
Abstract
Objective
To investigate the value of ultrasound in the dynamic assessment of lung injury after acute paraquat poisoning.
Methods
A prospective observational study was performed on patients with paraquat poisoning from admission to day 28 or discharge. Ultrasound assessment of the lungs was performtyed every 48 hours. The correlation of the lung ultrasound score (LUS) with other indicators was analyzed.
Results
Twenty-six patients were enrolled, with an average age of 46 ± 16 years. The average toxic dose was 95 ± 51 mL. The intensive care unit (ICU) stay averaged 9 ± 8 days, and the 28-day mortality was 88.5%. There was a significant negative correlation between LUS and oxygenation index (rho = −0.896) and a significant positive correlation between LUS and carbon dioxide concentration (rho = 0.567). Lung ultrasound and computed tomography imaging correlated closely.
Conclusion
Lung ultrasound can reflect changes in lung status in patients with paraquat poisoning and can be used to evaluate lung injury in these patients.
Introduction
Paraquat poisoning is an important public health problem because of its high mortality rate; it has been an area of focus in the international community, especially in developing countries. 1 Regardless of whether the poisoning is acute or chronic, lung injury is obvious, characterized by pulmonary fibrosis. The main cause of death in patients is multiple organ dysfunction syndrome/multiple organ failure (MODS/MOF). 2 Therefore, assessment of lung injury in patients with paraquat poisoning is important to guide treatment. Lung ultrasound has proven its value in trauma, acute respiratory distress syndrome (ARDS), pneumonia, and many other diseases. 3 We evaluated the use of ultrasound and lung ultrasound score (LUS) to assess lung injury in patients with paraquat poisoning.
Patients and methods
Patients
This study was a prospective observational study approved by the Ethics Committee of The First Affiliated Hospital of Jiaxing University (approval number: 2015-020), and written informed consent was obtained from all participants. Patients poisoned by paraquat who were admitted to the ICU of the First Affiliated Hospital of Jiaxing University from June 2015 to December 2017 were selected.
The inclusion criteria were (1) ≥18 years old; and (2) acute poisoning by paraquat, with time since exposure <24 hours. The exclusion criteria were (1) hemothorax or pneumothorax without drainage; (2) pulmonary artery wedge pressure >18 mmHg or central venous pressure (CVP) >15 mmHg; (3) pulmonary space-occupying lesions affecting ultrasound observers; (4) hospital stay time <48 hours. Twenty-six patients were included, including 13 men and 13 women aged from 18 to 72 years.
Patient treatment
All patients were diagnosed according to medical history and the urine paraquat sodium bicarbonate-sodium dithionite rapid test, followed by the Taishan Consensus for routine treatment, 4 including hemoadsorption for 6 hours immediately after ICU admission (HA130, Zhuhai Jianfan Biotechnology Co. Ltd., Shenzhen, China). If the partial pressure of O2 (ppO2) was <60 mmHg, noninvasive or invasive assisted ventilation was administered (only pressure support, no increase in oxygen concentration). When the ppO2 was <40 mmHg, we gradually increased the concentration of inhaled oxygen and maintained the ppO2 >40 mmHg. Continuous renal replacement therapy (CRRT) was administered in the presence of persistently elevated renal function or if there was no urine. All patients were routinely monitored for heart rate using the Philips MP60 multifunction monitor (Royal Philips, Eindhoven, the Netherlands), in addition to oxygen saturation, noninvasive/invasive blood pressure, and continuous central venous pressure. Arterial blood gas levels were measured synchronously every time the patient underwent pulmonary ultrasound examination. Daily routine assessments of liver and kidney function (serum creatinine, sCr), complete blood count, coagulation function, and inflammation index (C-reactive protein, CRP) were performed.
Lung ultrasound score
From the first day of admission until the patient was discharged from the hospital or 28 days after admission, at intervals of 24 hours, ultrasound (Turbo, US Sonosite, Curve Probe, 2–7 MHz; Sonosite Inc., Bothell, WA) was used by physicians trained in ultrasound who were unaware of the patient’s condition. They acquired images using a bedside lung ultrasound exam (BLUE) and assessed the lung at the standard BLUE points at the anterior chest wall and along a horizontal line, intersecting the anterior and posterior axillary lines at the end of expiration (12 positions in total; Figure 1). Image data were stored on the ultrasound scanner. Two other physicians who were unaware of the experimental design and trained in lung ultrasound assessed the stored images to determine the LUS. Four ultrasound aeration patterns were defined: (1) normal aeration (N): presence of lung sliding with A lines or fewer than two isolated B lines; (2) moderate loss of lung aeration: multiple, well-defined B lines (B1 lines); (3) severe loss of lung aeration: multiple coalescent B lines (B2 lines); and (4) parenchymal consolidation (C), the presence of a tissue pattern characterized by dynamic air bronchograms. For a given region of interest, points were allocated according to the worst ultrasound pattern observed: N = 0, B1 lines = 1, B2 lines = 2, and C = 3. The LUS ranged between 0 and 36 and was calculated as the sum of points at the 12 positions.5–8 The final LUS was taken as the mean of the two physicians’ readings (Figure 2).

Lung ultrasound exam points: Bedside lung ultrasound examination (BLUE) positions on the anterior chest wall and the intersection of the front and rear axillary lines.

Four ultrasound aeration patterns were defined: (a) normal aeration (N): presence of smooth movement of the pleural surface with A lines (*) or <2 isolated B lines (#); (b) moderate loss of lung aeration: multiple, well-defined B lines (B1 lines); (c) severe loss of lung aeration: multiple coalescent B lines (B2 lines); and (d) lung consolidation (C), the presence of a tissue pattern characterized by dynamic air bronchograms. For a given BLUE position, points were allocated according to the worst ultrasound pattern observed: N = 0, B1 lines = 1, B2 lines = 2, C = 3. The LUS ranged between 0 and 36 and was calculated as the sum of the points.
Data analysis
Data were analyzed statistically using SPSS version 22 (IBM Corp., Armonk, NY, USA). Means and standard deviations (SD) were used to describe data distributions. Correlation between the LUS and the clinical and laboratory findings was performed using Spearman’s rank correlation. Differences were considered statistically significant at P < 0.05.
Results
Thirty-two patients were enrolled in the study; six patients were excluded for hospital stays <48 hours or the discovery of pulmonary space-occupying lesions. Of the remaining 26 patients (discharged patients with survival assessed by telephone follow-up), 23 had died within 28 days after admission, for a 28-day mortality of 88.5%. There was no significant difference in initial characteristics between male and female patients (Table 1).
Baseline characteristics of the patients.

LUS, lung ultrasound score; PaO2, arterial blood O2 partial pressure; FiO2, fraction of inspired O2; sCr, serum creatinine; CRP, C-reactive protein; ICU, intensive care unit.
LUS changes in the patients
Pulmonary damage occurred in all patients enrolled during hospitalization. The final ultrasound score was significantly higher in all patients compared with the initial ultrasound score (16 ± 6 vs. 3 ± 3, P < 0.001), and there were no significant differences between men and women in final ultrasound score or in changes in the ultrasound scores (16 ± 4 vs. 15 ± 7; 12 ± 5 vs. 12 ± 6) (Figure 3a,b).

(a) The initial lung ultrasound score (LUS1) and the final lung ultrasound score (LUS2) in patients with paraquat poisoning. The final ultrasound score was significantly higher than the initial ultrasound score in all patients (P < 0.001). (b) Dynamic changes of lung ultrasound score of all patients.
Correlation between LUS and other variables
A decreased oxygen index and elevated LUS were observed in all enrolled patients. There was a significant negative correlation between LUS and the oxygen index (rho = −0.896, P < 0.001) (Figure 4).

Correlation between LUS and oxygen index. As the patient’s oxygen index decreased, the patient’s LUS increased, and there was a significant negative correlation between the LUS and PaO2 (rho = −0.896, *P < 0.001). LUS, lung ultrasound score; PaO2, arterial blood O2 partial pressure.
After lung injury occurred in the enrolled patients, early CO2 retention was not obvious, and some patients even had hyperventilation in the early stages. As lung damage worsened, CO2 retention gradually manifested, and the LUS and arterial blood carbon dioxide partial pressure (PaCO2) were significantly positively related (rho = 0.567, P < 0.001) (Figure 5).
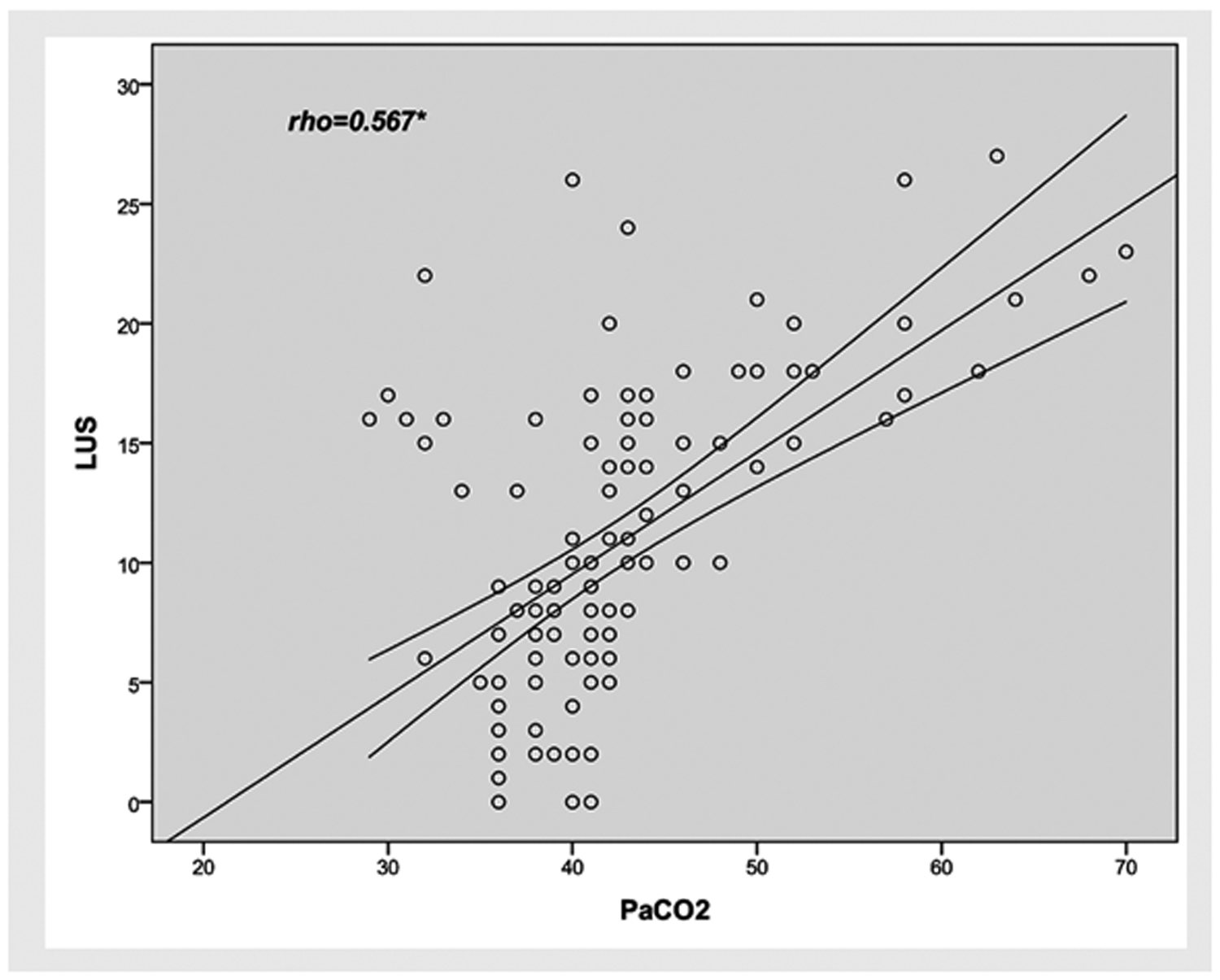
Correlation between LUS and PaCO2. There was a significant positive correlation between the LUS and PaCO2 (rho = 0.567, *P < 0.001). LUS, lung ultrasound score; PaCO2, arterial blood CO2 partial pressure.
During treatment of the patients, CRP increased and LUS was positively correlated with CRP (rho = 0.771, P < 0.001) (Figure 6). There was high consistency between ultrasound and CT images of the lungs (Figure 7).

Correlation between the LUS and CRP. The LUS and CRP increased to different degrees during the treatment of the selected patients, and there was a significant positive correlation between them (rho = 0.771, *P < 0.001). LUS, lung ultrasound score; CRP, C-reactive protein.

Changes in lung images in patients with paraquat poisoning. As the patient’s lung injury worsened, the CT showed that the patient’s right lower lung gradually showed interstitial edema and consolidation, and the corresponding lung ultrasound showed an increase in B-lines and lung tissue with dynamic inflation.
Discussion
In this study, all 26 patients had moderate to severe disease, developing multiple organ dysfunction with respiratory and renal impairment, and most patients eventually died. The pathologic mechanism of paraquat poisoning has not been fully clarified. According to existing research, the main mechanism of paraquat poisoning involves oxidative damage, inflammatory reaction, or apoptosis. Multiple organ dysfunction and failure, mainly lung injury, leads to death in poisoned patients. 9 Mortality was higher among the patients treated in our hospital than is reported in the current literature. 4 The patients admitted to our hospital may have had more severe poisoning and a longer duration of poisoning, which are the main prognostic factors in patients suffering from paraquat poisoning. 10
In all patients in this study, lung damage improved and adequate assessment of the lungs became an important part of the treatment. In the past, patients with paraquat poisoning were mainly evaluated using CT or chest X-ray to assess lung injury, 11 but with the progression of disease, especially low oxygen saturation, the likelihood of a patient being able to undergo CT examination is extremely low and the sensitivity and specificity of bedside chest X-ray examinations are poor.12,13 In addition, radioactive damage from CT and chest X-ray examinations should be avoided as much as possible. 14
In recent years, the application of pulmonary ultrasound in different diseases, such as trauma, shock, pleural effusion, and ARDS, has been confirmed,15,16 and has obvious advantages compared with chest radiography. 17 The results of this study suggest a significant negative correlation between LUS and oxygen index, as the correlation with PaCO2 was relatively weak, probably due to the early phase of lung injury with paraquat poisoning, with interstitial edema and pulmonary fibrosis resulting in a diffusion disorder as the main pathological change. A ventilatory disorder only complicated by infection or another disorder could arise in the middle and late stages of the disease, 18 whereas pulmonary ultrasound has good sensitivity to detect pathological changes in diffuse function such as pulmonary interstitial edema. 19
Paraquat poisoning is often accompanied by vomiting with aspiration, which may lead to a secondary infection in the late stage of lung injury. 2 Therefore, subsequent deterioration in oxygenation should point to the possibility of infection; there is also a significant correlation between LUS and CRP, similar to the findings of Yousef and De Luca, 20 but the correlation coefficient was lower than that for LUS and oxygen index. Therefore, lung injury is a more important factor than infection in paraquat poisoning. Finally, there was high consistency between pulmonary ultrasound and CT imaging, consistent with previous literature reports.15,21
This study had some limitations. First, the number of patients was small. In recent years, China has gradually banned the marketing of paraquat of different dosages and forms, which has led to a significant reduction in paraquat poisoning; however, we achieved statistical significance despite the small sample size. Second, this was a single-center study, and patients with paraquat poisoning may have had a bias in the time of poisoning and the initial treatment strategy. Third, the LUS is operator-dependent and cannot be fully objectively quantified. It should be used as an adjunct to chest radiography and CT in caring for patients with acute paraquat poisoning.
Conclusion
We found a reliable correlation between LUS, degree of lung injury, and oxygen index in patients with paraquat poisoning. Lung ultrasound and CT imaging results were highly consistent. Our results suggest that lung ultrasound can be used as an effective tool to evaluate lung injury in patients with paraquat poisoning. Further studies are required to confirm our results.
Footnotes
Acknowledgement
We thank Huijie Yu, Songao Xu, Xiangyun Zhu, and the staff of the Emergency Department of the First Hospital of Jiaxing for assistance with case collection.
Author contributions
PS (corresponding author) was in charge of the study design and data analysis. QQW was responsible for the data analysis and manuscript writing and cooperated with WLY, YCG, XBS, and YCS in the research work. All authors participated in the critical revision of the manuscript, and all authors approved the final version to be submitted.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was funded by the Science and Technology Project of Jiaxing (No. 2019AD32231).