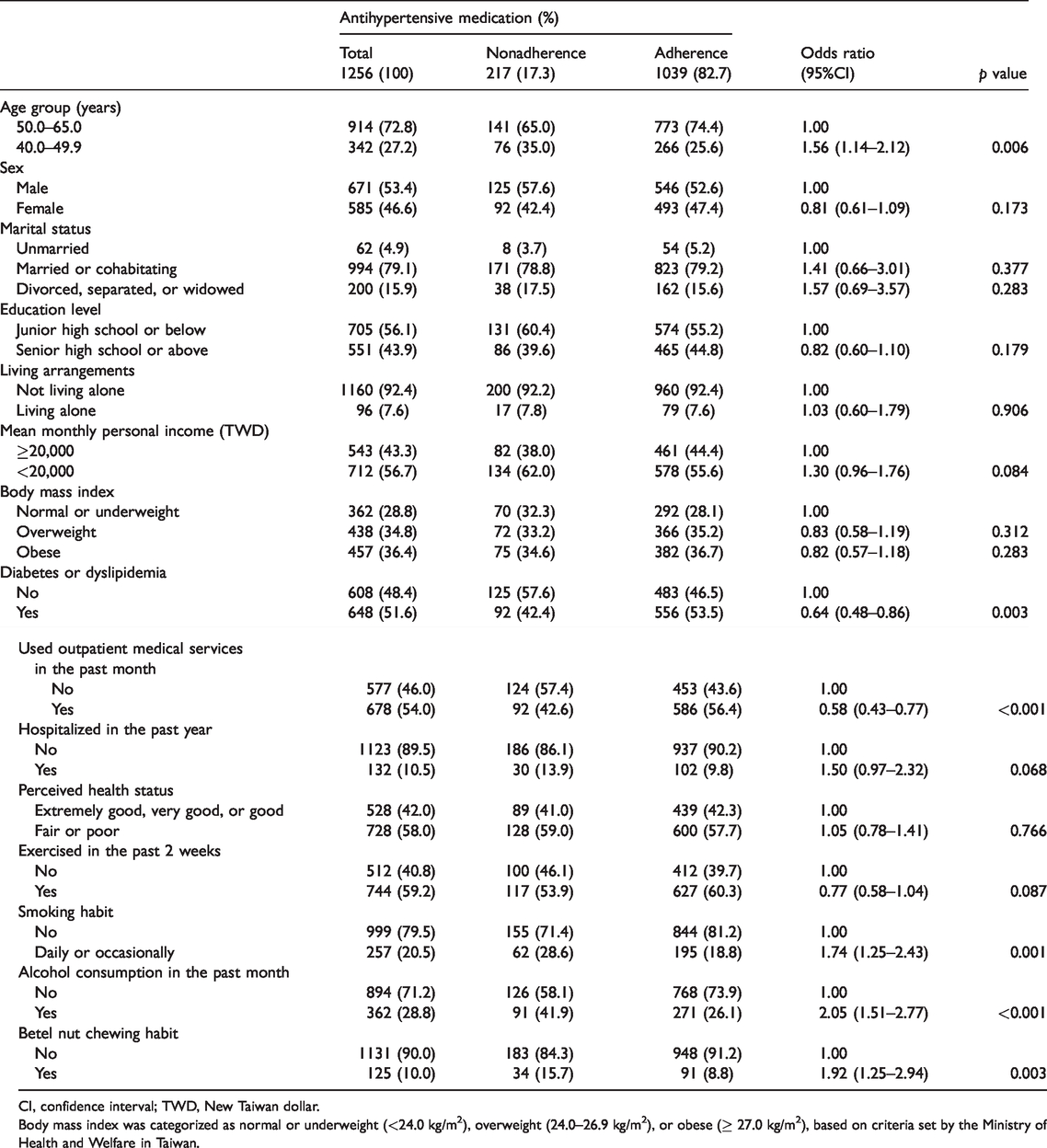
CI, confidence interval; TWD, New Taiwan dollar.
Body mass index was categorized as normal or underweight (<24.0 kg/m2), overweight (24.0–26.9 kg/m2), or obese (≥ 27.0 kg/m2), based on criteria set by the Ministry of Health and Welfare in Taiwan.
Table 1 also shows the results of univariate logistic regression analyses for nonadherence to antihypertensive medication. Of the 15 factors, six were significantly associated with nonadherence to antihypertensive medication. The results of multiple logistic regression analysis for nonadherence to antihypertensive medication are shown in Table 2. Six factors were found to be significantly and independently associated with nonadherence to antihypertensive medication: aged 40 to 49 years versus 50 to 65 years (odds ratio [OR] = 1.61, P = 0.005), mean monthly personal income of < TWD 20,000 (USD 660) (OR = 1.87, P < 0.001), hospitalization in the past year (OR = 1.70, P = 0.023), and consumed alcohol in the past month (OR = 2.38, P < 0.001). Conversely, outpatient medical services use in the past month (OR = 0.57, P < 0.001) and diabetes or dyslipidemia (OR = 0.63, P = 0.003) were inversely and significantly associated with nonadherence.
Multiple logistic regression analysis of nonadherence to antihypertensive medication among middle-aged adults (N = 1256).

Hosmer and Lemeshow goodness of fit test, p = 0.451.
CI, confidence interval; TWD, New Taiwan dollar.
Discussion
Findings from our secondary analysis of a population-based survey revealed that 82.7% of respondents used antihypertensive medication regularly. The level of antihypertensive medication adherence in Taiwan was similar to that reported in South America 12 and higher than the 50% reported in a Vietnamese study 13 and the 56% in a Middle East study. 14 A retrospective population-based study using the Taiwan National Health Insurance Research Database (NHIRD) found that 52.9% of patients had high antihypertensive medication adherence, which was defined as a medication possession ratio (MPR) ≥80%. 15 However, using the MPR as a measure of compliance, a cohort study among 83,884 Chinese patients revealed that 85.5% of them had good compliance with antihypertensive medication. 16 Another study among 1,523 Korean patients with hypertension who visited a family physician also reported that 81.7% had good adherence to antihypertensive medication. 17 The differences in study findings might be explained by variations in the design and definition of adherence among studies. Nevertheless, the relatively high adherence in the present study might be partly explained by the fact that the cost of medical care and medications should not be a barrier to adherence because Taiwan has had universal health insurance coverage since 1995. 18
Our study revealed six factors that were significantly and independently associated with nonadherence to antihypertensive medication, including younger age. This finding is consistent with the conclusion from prior studies that older age was associated with better medication adherence.19–21 It has been suggested that older individuals might be more concerned about their health and receive better support from health care providers or family members, resulting in better adherence. 22
A mean personal income of less than TWD 20,000 (USD 660) per month was found to be associated with medication nonadherence in this study. Based on electronic pharmacy administrative data, Rolnick et al. 23 reported that medication adherence, assessed using the MPR, was significantly associated with higher income in patients with various diseases, including hypertension. A recent meta-analysis of 30 studies also concluded that high socioeconomic status was significantly associated with a low risk of nonadherence. 24 Although the National Health Insurance scheme was implemented to provide Taiwan’s population with affordable health care services, physical access to health care resources remains unequal across the country. 18 Whether this inequality in access to health care might explain the association between socioeconomic status and nonadherence deserves further investigation.
In this study, we found that the use of outpatient medical services in the past month was significantly associated with a low risk of nonadherence. This finding might reflect convenient access to health care facilities, which could contribute to adherence. In addition, outpatient visits might provide an opportunity to monitor treatment, discuss adverse effects, and provide patient education on medication adherence. A cross-sectional analysis of 49,479 Medicaid patients with hypertension also revealed that outpatient visits were associated with decreased nonadherence. 25
We found that hospitalization in the past year was significantly associated with nonadherence to antihypertensive medication. Our finding was similar to that of a population-based, prospective, observational study among community-dwelling older adults in which hospitalization during the previous 6 months was an independent factor significantly associated with nonadherence. 26 A possible reason for this is confusion caused by a change in the medication regimen during and after hospitalization, particularly among individuals with low health literacy. 27
Individuals with diabetes or dyslipidemia were found to have a significantly lower risk of nonadherence. This finding is similar to that of a study including 1,523 patients with hypertension in a Korean family practice. Patients with good adherence were more likely to be taking concomitant medications for diabetes and dyslipidemia. The authors suggested that patients with concomitant comorbid conditions might be more aware of having a higher disease risk and thus show better adherence. 17
In terms of health behavior factors, only alcohol use in the past month was significantly and independently associated with nonadherence to antihypertensive medication in our study. A systematic review indicated that alcohol consumption was associated with medication nonadherence in various chronic diseases, which was suggested to be caused by forgetfulness related to alcohol use or intentionally avoiding potential drug interactions. 28
There are several limitations in our study that should be noted. First, our data were based on the Taiwan NHIS, and variables available for the analyses were limited by those included in the survey. For example, information about the class of antihypertensive medication, the medication regimen, and the presence of adverse effects were unavailable. Second, because the data were based on self-reporting, misclassification owing to recall error cannot be completely ruled out. Nevertheless, self-reports have been shown to provide estimates of adherence similar to those of pharmacy refill and electronic adherence measures. 29 In addition, a recent study comparing the agreement between self-reports and medical records among 3601 middle-aged and older adults in Taiwan showed that the consistency between self-reports and medical data was excellent for diabetes (Kappa = 0.80) and good for hypertension (Kappa = 0.67). 30 Third, this study was based on a cross-sectional design; therefore, causal relationships could not be established.
In conclusion, findings from this secondary analysis of a national, population-based health survey revealed a number of significant and independent factors associated with nonadherence to antihypertensive medication. These factors should be considered when planning and implementing blood pressure control intervention among middle-aged adults with hypertension.
Footnotes
Acknowledgments
This study is based on data from the National Health Interview Survey provided by the Health Promotion Administration, Ministry of Health and Welfare, Taiwan. The interpretation and conclusions contained herein do not represent those of the Health Promotion Administration, Ministry of Health and Welfare, Taiwan who provided all of data.
Data availability
The data used to support the findings of this study are available from the corresponding authors upon request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.