
Abstract
Objective
Patients with type 2 diabetes (T2DM) are prone to cardiovascular disease, and both conditions are linked to oxidative DNA damage, which produces 8-hydroxy-2′-deoxyguanosine (8-OHdG). We investigated the impact of 8-OHdG on coronary heart disease (CHD) in elderly patients with T2DM.
Methods
We assessed the demographic, clinical, and biochemical characteristics of 147 patients with T2DM (mean age 73.29 ± 8.19 years) with or without CHD. Serum 8-OHdG was detected by enzyme-linked immunosorbent assay. CHD was diagnosed as ≥50% stenosis in at least one main branch of the coronary arteries determined by coronarography, evaluated by Gensini score.
Results
Serum 8-OHdG, number of stenotic branches, and Gensini score were all significantly increased in the CHD group. After adjustment for various factors, the number of stenotic branches and Gensini score remained positively correlated with 8-OHdG levels in the CHD group. Coronary artery lesions were significantly more severe in the CHD compared with the non-CHD group when 8-OHdG levels were >0.523 ng/mL. The number of stenotic branches and Gensini score were significantly independently associated with 8-OHdG levels in patients with T2DM.
Conclusions
8-OHdG is a marker of oxidative DNA damage, and is highly associated with the extent of coronary artery lesions in ageing patients with T2DM.
Keywords
Introduction
Type 2 diabetes (T2DM) is a global public health problem with a rapidly increasing prevalence over the last 10 years. In addition, some factors associated with cardiovascular disease (CVD), including blood pressure and dyslipidemia, are also important factors in the progression of diabetes. Conversely, patients with T2DM show accelerated atherosclerosis and to have a higher prevalence of CVD.
Reactive oxygen species (ROS) are oxygen-containing molecules that can be cleared by antioxidant substances in normal situations. However, overexpression of ROS results in oxidative damage, of which oxidative DNA damage is the most injurious. The products generated by this process can be detected in blood and urine. 8-Hydroxy-2′-deoxyguanosine (8-OHdG) is the most abundant oxidative product, and reflects the degree of oxidative DNA damage. Given that excess ROS might play a role in CVD, high levels of 8-OHdG are considered to have a possible link to this disease. Moreover, previous studies showed that hyperglycemia independently increased 8-OHdG levels in patients with T2DM, and 8-OHdG was shown to be a novel biomarker of macrovascular complications in patients with T2DM. 1
In the current study, we investigated the possible contribution of 8-OHdG to the extent of coronary artery lesions in aging patients with T2DM, based on serum 8-OHdG levels measured by enzyme-linked immunosorbent assay (ELISA).
Methods
Subjects
Elderly patients with T2DM who were examined by coronarography at Ruijin Hospital or Ruijin Hospital North, Shanghai Jiaotong University School of Medicine, between December 2015 and June 2016, were included in the study. Other related data including history of past and current illnesses (hypertension, coronary heart disease, chronic heart failure, arrhythmia, cerebrovascular disease, and tumors) were collected. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured in all participants after resting for at least 5 minutes. We also measured biomarkers including 8-OHdG, fasting blood glucose (FBG), glycosylated hemoglobin (HbA1c), total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), blood urea nitrogen (BUN), creatinine (Cr), and uric acid (UA). Serum levels of 8-OHdG were measured by ELISA (Xinfan Biotechnology Co., Ltd, Shanghai, China). 2 The exclusion criteria were as follows: (1) type 1 diabetes, (2) severe diabetic complications such as ketoacidosis or coma, (3) chronic heart failure, (4) liver dysfunction, (5) chronic renal insufficiency or hemodialysis, and (6) cerebral infarction or cerebral hemorrhage. The flow chart of the study design is shown in Figure 1.

Flow chart of study design. SBP, systolic blood pressure; DBP, diastolic blood pressure; 8-OHdG, 8-hydroxy-2′-deoxyguanosine; FBG, fasting blood glucose; HbA1c, glycosylated hemoglobin, TC, total cholesterol; TG, triglycerides; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; BUN, blood urea nitrogen; Cr, creatinine; UA, uric acid.
All patients provided informed consent, and patient anonymity has been preserved.
Diagnostic standards
All patients were diagnosed with diabetes according to the American Diabetes Association Standards 3 and underwent coronarography. Patients were excluded if they had type 1 diabetes, diagnosed according to the World Health Organization Expert Committee on Diabetes Mellitus in 1999. 4 The definition of chronic renal insufficiency was based on the National Kidney Foundation Kidney Disease Outcomes Quality Initiative (NKF-KDOQI) in 2002 and endorsed by the Kidney Disease: Improving Global Outcomes (KDIGO) in 2004, using an estimated glomerular filtration rate <15 mL/minute per 1.73 m2 (stage 5).5,6 Patients with obstructive coronary disease defined as ≥50% stenosis of coronary vessels on coronarography were included. 7 The extent of the lesion in CHD was evaluated as described previously. 8 The final score for each patient was the sum of all the affected branches. 9
Statistical analysis
The results were analyzed using SPSS Statistics for Windows, version 20.0 (SPSS Inc., Chicago, IL, USA) and Prism 6.0 software (GraphPad Software Inc., CA, USA). Data are shown as mean ± standard deviation. Non-CHD and CHD groups were compared using two-tailed t-tests, and different groups of 8-OHdG were compared by one-way ANOVA. The relationships among 8-OHdG, the number of stenotic branches, and Gensini scores were evaluated using Pearson’s analysis, partial correlation analysis (adjusted mode), and multiple regression analyses. P values < 0.05 were considered significant.
Ethics approval and consent to participate
The included subjects gave informed consent, and patient anonymity has been preserved.
Results
General information
A total of 147 patients with T2DM were included in the study, including 91 men (61.9%) and 56 women (38.1%), mean age 73.29 ± 8.19 years (range 64–92 years). The patients were divided into a non-CHD group (n = 84) and a CHD group (n = 63). SBP and DBP were both significantly higher in the CHD group (both P < 0.001). 8-OHdG levels, the number of stenotic branches, and Gensini scores were also significantly higher in the CHD group (all P < 0.001). However, there were no differences in the levels of TC, TG, LDL-C, and Cr between the two groups (Table 1).
General information.

CHD, coronary heart disease; 8-OHdG, 8-hydroxy-2′-deoxyguanosine; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, fasting blood glucose; FBG, 2-h postprandial blood glucose; HbA1c, glycosylated hemoglobin; TG, triglycerides; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; BUN, blood urea nitrogen; Cr, creatinine; UA, uric acid.
Relationship between extent of coronary artery lesions and 8-OHdG
The patients were classified into four groups based on the interquartile values of 8-OHdG. The number of stenotic branches and Gensini scores increased significantly in line with increasing 8-OHdG (Table 2). Moreover, the extent of coronary artery lesions was more severe in the CHD group than in the non-CHD group when the level of 8-OHdG was >0.523 ng/mL (Figure 2a and 2b).
Extent of coronary artery lesions in relation to 8-hydroxy-2′-deoxyguanosine levels.

8-OHdG, 8-hydroxy-2′-deoxyguanosine.
aCompared with group 1 (8-OHdG ≤0.215 ng/mL), P<0.001; bcompared with 8-OHdG ≤0.215 ng/mL group, P<0.05; ccompared with group 2 (8-OHdG 0.215–0.294 ng/mL), P<0.001; dcompared with group 3 (8-OHdG 0.294–0.523 ng/mL), P<0.001.
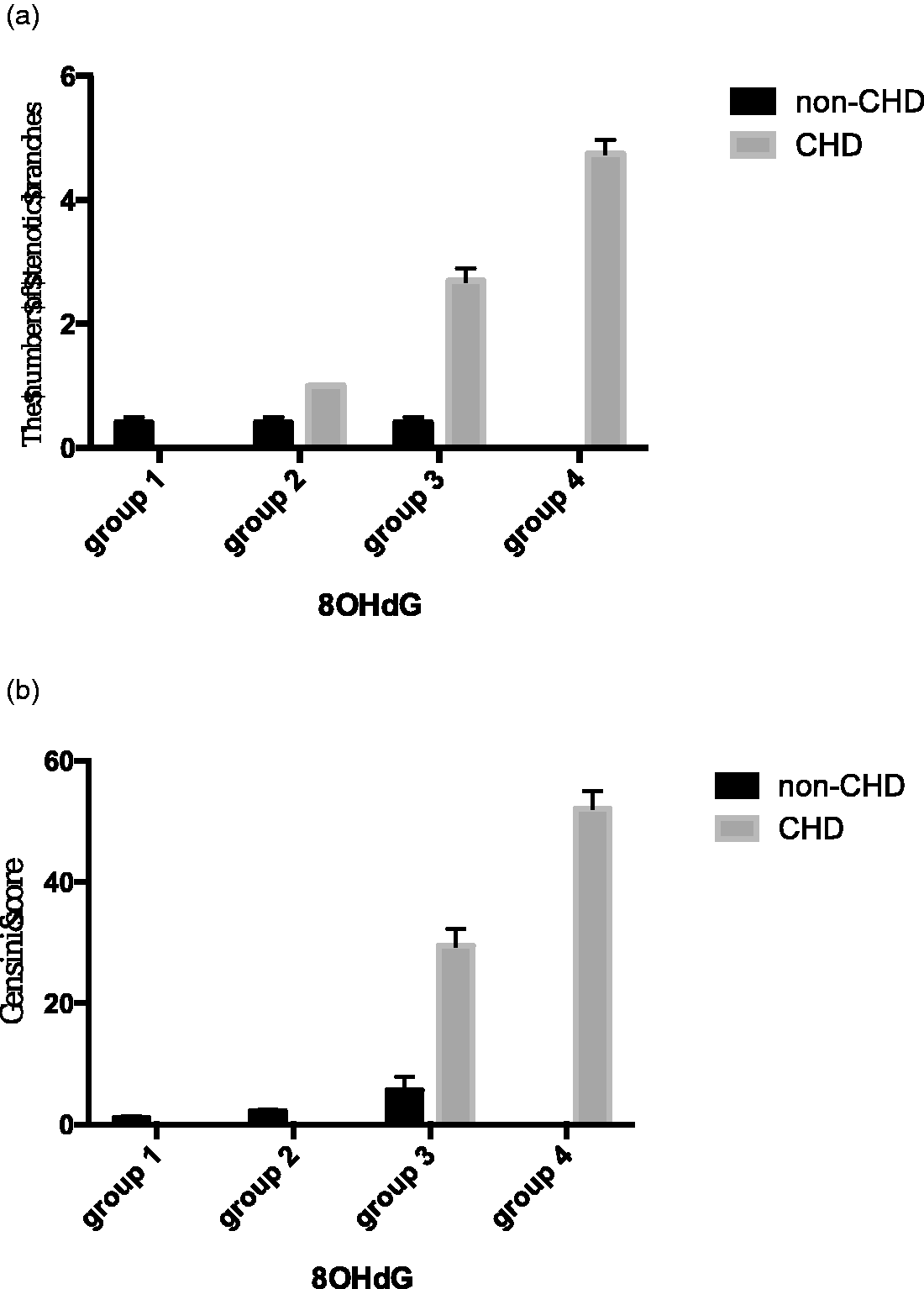
Relationship between the extent of coronary artery lesions and 8-hydroxy-2′-deoxyguanosine (8-OHdG). (a,b) There was no significant difference in the number of stenotic branches or Gensini score among the four groups according to 8-OHdG levels in the non-coronary heart disease (CHD) group. However, there were significant differences in the number of stenotic branches between groups 1 and 3 (P < 0.0001), groups 1 and 4 (P < 0.0001), groups 2 and 4 (P < 0.005), and groups 3 and 4 (P < 0.0001) in the CHD group. There were also significant differences in Gensini scores between groups 1 and 4 (P < 0.005), groups 2 and 4 (P < 0.005), and groups 3 and 4 (P < 0.0001).
Correlations between number of stenotic branches, Gensini score, and 8-OHdG
The number of stenotic branches and Gensini score were significantly positively correlated with the level of 8-OHdG in the non-CHD (P = 0.027 and < 0.001, respectively) and CHD groups (both P < 0.001). After adjusting for sex, SBP, DBP, FBG, HbA1c, HDL, BUN and UA, these correlations remained significant in both groups (P = 0.002 and < 0.001, and both P < 0.001, respectively) (Table 3). The number of stenotic branches and Gensini score showed more positive relationships with 8-OHdG level in the CHD group (Table 3). Multiple regression analyses were conducted using 8-OHdG level as a dependent variable, and potential risk factors including the number of stenotic branches, Gensini score, sex, SBP, DBP, FBG, HbA1c, HDL, BUN, and UA as independent variables. The number of stenotic branches (odds ratio (OR) 0.269, 95% confidence interval (95%CI) 0.076–0.954, P = 0.042) and Gensini score (OR 0.879, 95%CI 0.782–0.988, P = 0.031) were independently associated with 8-OHdG level in elderly patients with T2DM.
Correlation between 8-hydroxy-2′-deoxyguanosine and number of stenotic branches of coronary arteries and Gensini scores (r value).

*Adjusted for sex, systolic blood pressure, diastolic blood pressure, fasting blood glucose, glycosylated hemoglobin, high-density lipoprotein cholesterol, blood urea nitrogen, and uric acid. CHD, coronary heart disease; 8-OHdG, 8-hydroxy-2′-deoxyguanosine.
Discussion
T2DM has become a worldwide disease and a leading cause of mortality in recent decades. The prevalence of T2DM in China continues to increase, and Xu et al. 10 demonstrated an overall prevalence of diabetes of 11.6% (12.1% in men and 11.0% in women) in a representative sample of Chinese adults.
Many epidemiological studies have observed an increased risk of CVD in patients with T2DM. Hyperglycemia, diabetic dyslipidemia, and chronic sub-clinical inflammation have been thought to accelerate vascular injury and contribute to the prevalence of CVD in T2DM. A balance exists between antioxidant systems and potentially dangerous levels of oxidants controlled by scavenging of ROS. 8-OHdG is a product and marker of oxidative DNA damage, and several case-control studies have demonstrated significant positive associations between 8-OHdG and CVD. Jaruga et al. 11 demonstrated significantly greater concentrations of 8-OHdG in the urine of patients with atherosclerosis compared with healthy individuals. Xiang et al. 12 also confirmed that serum 8-OHdG was independently associated with the presence of coronary artery disease (OR, 1.318; P = 0.027). Moreover, 8-OHdG levels increased in line with the number of diseased vessels (P = 0.002) and were significantly correlated with Gensini score (r = 0.379, P = 0.001). 12 One prospective study 13 determined the incidence of major adverse cardiovascular events (MACE) in 237 patients with coronary stenosis during a median follow-up of 7.8 years, and found that baseline plasma levels of 8-OHdG tended to be higher in patients with MACEs than in those without MACEs, though the difference was not significant. In addition, 8-OHdG levels were elevated in T2DM patients with microvascular and macrovascular complications. 1 However, few studies 12 have used an international quantitative standard to evaluate the degree of coronary artery lesions in this population.
In the present study, we found substantial increases in blood pressure (SBP and DBP) and hyperglycemia (FBG and HbA1c) in the CHD group, but no significant difference in dyslipidemia between the non-CHD and CHD groups. In addition to these common factors in the progression of diabetes, our study also revealed high levels of 8-OHdG, more stenotic branches, and higher Gensini scores in the CHD group, suggesting that poor glycemic control led to increased oxidative stress, which in turn contributed to CVD in T2DM by damaging arterial walls.
We further investigated how serum levels of 8-OHdG affected the extent of coronary artery lesions, and found that serum 8-OHdG influenced both the number of stenotic branches and the Gensini score. Coronary artery lesions in T2DM include multivascular lesions, diffuse lesions, and a high degree of stenosis. Gensini score can thus better reflect the extent of the lesions, and showed a more positive relationship with 8-OHdG compared with number of stenotic branches (OR 0.879, 95%CI 0.782–0.988, P = 0.031). In addition, T2DM tended to have a higher chance of being accompanied by CHD in patients with a serum level of 8-OHdG >0.523 ng/mL.
Our study had some limitations. First, we did not address the mechanisms involved in the observed relationships, and further studies with animal models are needed to investigate these possible mechanisms. Second, the sample size was relatively small, and we did not consider the effects of any drugs used by the participants during the study. We therefore cannot exclude any possible effects of different drug treatments. Finally, further longitudinal studies are needed to confirm our current conclusions.
Conclusions
The results of the current study showed that elevated 8-OHdG levels reflected increased oxidative DNA damage in ageing patients with both T2DM and CHD. This study further confirms the value of 8-OHdG as a potential predictor of CHD in elderly patients with T2DM.
Footnotes
Availability of data and material
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Medical and Science Crossover Research Fund of Shanghai Jiaotong University (YG2014MS55) and Shanghai Municipal Health Bureau (16CR4013A).