
Abstract
Objectives
Suicide is closely related to sociological factors, but sociological analyses of suicide risk in leukemia are lacking. This study is the first to use the Surveillance, Epidemiology, and End Results Program (SEER) database to analyze sociological risk factors for suicide death in leukemia patients.
Methods
A retrospective search of the SEER database was conducted. Logistic regression was used to identify independent risk factors for suicide death. Variables significant in the univariate logistic regression models were subsequently analyzed using multivariate regression.
Results
The death rate was highest in California (1.73%). Suicide mortality was more common during the 1970s and 1980s, after which it trended downward. Young age at diagnosis (18–34 vs. >64 years: odds ratio [OR] = 1.537, 95% confidence interval [CI] = 1.007–2.347; 35–64 vs. >64 years: OR = 1.610, 95% CI = 1.309–1.979), being male (OR = 1.518, 95% CI = 1.230–1.873), and living where a high proportion of people have at least a bachelor’s degree (>50% vs. <20%: OR = 8.115, 95% CI = 5.053–13.034) significantly increased suicide death risk.
Conclusion
Our findings could increase clinician awareness of and appropriate support for leukemia patients at risk of death by suicide.
Keywords
Introduction
Death by suicide is a global problem that can occur throughout the life span and represents a serious healthcare burden. 1 Globally, almost 800,000 people die each year from suicide (one death every 40 seconds), accounting for 1.5% of deaths worldwide. 2 The healthcare burden is even greater when suicidal ideation and attempted suicide are included. 3
Cancer poses a major threat to human life, and being diagnosed with cancer is associated with increased risks of suicidal ideation and attempted suicide. 4 The suicide rate is reportedly almost twice as high in cancer patients as in the general population.5,6 In addition, about 70% of suicide deaths among patients older than 60 years are related to medical conditions, and the incidence is particularly high in cancer patients.7–12 Anxiety, comorbidities (e.g. depression, patient stress, high levels of hopelessness13–15), psychosocial conditions and decreased quality of life owing to adverse drug reactions are the leading causes of suicide in cancer patients.
Increasing attention is being paid to sociological factors associated with suicide, and research on the association between cancer and sociological factors is growing. Caleyachetty et al. 16 found that exposure to a greater number of social risk factors increases the risk of death from all cancers combined, tobacco-related cancers and lung cancer in US adults. Another study found that women who had been socially isolated before diagnosis had a 66% increased risk of subsequent all-cause mortality and a triple risk of breast cancer mortality compared with socially integrated women. 17
Leukemia constitutes a group of life-threatening blood and bone marrow malignancies. 18 Leukemia cells proliferate and accumulate in bone marrow and other hematopoietic tissues owing to uncontrolled proliferation, differentiation disorders and blocked apoptosis, and infiltrate other non-hematopoietic tissues and organs, while inhibiting normal hematopoietic function.
The Surveillance, Epidemiology, and End Results Program (SEER) database includes 18 registries that cover 30% of the US population and records demographic, clinical and outcome information for all cancers diagnosed in representative geographic regions of the USA.19,20 It is therefore a potentially useful resource for identifying suicide deaths. The sociological risk factors examined in this study mainly relate to social environment, economics, education and other factors, rather than tumor size and stage, which are more clinically focused factors. Death by suicide is closely related to sociological factors (e.g. psychological, family, social life, interpersonal relationships and spiritual factors), but there are no previous sociological analyses of suicide risk in leukemia. Therefore, this study is the first to use the SEER database to analyze sociological risk factors for suicide death in leukemia patients.
Methods
Patients
A retrospective search of the SEER database was performed for cases diagnosed between 1973 and 2015; the database was accessed using SEER*Stat software (Surveillance Research Program, National Cancer Institute SEER*Stat software (seer.cancer.gov/seerstat) version 8.3.4). We searched the SEER database for records using International Classification of Diseases for Oncology (ICD-O-3) codes. We searched for patients older than 18 years, and excluded cases with no diagnosis, microscopic confirmation, autopsy findings only, or incomplete variables.
The use of data from the SEER database does not require informed patient consent because all of these publicly available data are anonymized and de-identified prior to release. The SEER database can be accessed free of charge, and this study was exempted from obtaining informed consent by the institutional research committee of the First Affiliated Hospital of Xi’an Jiaotong University.
Statistical analysis
Patients were divided into the following two groups: suicide death and other causes of death. Logistic regression was used to identify independent risk factors for death by suicide. Variables that were statistically significant in the univariate logistic regression models were subsequently also analyzed using multivariate logistic regression models. All statistical tests were two-sided, with P < 0.05 considered to indicate statistical significance. All statistical analyses were performed using SPSS version 24.0 (IBM Corp., Chicago, IL, USA) and R (version 3.5.0) software (www.r-project.org).
Results
Patient characteristics
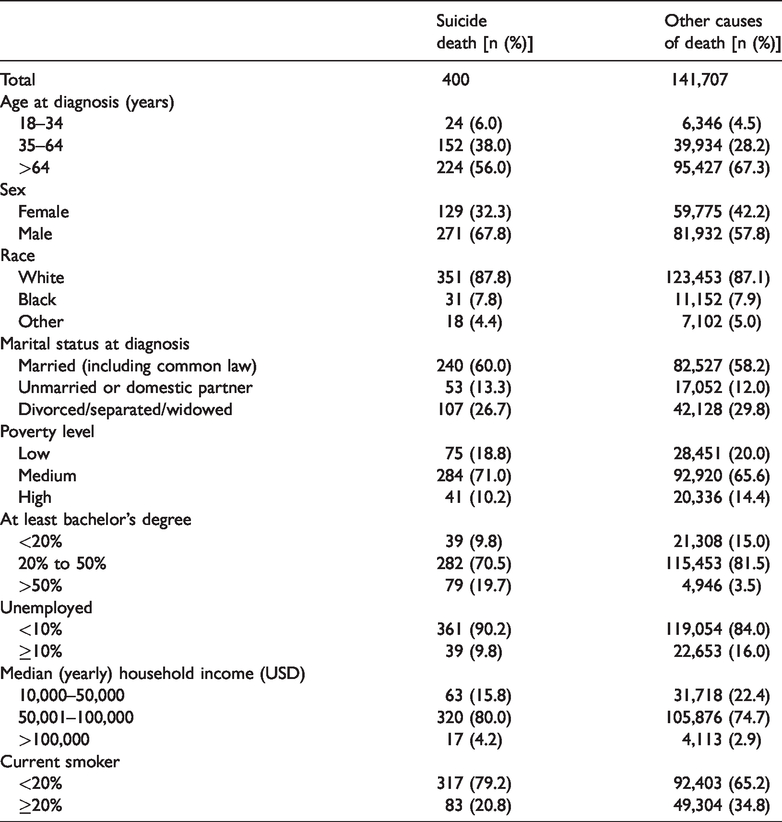
The application of our selection criteria identified 142,107 eligible patients, of whom 400 died by suicide. Most patients in the present cohort were aged >64 years, male, white and married. There were more suicide deaths in the groups living at a medium poverty level (71.0%), that comprised 20% to 50% of residents with at least a bachelor’s degree, had <10% who were unemployed, had a median household income of USD 50,001–100,000, and comprised <20% current smokers. The baseline demographics for the two groups are shown in Table 1.
Characteristics of patients.
Differences in suicide mortality rates by decade and state
The death rate from suicide was highest in California, at 1.73‰, followed by Washington, Michigan, and Georgia, at 0.22‰, 0.15‰ and 0.14‰, respectively. Suicide mortality was more common during the 1970s and 1980s, after which it trended downward (Figure 1).

Differences in rate of suicide mortality by decade.
Risk factors for suicide death
Univariate logistic regression showed that age at diagnosis, sex, having at least a bachelor’s degree, being unemployed, median household income and current smoking status were significant contributors to the risk of death by suicide (all P < 0.05). We included these factors in the multivariate logistic regression, which showed that age at diagnosis (18–34 vs. >64 years: odds ratio [OR] = 1.537, 95% confidence interval [CI] = 1.007–2.347, P = 0.046; 35–64 vs. >64 years: OR = 1.610, 95% CI = 1.309–1.979, P < 0.001), sex (male vs. female: OR = 1.518, 95% CI = 1.230–1.873, P < 0.001), and the proportion of residents having at least a bachelor’s degree (>50% vs. <20%: OR = 8.115, 95% CI = 5.053–13.034, P < 0.001) significantly affected the risk of suicide death. Having a higher median household income (>USD 100,000 vs. USD 10,000–50,000: OR = 0.294, 95% CI = 0.152–0.567, P < 0.001) and being a current smoker (≥20% vs. <20%: OR = 0.564, 95% CI = 0.409–0.778, P < 0.001) seemed to exert protective effects (Table 2).
Univariate and multivariate logistic regression analysis results.

OR: odds ratio; CI: confidence interval.
Stratified analysis of different current smoker groups
We conducted a stratified analysis of current smokers. In the group of people that comprised <20% current smokers, being younger at the time of diagnosis (18–34 vs. >64 years: OR = 1.656, 95% CI = 1.051–2.610, P = 0.030; 35–64 vs. >64 years: OR = 1.633, 95% CI = 1.294–2.061, P < 0.001) and having at least a bachelor’s degree (>50% vs. <20%: OR = 8.612, 95% CI = 3.017–24.580, P < 0.001) significantly increased the risk of suicide death. Having a higher median household income (>USD 100,000 vs. USD 10,000–50,000: OR = 0.290, 95% CI = 0.115–0.733, P = 0.009) was a protective factor. In the group of people comprising ≥20% current smokers, being younger at diagnosis (35–64 vs. >64 years: OR = 1.628, 95% CI = 1.028–2.579, P = 0.038) and being male (vs. female: OR = 4.508, 95% CI = 2.399–8.471, P < 0.001) significantly increased the risk of suicide death, whereas being black (vs. white: OR = 0.271, 95% CI = 0.083–0.884, P = 0.030) was a protective factor (Table 3).
Multivariate logistic regression analysis results for current smoker groups.

OR: odds ratio; CI: confidence interval.
Discussion
This study is the first to use the SEER database to analyze the sociological risk factors for suicide death in leukemia patients from 1973 to 2015. We found that younger age at time of diagnosis, being male and living where a higher proportion of people have at least a bachelor’s degree significantly increased the risk of suicide death.
Death by suicide is a major public health problem. 6 Suicidal ideation can be triggered by genetic, psychological or neurobiological factors, and some cancer patients—especially those in an advanced stage—have a strong wish to die.21–23 Kam et al. 24 found that the incidence of suicide was more than three times as high in patients with head and neck cancer compared with the general US population. Klaassen et al. 25 found that suicide in patients with genitourinary malignancies poses a public health problem, especially among males, older people and those with aggressive disease. Bowden et al. 7 found that being female, white and aged ≤39 years or 70 to 79 years were factors strongly associated with an increased risk of suicide in patients with gastric cancer. However, there are few reports on the association between leukemia and suicide risk. This is the first study to use the SEER database to analyze the sociological risk factors for suicide death in leukemia patients. The findings indicate that being younger at diagnosis, being male, and having at least a bachelor’s degree significantly increased the risk of suicide death.
Age has always been a risk factor for death by suicide, and patients of different ages exhibit different psychological responses during treatment. 26 One study of medical students, house staff and faculty physicians showed that younger patients are more likely to have anxiety than older patients. 27 We found that age at diagnosis was a risk factor for death by suicide among leukemia patients. This suggests that young patients should receive cancer-related psychological education as soon as possible, and they should communicate with their family and medical workers to avoid excessive psychological stress levels.
We also found that sex was a risk factor for suicide. Being male conferred an increased suicide death risk, which is consistent with the finding that males in the general population are more likely to die by suicide. 28 Another study showed that suicidal ideation was significantly more common in males. 29 Healthcare professionals should pay more attention to communicating with male patients to help them avoid death by suicide caused by factors such as excessive psychological stress, fear of the reactions of parents and friends, and fear of social discrimination. 5
One of our most interesting findings was that highly educated patients (those with at least a bachelor’s degree) are significantly more likely to die from suicide. Levels of psychological distress are increasing among students in higher education institutions. 30 Suicidal behavior in college students is related to various factors, such as psychopathology, stressful life events and personality traits, 31 and the rapid growth of higher education and the high expectations students must meet have increased the amount of psychological pressure that they experience. 32 The number of years of potential life lost by suicide death and the associated socioeconomic burden are enormous.33–35 It is clear that there is a need to investigate these apparent effects of academic qualifications to develop effective prevention strategies in this population.
The death rate from suicide was highest in California, followed by Washington, Michigan, and Georgia. This may be because these states, particularly California, have a more developed economy, higher living standards, higher levels of education and higher levels of psychological stress.
We found that being a current smoker seemed to have a protective effect. We conducted a stratified analysis after dividing smokers into two groups according to their proportion. Age at diagnosis remained a risk factor for suicide death. The risk of suicide death was significantly higher in the group comprising <20% current smokers, in that having at least a bachelor’s degree (>50% vs. <20%), and in the group comprising ≥20% current smokers who were male.
The World Health Organization has shown that suicide is now the fourth most important health problem after cerebrovascular disease, chronic obstructive pulmonary disease and severe depression, and so is an important issue that affects public health, family happiness and social harmony. 36 Suicide in hospitalized patients also causes serious harm and is a source of substantial psychological stress for medical staff. 37 Improving hospital safety, security and management; outpatient monitoring; and training medical staff in patient suicide assessments and prevention are particularly important for preventing suicide among leukemia patients.
There were several study limitations: (1) the retrospective design is an inherent limitation, (2) we were unable to obtain SEER data on various potentially important factors such as anxiety, depression and pain, (3) the cause of death recorded in the database may have been biased by misclassification, (4) these results do not include individuals who attempt suicide, (5) some of the individuals with leukemia also had secondary cancers or metastatic cancers. Emotional distress may be cumulative and so may be strongly related to suicide, and (6) these findings likely cannot be generalized to minority populations, as the sample comprises predominately older, Caucasian males.
Conclusion
We found that younger age at diagnosis, being male and having at least a bachelor’s degree significantly increased the risk of suicide death. It is crucial to identify and treat people at risk of death by suicide as early as possible. More attention should be paid to sociological risk factors. Clinicians, caregivers and family members should be more aware of suicidal tendency in leukemia patients to provide timely treatment and psychological counselling.