
Abstract
Gallstone disease is common in China and is generally treated with laparoscopic cholecystectomy. For some patients with normal contraction function and a small number of stones, endoscopic minimally invasive cholecystolithotomy is an additional possible treatment method that avoids complications related to laparoscopic cholecystectomy. Here, we describe a 45-year-old woman who underwent endoscopic minimally invasive cholecystolithotomy and was found to have duplicate gallbladder, which was not diagnosed preoperatively. We discuss the usefulness of the endoscopic minimally invasive cholecystolithotomy procedure and the management of duplicate gallbladder in patients undergoing endoscopic minimally invasive cholecystolithotomy.
Keywords
Introduction
Gallstone disease (GD) is a disorder that frequent occurs in humans, representing a strain on healthcare systems worldwide. The prevalence of GD is approximately 10% to 15% of the United States adult population; 1 in China, the morbidity of GD is approximately 4% to 7%. 2 Thus far, laparoscopic cholecystectomy (LC) has become the gold standard treatment for GD and is one of the most commonly performed general surgical procedures. 3 However, endoscopic minimally invasive cholecystolithotomy (EMIC) is a new surgical method for treatment of GD, which has shown satisfactory clinical outcomes in some patients.4,5 Here, we describe a patient who underwent EMIC and was found to have duplicate gallbladder (DG). We discuss the usefulness of the EMIC procedure and the management of DG in patients undergoing EMIC.
Case Report
A 45-year-old woman with a 2-year history of intermittent right upper abdominal pain induced by heavy physical labor and food intake (especially greasy food) presented to her local hospital for treatment in June 2015. She reported upper abdominal swelling pain after food intake, without nausea, vomiting, jaundice, or fever. She had no other relevant medical history or history of prior surgery. After several blood tests (e.g., routine blood test, liver and kidney function assessment, and blood amylase measurement) and an abdominal ultrasound examination, she was diagnosed with GD; antiphlogistic and cholagogic therapy was recommended, with periodic follow-up.
In November 2017, the patient had exhibited a progression-free status for nearly 2 years, but presented to our clinic with aggravated right upper quadrant pain. Abdominal ultrasound of the gallbladder showed a stone that was 1.3 × 0.8 cm, although the gallbladder wall was smooth. Dilatation of the common bile duct was not observed, nor was dilatation of the pancreatic duct (Figure 1). No other abnormalities were observed in the biliary system. Gastroscopic examination to exclude stomach disease revealed that the patient also exhibited chronic non-atrophic gastritis. Therefore, the patient was scheduled to undergo EMIC.

Abdominal ultrasound examination showed the stone within the gallbladder (arrow). A diaphragm in the gallbladder was misdiagnosed as gallbladder folding.
The operation was performed using the conventional three-port technique. A 10-mm trocar for the video laparoscope was placed above the umbilicus; another 10-mm trocar was inserted 3 cm below the xiphisternum. In addition, a 5-mm trocar was placed 2 to 3 cm below the right costal margin in the midclavicular line. A small incision was made in the gallbladder fundus and bile was aspirated; subsequently, a choledochofiberscope was inserted in the gallbladder to retrieve the stone. One cholesterol polyp was retrieved, with a size of approximately 0.2 × 0.2 cm; however, the polyp did not contain a stone. The preoperative examination had shown that the size of the gallbladder stone was approximately 1.3 × 0.8 cm. Thus, we investigated whether the stone had been discharged into the intestine or hidden in the gallbladder wall. Several choledochoscopy attempts were made, but no stone was retrieved. An experienced sonographer was asked to assess whether the stone remained within the gallbladder, using intraoperative ultrasound. The laparoscopic incision was extended to the bottom of the gallbladder, which revealed the presence of an additional sac filled with bile; the stone was present inside this sac. Notably, there was no obvious bile duct within the second sac, and a diaphragm was present between this sac and the gallbladder (Figure 2). The patient was determined to exhibit Type I DG; moreover, some small branching bile ducts allowed communication between the two gallbladder cavities. After resection of the gallbladder diaphragm, the incision in the fundus was sutured with absorbable sutures and the surgery was completed (Figure 3). The operating time was 2 hours, and the volume of blood loss was approximately 20 mL. The patient did not develop any postoperative complications and was discharged 2 days postoperatively.

Stone shown in the duplicate gallbladder, along with the diaphragm.

Gallbladder shown after completion of the operation.
One month later, the patient returned to our hospital for follow-up and abdominal ultrasound showed no stone in the gallbladder (Figure 4). The patient has not experienced abdominal pain during the follow-up period, and has been able to consume a normal diet. The patient provided consent for publication of this report. The publication of this case report was approved by the Ethical Committee of Xiangya Hospital on 23 July 2019 (Approval No.: 201907496).
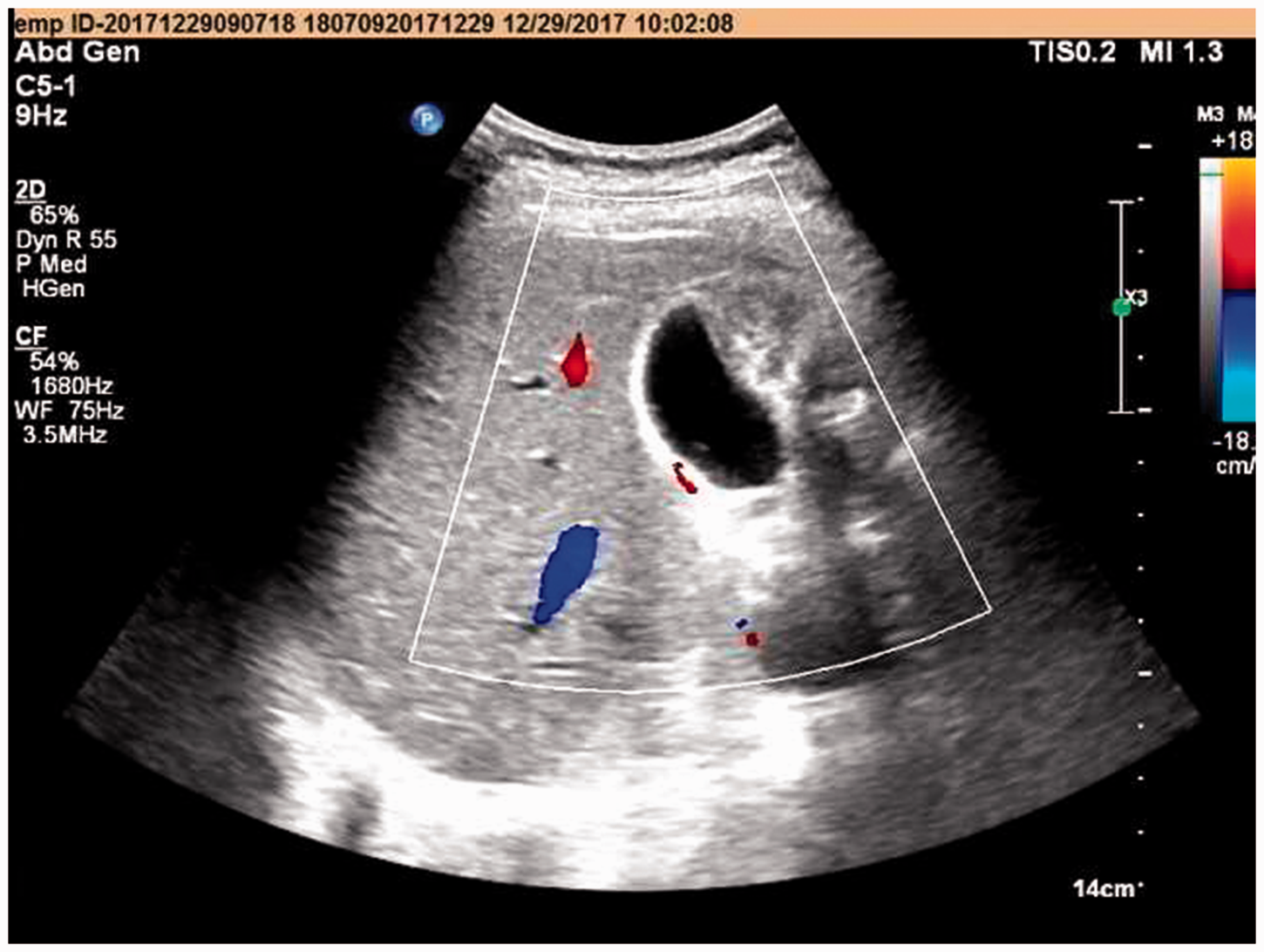
Image of the gallbladder at 1 month postoperatively.
Discussion
Gallstones can be symptomatic or asymptomatic. Notably, most gallstones are asymptomatic; however, when symptoms develop, it is likely that affected patients will experience recurrent episodes of symptoms.3–5 Overall, up to 20% of adults develop gallstones. Among the patients with gallstones, up to 32% of those who do not undergo operations may experience recurrent cholecystitis, choledocholithiasis, gallstone pancreatitis, gallstone ileus, and cholangitis; these comorbidities increase the cost of subsequent hospitalizations and cause great harm to patient health.2,6 An estimated 90% of patients with typical biliary symptoms and gallstones are expected to be symptom-free after cholecystectomy; therefore, many clinicians strongly advocate initial cholecystectomy.4,5 However, most patients with incidental findings of asymptomatic gallstones do not require surgery.
Removal of the gallbladder during open surgery has been performed for approximately 140 years, while LC has been performed for nearly 30 years. 7 Approximately 500,000 cholecystectomies are performed yearly in the United States with minimum morbidity (pooled prevalence range, 1.6%–5.3%) and mortality (pooled prevalence range, 0.08%–0.14%). LC remains the unchallenged gold standard treatment approach, with conversion rates of open operation between 4.2% and 6.2%. However, LC involves some complications.8,9 Biliary duct injuries and hemorrhages remain the most common complications. The incidence rate of unretrieved gallstones in the peritoneal cavity is high, at 2.4% to 50%. Vascular injuries during LC may occur more often during dissection of Calot’s triangle structures. Furthermore, 10% of patients who undergo cholecystectomy subsequently develop post-cholecystectomy syndrome.8,9 These prior findings indicate that LC is not always an effective approach.
Attempts to reduce surgical discomfort have led to numerous minimally invasive approaches. The function of the gallbladder is storage and concentration of bile. Clinicians are increasingly realizing that removal of the gallbladder is harmful to digestive function. In recent years, some Chinese experts have reported the long-term feasibility of EMIC in clinical practice. 10 This operation is widely used in China and its use is supported by the Chinese Medical Association. EMIC is a selective operation method for gallstone patients that enables preservation of gallbladder function, avoidance of complications related to LC (e.g., biliary duct injuries and hemorrhages, vascular injuries during LC, post-cholecystectomy syndrome after LC), and achievement of a low stone recurrence rate of 1.9% to 5.39%.4,10 Our patient in this report had a strong preference for preservation of the gallbladder and has remained disease-free after the EMIC procedure.
DG is a rare congenital abnormality of the hepatobiliary system with an incidence of 1 per 3800 to 5000. It is seldom diagnosed preoperatively and is usually missed during surgery. Thus far, it has only been detected via preoperative imaging in 50% of affected patients. Ultrasound is often the first-line imaging modality used for assessment of patients with signs of cholecystitis/biliary colic. Sonographically, it is difficult to assess alterations in the anatomy of the biliary tree. 11 For this patient, we missed the diagnosis of DG preoperatively; moreover, no stone was found during intraoperative endoscopy. Following intraoperative ultrasonography and incision of a secondary gallbladder, the stone was found. Based on the Harlaftis classification of DG, our patient was diagnosed with Type 1 (split primordial) DG: 11 a single cystic duct that enters the common bile duct. After the operation, we reexamined ultrasonic images and found the presence of a diaphragm in the gallbladder, which had been misdiagnosed as gallbladder folding. Accordingly, there are two important questions: how can a definite preoperative diagnosis of DG be made? If this diagnosis cannot be made, how can the stone be removed? Notably, magnetic resonance cholangiopancreatography or endoscopic retrograde cholangiopancreatography (although more invasive) can be used preoperatively as supplementary tools to assess biliary anatomy. When patients are scheduled for EMIC, intraoperative endoscopy and operative ultrasonography may be necessary for successful completion of the EMIC procedure.
In conclusion, LC and EMIC are two most common surgery procedures in China. EMIC is useful for patients who have a strong preference to preserve normal gallbladder function. Successful preoperative diagnosis of DG is noted in only half of the patients who undergo EMIC. For patients who have GD combined with DG, the EMIC procedure seems to be challenging. By using a combination of intraoperative endoscopy and operative ultrasonography, patients with Type 1 DG can safely undergo EMIC.
Footnotes
Acknowledgements
The authors thank Dr Jintang Liao and Dr Ping Xue at the Department of Radiology, Xiangya Hospital for their contributions to this article.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.