
Abstract
Objective
To compare the effect of two prophylactic euvolemic fluid strategy regimens on the incidence of cerebral vasospasm and clinical outcomes in patients with aneurysmal subarachnoid hemorrhage (SAH).
Methods
Ninety-six patients with a basal intravenous intake of 15 mL/kg/day of Ringer’s lactate solution were included, and an additional 15 to 50 mL/kg/day Ringer’s lactate (RL-group) or hydroxyethyl starch 130/0.4 solution (HES-group) was administered to maintain the targeted mean arterial pressure. The primary end point was the occurrence of cerebral vasospasm during the first 14 days. The secondary end points were case fatality, Barthel’s index, and Glasgow Outcome Scores (GOS) at 30 days after SAH.
Results
Cerebral vasospasm developed in 42 patients (43.7%), and nine of these events were severe. The vasospasm rate among the RL- and HES-based groups was 25/48 and 17/48, respectively. For the secondary endpoint, four patients (4%) died by the end of follow-up (two in each group). Unfavorable outcome cases were not different in the RL and HES groups (9 vs. 14, respectively). There was no difference between the Barthel’s scores at 30 days between the two groups.
Conclusions
Using starches in a prophylactic treatment strategy in aneurysmal SAH in not supported by the study.
The trial was registered at Clinicaltrials.gov under the number NCT02064075
Keywords
Background
Despite the advancement of new management strategies, ischemic neurological deficit secondary to cerebral vasospasm remains a leading cause of unfavorable outcome (death or dependency) in patients with aneurysmal subarachnoid hemorrhage (SAH). 1 , 2 Intravascular volume dysregulation and consequent hypovolemia has been observed after SAH 3 , 4 and it has been also demonstrated that hypovolemia and volume restriction are important risk factors in the development of vasospasm and delayed ischemic neurologic deficit (DIND). 5 Previous case control studies from the 1980s indicated that volume expansion aiming to increase cerebral blood flow may help to prevent DIND.6–8 This led to the concept of triple-H therapy (hypertension–hypervolemia–hemodilution) that has been in use for more than two decades. 9 , 10 However, this concept has been challenged because positive fluid balance was associated with poor outcomes in some studies 11 , 12 or it did not result in an improved clinical outcome. 13 , 14 Recent guidelines favor maintaining euvolemic fluid status and avoiding hyper- and hypovolemia. Additionally, the increase in mean arterial pressure (MAP) is proposed as the most important element of triple-H therapy. 15 In everyday practice, target blood pressure is reached by a combination of fluid and vasopressor administration. Currently, crystalloids rather than colloids are the preferred solutions for fluid replacement based on the recommendations, but because there is a lack of large, prospective randomized trials, there is little evidence to support this recommendation.
In the present study, we aimed to compare the effect of two prophylactic euvolemic fluid strategy regimens on the incidence of cerebral vasospasm and on the clinical outcome in patients with aneurysmal SAH. This is a single center, blinded, randomized study comparing the effect of Ringer’s lactate and hydroxyethyl starch (HES)-based fluid strategies.
Patients and methods
Between February 2014 and March 2015, a prospective, randomized, blinded, controlled trial was conducted in patients who were admitted to the Neurosurgical Intensive Care Unit (ICU) in the Department of Anesthesiology and Intensive Care and the Department of Neurosurgery University of Debrecen, Faculty of Medicine with the diagnosis of non-traumatic spontaneous SAH. After permission from the local medical ethics committee, patients or their relatives provided written informed consent to participate in the study. The trial was registered at Clinicaltrials.gov under the number NCT02064075.
The diagnosis of aneurysmal SAH was based on clinical findings and computed tomography (CT) followed by cerebral angiography in all patients. On admission, SAH severity was evaluated using the Hunt and Hess and Fisher’s gradings. After the CT and cerebral angiography, a decision was made by the team consisting of neurosurgeons and neuroradiologist about the intervention (surgical clipping or coiling of the aneurysms). All patients received nimodipine (6 × 60 mg) and 40 mg/day simvastatin orally. The serum magnesium concentration was kept within the normal range by administering MgSO4 as was necessary based on laboratory results (target plasma concentration: 0.6–1.1 mmol/L). The exclusion criteria included patients who were not cooperative, refused to participate in the study, or died during screening and entry into the study.
Therapeutic regimen
Guidance of prophylactic fluid therapy was conducted between the admission day and day 7, and it was based on the MAP value measured at admission. An individual MAP was targeted, as follows: MAP at admission +30%, until a maximum of 200 mmHg systolic blood pressure. A basal fluid intake of 15 mL/kg/day Ringer’s lactate solution was administered intravenously in all patients. To reach the target MAP values, an additional amount of 15 to 50 mL/kg/day Ringer’s lactate (B. Braun, Melsungen AG, Germany) or HES 130/0.4 solution (Voluven, Fresenius-Kabi, Bad Homburg, Germany) was administered based on the randomization. In addition to fluid therapy, intravenous noradrenaline and/or dobutamine was administered to reach the required target blood pressure values. Normovolemic daily fluid balance was reached by adding furosemide and adjusting the noradrenaline dose as necessary. This prophylactic fluid strategy was administered between day 0 and day 7 in all patients.
Randomization and blinding, treatment allocation, and follow-up
Patients were randomly allocated into two groups to receive either additional Ringer’s lactate or HES after arrival at the ICU. To ensure that there were an equal number of patients in both groups, we used permuted block randomization. We labeled 48 cards with R and another 48 cards with V, and then we mixed them and put them into opaque envelopes. Four-item blocks were generated based on a random number generator followed by permuted block generation for all possible variations. During inclusion, the next labeled card among the arranged blocks was selected. An independent intensivist, who was not part of the follow-up investigations prepared the infusions. Follow-up neurological assessment and transcranial Doppler measurements were performed by experienced intensivists (BF, PS) who were blinded to the patients’ group. This was ensured by covering the infusion label during transcranial color-coded duplex (TCCD) sonography and neurologic assessments.
Evaluating vasospasm
All patients underwent routine monitoring in the ICU including continuous electrocardiogram (ECG), pulsoxymetry, intraarterial blood pressure measurement (radial artery). Neurological status was recorded twice daily by the ICU staff. TCCD sonography was performed daily using a 2-MHz sector probe from a Siemens Acuson Antares (Siemens Healthcare GmbH, Erlangen, Germany) ultrasound device. Cerebral vasospasm was defined when the mean blood flow velocity values exceeded 120 cm/s in the middle cerebral artery or in any other segments of the circle of Willis. Severe vasospasm was considered if the mean blood flow velocity was higher than 200 cm/s.
Outcome measures
Primary end point was defined as occurrence of cerebral vasospasm between days 1 to 14 after bleeding. Secondary end points were as follows: case fatality, Barthel’s index, and Glasgow Outcome Scores (GOS) at 30 days after SAH in the two groups.
Statistical analysis
Sample size estimation was based on previously published data, which showed that the incidence of cerebral vasospasm is approximately 30% after SAH. We anticipated that the occurrence of vasospasm would be decreased by 20% in the HES group compared with the RL-group. At an alpha of 0.05 and a power of 80%, 90 patients (45 in each group) were required to answer the study questions. Including potential dropouts, we decided to include 96 patients (three additional patients in each group).
Continuous variables are presented as the mean and standard deviation (SD). Categorical variables were compared using the chi-square test. Blood flow velocities in the middle cerebral artery during follow up were compared using a repeated measure ANOVA between the two groups with treatment allocation and time main effects. A p value of <0.05 was accepted as statistically significant. Dell Statistica 13.2 (Dell Inc., Aliso Viejo, CA, USA) was used for data analysis.
Results
There were 96 patients included in this study, with 48 patients in the RL-group and 48 patients in the HES-group. In the RL-group, the average age was 49.64±11.2 years, and 15 patients were men and 33 patients were women. In the HES-group, the average age was 51.23±10.34 years, and 20 patients were men and 28 patients were women (Table 1). Comorbidities, confounding factors, and clinical characteristics of the included patients are also summarized in Table 1. There were no significant differences between the groups for any of the initial parameters. Figure 1 summarizes the screening, inclusion, and exclusion criteria for the patients.
Characteristics and confounding factors of the two groups.

RL, Ringer’s lactate; HES, hydroxyethyl starch; ACI, internal carotid artery; MCA, middle cerebral artery; ACA, anterior cerebral artery; ACoP, posterior communicating artery; PCA, posterior cerebral artery; BA, basilar artery; CT, computed tomography; PICA, Posterior inferior cerebellar artery; NIH, National Institutes of Health; IQR, interquartile range; N.S., not significant.

Consort flow chart of patient screening and inclusion.
Primary end point: Development of cerebral vasospasm
Overall, cerebral vasospasm developed in 42 patients (43.7%). Among these 42 patients, 9 patients experienced severe (>200 cm/second mean blood flow velocity) cerebral vasospasm. The distribution of patients with cerebral vasospasm among the RL-based and HES-based groups was 25/48 (6 severe) compared with 17/48 (3 severe), respectively (chi-square: 3.41). Aneurysm could not be detected using digital subtraction angiography (DSA) angiography in 22 patients, among whom nine patients were in the RL-group and 13 patients were in the HES-based group (Table 1). Among the angiogram-negative group, vasospasm developed in two out of the 24 patients. Both of these patients were randomized to the HES group and the events were considered to be moderately severe (120 cm/s < middle cerebral artery mean blood flow velocity (MCAV) < 200 cm/s).
TCCD measurements were performed once daily between days 1 and 14. After 2 weeks, TCCD monitoring was continued only in patients where the previous TCCD results indicated cerebral vasospasm and continuation of monitoring was considered necessary by the staff. There were 19 patients in the RL-based group and 14 patients in the HES-based group who required further monitored using TCCD between days 14 and 20. The results of the TCCD measurements in the two groups are shown in Figure 2. Mean blood flow velocities in the middle cerebral artery showed a similar pattern in the RL-based and HES-based groups, but there was no statistically significant difference between the treatment groups (treatment allocation main effect, not significant; time main effect, p<0.001; treatment with time interaction, not significant).
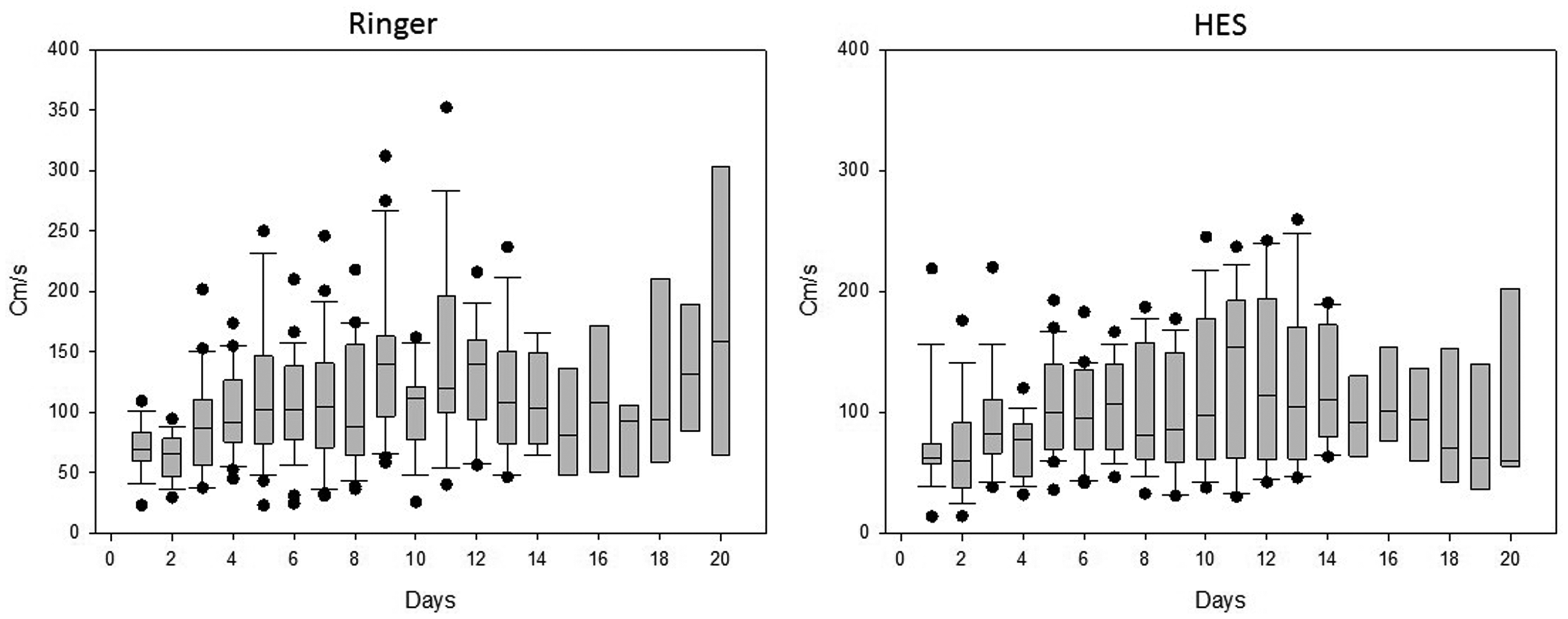
Middle cerebral artery mean blood flow velocities in the RL and in the HES based groups. The median and IQR, and the minimum and maximum values are presented.
Secondary end points
The overall case fatality at 30 days was four (4.1%). There was no fatal outcome among angiogram-negative patients in either the RL-based and the HES-based groups. All deaths occurred in the aneurysmal group, which included two patients in the RL-based group and two other patients in the HES-based group. Thus, case fatality was not influenced by the fluid strategy.
A GOS referring to unfavorable outcome (death, permanent vegetative state, and severe disability; GOS 1–3) was observed in nine patients (all aneurysmal) in the RL-based group and 14 patients (13 aneurysmal and one angiogram-negative) in the HES-based group. A favorable outcome (GOS 4–5, independent in daily living) was observed in 39 patients (29 aneurysmal and ten angiogram-negative patients) in the RL-group and 34 patients (21 aneurysmal and 13 angiogram-negative) in the HES-group. The differences in this outcome were not statistically significant (Chi-square = 1.43).
The distribution of the different Barthel’s scores in the RL and HES groups is summarized in Table 2. There were no differences between the distribution of patients with a different severity of the Barthel’s scores at 30 days between the two groups. This was also true for the aneurysmal cases after leaving out the data from the angiogram-negative patients.
Barthel’s index at day 30 in the Ringer’s and HES groups.

Data in parenthesis indicate angiogram-positive cases.
HES, hydroxyethyl starch; N.S, not significant.
Catecholamine (norepinephrine) administration was necessary in ten patients in the RL-group and nine patients in the HES-group.
Discussion
In the present study, we administered prophylactic fluid therapy to reach a targeted mean blood pressure with the intention to prevent cerebral vasospasm and improve outcome in patients with SAH. Two fluid strategies were compared (crystalloid [RL]-based and HES-based) and no differences were shown in any of the study end points (occurrence of vasospasm, outcomes at 30 days after onset). To the best of our knowledge, this is the first prospective, randomized, double-blind trial that compared the prophylactic efficacy of Ringer’s lactate and HES 130/0.4 in patients with SAH.
The European Medicines Agency proposed to restrict the use of HES in critically ill septic patients because of a reported increase of renal failure compared with crystalloid solutions. 16 Whether this proposal also applies to patients with aneurysmal SAH remains controversial. In a recent study, Ibrahim and Macdonald 17 conducted a post-hoc analysis of the CONSCIOUS-1 trial and compared the outcome of colloid-based and crystalloid-based groups in patients with aneurysmal SAH. That study focused on the efficacy clazosentan and the fluid strategy was left to the discretion of the treating physician. In that study, 41 patients received colloids (either for treatment or for prophylactic purposes). There was no difference between the colloid and non-colloid groups in terms of delayed ischemic neurological deficits, GOS, and Rankin scores. A similar result was found by Lennihan et al. 18 who administered albumin as colloid therapy and found that there was no benefit of prophylactic hypervolemic fluid therapy. In a similar study, Egge et al. 19 found no benefit of hypervolemic hypertensive hemodilution therapy (using albumin and rheomacrodex) compared with normovolemic strategy in terms of vasospasm occurrence and clinical outcomes. In a retrospective analysis comparing HES- and crystalloid-based prophylactic fluid strategies, no differences were found between in-hospital mortality and GOS in the two groups, although the incidence of vasospasm and the ICU length of stay was greater in the HES-group compared with the crystalloid-based group. 20 In a prophylactic hypervolemic study using 5% albumin, the incidence of symptomatic cerebral vasospasm was identical in the normovolemic and hypervolemic groups, and there was no difference in GOS at 30 days in the two groups.
It is hard to compare our results with these previous studies because of their different concepts. The use of colloids for prophylactic purposes was based upon the concept that they may have advantageous hemorheological effects and may improve cardiac output, with an increase in cerebral blood flow 21 before a severe vasospasm develops. However, later studies showed that hypervolemia may be as detrimental for patients with SAH as hypovolemia and a positive fluid balance is associated with a worse outcome. 17 Consistent with this, based on the recent recommendations, volume management should target euvolemia and avoid prophylactic hypervolemic therapy. 15 In accordance with the weak recommendation of this consensus document, in the present randomized trial, we showed that the use of colloids for euvolemic prophylactic therapy has no advantage over crystalloid therapy for vasospasm occurrence and clinical outcome. Although the rate of cerebral vasospasm was 30% lower in the HES-group compared with the RL-group, clinical outcomes at 1 month after the onset of SAH did not suggest even a mild tendency for a benefit of HES. However, for vasospasm, a large trial may provide a final conclusion, such a trial is not justified because there was not even a small signal for a possible benefit of HES.
There were some limitations in our study. First, the fluid strategy was based upon invasive blood pressure measurements and daily fluid balance data and no other hemodynamic monitoring (pulse induced contour cardiac output [PiCCo] or central venous pressure monitoring) 22 was used. This might have resulted in inequalities in the fluid status during certain periods of the day, but euvolemia was maintained based on the fluid balance data in all patients. Second, the prophylactic fluid strategy was started on the day of admission and lasted for 7 days per protocol. This may be considered to be a short time for prophylaxis, but the decision was made to cover the most probable period of vasospasm development. In those patients in whom cerebral vasospasm developed, targeted blood pressure therapy was also maintained for the later period of treatment. Another important limitation is that the definition of the vasospasm in the present study was based on transcranial Doppler measurements. The most common definition of vasospasm in the literature includes a blood pressure dependent new neurological deficit with/or increased velocity in TCCD in sedated patients on CT- or conventional angiography with/or perfusion imaging. These additional diagnostic methods were only used if blood flow velocities increased and the neurological status of the patients deteriorated despite increasing the blood pressure.
Conclusion
In this single center, randomized, double-blind trial, we found no difference between the outcome parameters of crystalloid and HES-based prophylactic euvolemic fluid strategies in patients with aneurysmal SAH. The results of the present study do not support the use of starches in the prophylactic treatment strategy in SAH patients.
Abbreviations
RL, lactated Ringer’s solution
HES, hydroxyethyl starch
GOS, Glasgow outcome score
ICU, intensive care unit
SAH, subarachnoid hemorrhage
DIND, delayed ischemic neurologic deficit
MAP, mean arterial pressure
CT, computer-assisted tomography
TCCD, transcranial color-coded duplex sonography
Footnotes
Authors’ contributions
JG, DV, BF, EF: patient follow-up, data handling, and drafted the manuscript; PS: transcranial Doppler measurements; BF: study concept, transcranial Doppler measurements, and drafted the manuscript; DB, MCs: manuscript concept, statistical analysis, and drafted the manuscript; SSz: study concept and drafted the manuscript.
Availability of data and material
Data will be available upon request from the corresponding author.
Consent for publication
All authors read and approved the manuscript
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics approval and consent to participate
The study was performed after obtaining permission from the medical ethics committee of the UNIVERSITY OF DEBRECEN (DEOEC RKEB/IKEB Prot. No. 3799 -2012), and the patients or their relatives gave written informed consent to participate in the study. The trial was registered at Clinicaltrials.gov under the number NCT02064075.
Funding
The work was supported by the Hungarian Brain Research Program (Grant number 2017-1.2.1-NKP-2017-00002).