
Abstract
This study was performed to describe the clinical features, risk factors, and treatment methods of uterine torsion in pregnancy. The most common symptoms are abdominal pain, fetal heart rate changes, and failure of cervical dilatation and are often accompanied by complete or partial placental abruption. Preoperative diagnosis is challenging even with the use of ultrasound. Uterine torsion in the third trimester is correlated with the presence of multiple uterine fibroids. The causes of gravid uterine torsion vary and the clinical manifestations are nonspecific. Early diagnosis and improved detection approaches are the keys to treatment of patients with uterine torsion. However, the preoperative diagnosis remains difficult and the diagnosis is often made during cesarean section.
Introduction
The most common symptoms of uterine torsion in pregnancy are abdominal pain, fetal heart rate changes, and failure of cervical dilatation and are often accompanied by complete or partial placental abruption. 1 Preoperative diagnosis is challenging, even with the use of ultrasound. Uterine torsion in the third trimester is correlated with multiple uterine fibroids.
Case presentation
On 20 October 2017, a married 35-year-old woman presented at 40+1 weeks of gestation with a 1-day history of lower abdominal tenesmus. Her last menstruation had occurred on 11 January 2017, and the expected date of childbirth was 19 October 2017. Urine human chorionic gonadotropin was positive 35 days after menopause. Early pregnancy reactions, such as nausea and vomiting, began at more than 40 days after menopause and lasted for nearly 1 month. The patient reported that a small myoma had been detected by color Doppler ultrasound in early pregnancy (the specific details were unknown) but that the myoma had not been detected by subsequent regular reexamination. Furthermore, the patient had no history of exposure to radiation, toxic chemicals, or other known risk factors. She also mentioned that she had undergone transabdominal myomectomy in 2010 (the specific details were unknown). Fetal movement began at 4 months of gestation and had actively persisted to date. The pregnancy was stable, but regular antenatal care had not been carried out and Down syndrome screening had not been performed. TORCH viruses (toxoplasmosis, other [syphilis, varicella-zoster, parvovirus B19], rubella, cytomegalovirus, and herpes) were negative, and the 75-g glucose tolerance test result was normal. The patient did not undergo prenatal diagnosis.
One day before presentation, the patient had developed a paroxysmal tenesmus sensation in the lower abdomen. She then visited our hospital and was admitted to our department. On presentation, the patient had irregular pain in the lower abdomen but no vaginal bleeding or discharge. The fetal movements were good, diet and sleep were acceptable, and stool and urination were normal. The patient’s temperature was 36.3°C, pulse rate was 78 beats/minute, respiratory rate was 20 breaths/minute, and blood pressure was 121/88 mmHg. The abdominal bulging was similar to that of a full-term pregnancy. A 2-cm transverse scar was observed on the pubic surface of the lower abdomen.
Obstetric examination revealed that the height of the uterus was 33 cm, the abdominal circumference was 101 cm, the fetal position was left occiput anterior, and the fetal heart rate was 145 beats/minute. The head of the fetus was exposed by the incision. The first exposed part was 3 cm above the ischial spine, the fetal membranes were not broken, the cervix was moderate in texture, and the opening of the womb was closed.
Adjuvant examination showed that the hemoglobin concentration was 102 g/L and that no abnormalities of coagulation function were present. Color Doppler ultrasound (performed on 20 October 2017 in our hospital) revealed the following: the pregnancy was intrauterine, fetal development was equivalent to full-term pregnancy, placental maturity was grade 2, and the fetal umbilical cord was possibly wrapped around the neck (Figure 1).

Color Doppler ultrasound examination showed that the pregnancy was intrauterine, fetal development was equivalent to full-term pregnancy, placental maturity was grade 2, and fetal umbilical cord was possibly wrapped around the neck.
The patient underwent cesarean section on 21 October 2017. During the operation, the original transverse incision of the lower abdomen was selected for the new port to access the abdomen. The surgical field was full of what appeared to be thickened and elongated round ligaments of the uterus and ovarian oviduct (these were subsequently proven to be the right appendages), which were located to the left of the center of the incision (Figure 2(a)). The lower segment of the uterus contained a rich vascular plexus, and the bladder reflex of the uterine peritoneum could not be identified. In the process of avoiding the vascular-rich areas, a transverse incision of the lower uterine segment was made, and a live male infant was removed. His body weight was 3,650 g, height was 55 cm, and Apgar scores ranged from 9 to 10. After delivery, the patient’s uterine contraction was good, the placenta was naturally expelled, and bleeding was minimal. The uterine incision was routinely sutured. Careful inspection then revealed that the uterus had twisted 120° counterclockwise, and the incision was located in the lower part of the posterior wall of the uterus. The uterus was repositioned, and oxytocin was locally injected. No uterine malformation was found (Figure 2(a)). Intraoperative exploration revealed 11 leiomyomas of various sizes located in the anterior wall of the uterus (Figure 2(b)). The largest was approximately 5 × 4 × 3 cm, and the smallest was approximately 1 × 0.5 × 0.5 cm. Hysteromyomectomy was performed at the patient’s request (Figure 2(c)). The postoperative pathological examination revealed uterine leiomyomas with degeneration (Figure 2(d)). After the operation, antibiotics and oxytocin were routinely administered. The patient was discharged on postoperative day 5. No abnormalities were found in either the mother or infant. The patient was instructed to use contraception upon discharge.
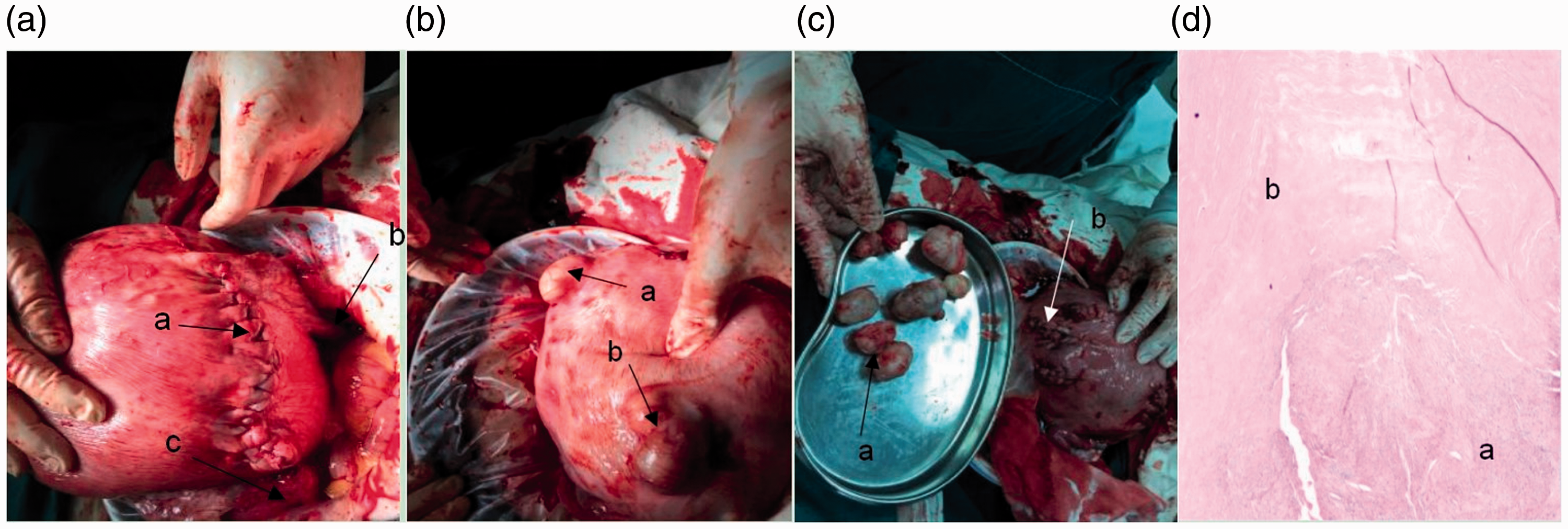
(A) The uterus after the cesarean section is shown, and the anatomic position has been restored. (a) The cesarean section incision was located at the posterior wall of the uterus. (b) The right appendages with a 180° counterclockwise twist are shown, indicating that the anatomical position has been restored. (c) The left appendages are shown. (B) (a and b) Multiple myomas of the uterus (most were subserosal uterine leiomyomas, but some were intramural leiomyomas). (C) (a) Several removed uterine leiomyomas are shown (in total, 11 uterine leiomyomas were resected). (b) The uterine leiomyoma cavity is shown. (D) Pathological images after the hysteromyomectomy. (a) Uterine leiomyoma. (b) Uterine leiomyoma with degeneration.
Ethics
This study was conducted with approval from the Ethics Committee of Xuzhou Central Hospital and was conducted in accordance with the Declaration of Helsinki. The patient provided written informed consent.
Discussion and conclusions
Causes of uterine torsion during gestation
Uterine torsion is defined as torsion of the uterus around its longitudinal axis exceeding 45°, and most torsions are approximately 180°. However, there are also reports of 60° to 720° torsions. Uterine torsion during gestation is very rare in humans, but it is common in cattle and cats. Because the uterine ligaments play a balancing role, it is normally very difficult for uterine torsion to occur. Hence, uterine torsion is rare, and uterine torsion in full-term pregnancy is even rarer. The causes of uterine torsion in the gestational period remain unclear. As pregnancy advances, the cervix and lower segment of the uterus gradually grow and become soft, and the tissues become congested and loose. If the uterus is overactive at this time, uterine torsion may occur.1,2 Structural abnormalities of the uterus, such as a double uterus, rudimentary horn of the uterus, uterine leiomyoma, adnexal cyst, abnormal fetal position, or abrupt change of fetal posture, may be causes of uterine torsion. Myoma and pregnancy have adverse effects on each other, and the most serious effect is uterine torsion.3–5 A study by Huang et al. 6 revealed that the occurrence of uterine torsion in the third trimester of pregnancy may be correlated with an abnormal fetal position, older maternal age, and uterine ligament relaxation.
Clinical manifestations of uterine torsion during gestation
Li et al. 7 suggested that uterine torsion is easily misdiagnosed. Furthermore, its preoperative diagnosis is difficult, and it is usually diagnosed during caesarean section. Because its clinical manifestations vary, even if it is asymptomatic, chronic uterine torsion often has no typical clinical manifestations. In contrast, acute uterine torsion can be characterized by acute abdominal pain, which can be easily confused with acute abdomen, such as that caused by appendicitis, torsion of the ovarian tumor pedicle, and intestinal obstruction. The severity of uterine torsion depends on the magnitude and duration of the torsion, and its manifestations may include dystocia, abdominal pain, excessive uterine tension, vaginal bleeding, and shock. The typical clinical symptoms of uterine torsion are similar to those of placental abruption, uterine rupture, abdominal pregnancy, acute appendicitis, and pelvic mass torsion. Uterine torsion can lead to occlusion of the blood circulation of the uterus and appendages, and placental ischemic injury can lead to decidual necrosis with vascular rupture and bleeding, followed by preterm labor and separation of the decidua and placenta. 8 Furthermore, severe acute uterine torsion can lead to placental abruption 9 and intrauterine fetal death.10–12
Auxiliary diagnosis of uterine torsion during gestation
Ultrasound has very high value and clinical significance in the diagnosis of uterine torsion.13–15 Although color Doppler ultrasound cannot accurately diagnose uterine torsion, it can determine whether the placental position is inconsistent with the original position. In particular, when the placental position is found to be reversed from its original position, uterine torsion should be considered. 16 Computed tomography and magnetic resonance imaging are also helpful in the diagnosis to a certain extent. Vaginal examinations of patients with uterine torsion reveal that the cervix is high and difficult to touch and that the vaginal mucosa is spiral.
Treatment of uterine torsion during gestation
When uterine torsion in full-term pregnancy is diagnosed, surgery should be immediately performed. The main purpose of the operation is to remove the factors that endanger the safety of the mother and infant, such as fetal distress and placental abruption, thereby saving the lives of the mother and infant and preserving the uterus. Before 34 weeks of pregnancy, there is an opportunity to reposition the uterus and continue pregnancy. If possible, in a full-term pregnancy, the uterus should be repositioned and cesarean section should be carried out. When repositioning the uterus is difficult or the fetus cannot be located, the main treatment principle should be to ensure safe delivery of the fetus. During the operation, a transverse or classic cesarean section should be performed to avoid the uterine arteries and veins according to specific conditions and thus avoid massive hemorrhage. If the torsion time is long, the uterus may become necrotic and the blood vessels may develop thrombosis. Hence, the uterus should be removed. 17
Prevention
Uterine torsion is seriously harmful to both the mother and infant. Therefore, prenatal health care, prenatal examination, and ultrasound examination should be optimized; the patient’s sexual activity should be reduced as far as possible or avoided; and heavy physical labor should be avoided in the second and third trimesters of pregnancy. For patients with a history of uterine leiomyoma, this should be comprehensively considered according to the size and location of the myoma and the history of myomectomy. Furthermore, patient care after pregnancy should also be optimized, and abdominal pain and other symptoms should be monitored and managed in a timely manner. With respect to the risks of placental abruption, red degeneration of uterine leiomyomas, subserosal uterine fibroid torsion, and abortion during gestation, no relevant reports to date have indicated whether it is necessary to fix the relaxed ligament during cesarean section. Hence, further clinical observations are needed.
Footnotes
Acknowledgements
We would like to acknowledge the hard and dedicated work of all the staff members who implemented the intervention and evaluation components of the study.
Availability of data and materials
All materials described in the manuscript, including all relevant raw data, will be freely available to any scientist wishing to use them for non-commercial purposes without breaching participant confidentiality.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was funded by the Basic and clinical study of radionuclide iodine-125 combined with dual-regulation oncolytic virus in highly targeted treatment of prostate cancer (2015-WSW-078), Effect and mechanism of deubiquitinase OTUD5 regulating A K D ubiquitination on radiosensitivity of cervical cancer (KC15SH023), and Provincial department of education-Methylation regulation of Reh gene by MAP30 and its anti bladder tumor mechanism (18KJB18000). The funding body had no role in the design of the study; collection, analysis, or interpretation of the data; or writing of the manuscript.