
Abstract
Objective
This study was performed to investigate the feasibility of tubularization of the ileal seromuscular fold for long-segmental ureteral reconstruction in a canine model and assess the clinical application of this procedure.
Methods
The experimental study was conducted on six beagles. An ileal segment was chosen and folded along its longitudinal axis and thereafter sutured to tubularize the serous surface. The tubularization of the ileal seromuscular fold was designed to be 10 to 12 cm for ureteral substitution. The neo-ureters were pathologically examined. A patient in our hospital also underwent this reconstructive operation. Several blood parameters were assessed and urography was performed for postoperative evaluation.
Results
All animals and the patient tolerated the operation and recovered as planned. No severe postoperative complications occurred. Blood examination revealed that renal function was within the normal range. Urography indicated patency of urine excretion without leakage or stenosis. In the patient, antegrade urography showed rhythmic peristalsis of the neo-ureter. The pathologic examination revealed a healthy condition of the neo-ureter and an open lumen with a serous epithelial lining.
Conclusion
Ureteral reconstruction by tubularization of the ileal seromuscular fold is anatomically possible and was preliminarily validated in a patient in the clinical setting.
Keywords
Introduction
With the development of endoscopic technology, the incidence of iatrogenic ureteral injury has reportedly increased. 1 Such ureteral injuries generally lead to ureteral defects and stenosis and sometimes even involve the long-segmental ureter. 2 Ureteral replacement is the preferred surgical management technique for long-segmental injuries; such replacement techniques include ureteroplasty using a bladder muscle flap (Boari flap), ileal substitution, and use of tissue engineering materials. 3
An ideal ureteral substitute requires tissue compatibility, an adequate blood supply, similarity to the normal ureteral structure, preservation of ureteral peristalsis, and technical feasibility without reabsorption of urine or lithogenesis. 4 Ileal substitution is universally applied as a ureteral replacement technique, and the abundant material available for this procedure makes it particularly advantageous. However, it also has several disadvantages, such as reflux-associated infection and loss of renal function, electrolyte and metabolic disturbances, and mucus secretion. 5
Some modified ileal substitution procedures are reportedly associated with fewer postoperative complications; these procedures are represented by Yang–Monti techniques.6,7 Despite the improvement of achieving a smaller caliber, operations involving the mucosal lining are always potentially associated with the above-mentioned problems. Therefore, whether demucosalized intestine is a feasible method is a primary consideration. Several recent experimental studies have explored promising models using autologous materials with non-mucosal linings.8,9
This study was performed to investigate a novel procedure using tubularization of the ileal seromuscular fold for long-segmental ureteral reconstruction. The experimental results and preliminary clinical application are presented and discussed below.
Materials and methods
Experimental canine study
Animals
This experimental study was conducted on six healthy adult male beagles obtained from the School of Agriculture, Shanghai Jiao Tong University. At the time of the operation, the dogs ranged in weight from 12 to 14 kg. The animals were caged individually in a clean-graded environment and provided filtered water and a standard diet until 10 hours prior to the surgical procedure. The study was reviewed and approved by the ethics committee of Huashan Hospital, Fudan University. The “Instructive Notions with Respect to Caring for Laboratory Animals,” published in 2006 by the Science and Technology Department of China, was strictly followed. The procedure was carried out at the laboratory animal center in the School of Agriculture, Shanghai Jiao Tong University from June 2017 to January 2018.
Surgical methods
The whole procedure was performed under general anesthesia. After opening the abdomen cavity through a median incision, the full-length right-side ureter (approximately 15 cm) was dissociated, and 10 cm of the middle part was resected. A 4.7-Fr double-J stent was inserted into both the proximal and distal stumps with a guide wire. An ileal segment around the right-side ureter was chosen for reconstruction and was in an isoperistaltic direction with the native ureter. The ileal segment was folded along its longitudinal axis, with the stent buried inside; it was thereafter sutured in an interrupted pattern to tubularize the serous surface (Figure 1(a), (b)). The reconstructive tube was designed to be 10 to 12 cm long. Its two ends were anastomosed to the proximal and distal stumps of the ureter, respectively (Figure 2). The ureteral stumps were inserted into the upper and lower ends of the reconstructive tube and fixed by full-thickness 4-0 absorbable sutures placed in an interrupted pattern in the ureteral wall and seromuscular layer of the intestinal wall (Figure 1(c)). A side-to-side intestinal anastomosis was conducted between the two arms of the substitutive ileal segment to regain the intestinal continuity.

Schematic diagram of tubularization of ileal seromuscular fold and anastomosis. (a) Transverse section view before tubularization. (b) Transverse section view after tubularization. (c) Longitudinal section view of anastomosis. White area: intestinal cavity. Gray area: intestinal wall. Pink area: mesentery. Yellow area: cavity of neo-ureter. Blue area: ureteral stent. Orange area: ureter wall. Purple line: suture.

Photographs of the canine operation. (a) Part of the right ureter was resected. (b) Anastomosis of the neo-ureter. Single arrow: proximal ureteral stump. Double arrow: distal ureteral stump.
Postoperative management and surveillance
The dogs were fasted for the first postoperative day; a liquid and normal diet was then started from the second and fourth day, respectively. All animals received ceftriaxone for the first 3 days and intravenous glucose until they began eating a normal diet. Postoperative surveillance included measurement of vital signs and monitoring of the urination and defecation conditions.
The ureteral stent was maintained for 8 weeks and removed through a brief cystostomy. Routine blood examinations and measurement of serum creatinine, urea nitrogen, and electrolytes were performed both before and 12 weeks after the procedure. Intravenous urography was conducted, and the experimental animals were then euthanized by intravenous injection of potassium chloride under general anesthesia.
Pathologic examination
The right-side kidney and ureter together with the peripheral connective tissue were obtained after exploration of the abdominal cavity and surgical field. The specimens were immediately fixed with formalin for 24 hours, embedded in paraffin, and stained with hematoxylin and eosin. A microscopic evaluation was performed separately by two experienced pathologists.
Clinical case
Clinical data
We recruited one patient during the study period (January 2018–June 2019). The patient was a 31-year-old woman with a complex surgical history. She had undergone lumbar spinal fusion with instrumentation for treatment of a giant cell tumor of bone 5 years previously, and the internal fixation device was removed in May 2018. During the latter operation, the right common iliac artery was injured and immediately repaired. The patient presented with a fever with delayed incision healing 10 days after the operation. Exploratory surgery indicated a right ureteral injury. A ureteral stent was inserted via ureteroscopy and was replaced by a new stent 2 months later. The patient thereafter developed severe hematuria and hemorrhagic shock. After withdrawal of the ureteral stent, a digital subtraction angiography was performed and a ureteroarterial fistula was identified. A covered arterial stent was then placed. During the postoperative follow-up, severe hydronephrosis was discovered; therefore, the patient underwent percutaneous nephrostomy to conserve her renal function.
In general, the patient was in good health during her preoperative evaluations. Blood tests and emission computed tomography indicated that the ipsilateral kidney function was normal. Antegrade urography and computed tomography (CT) showed that the renal pelvis was moderately dilated with a nephrostomy tube inside (Figure 3(a), (b)).
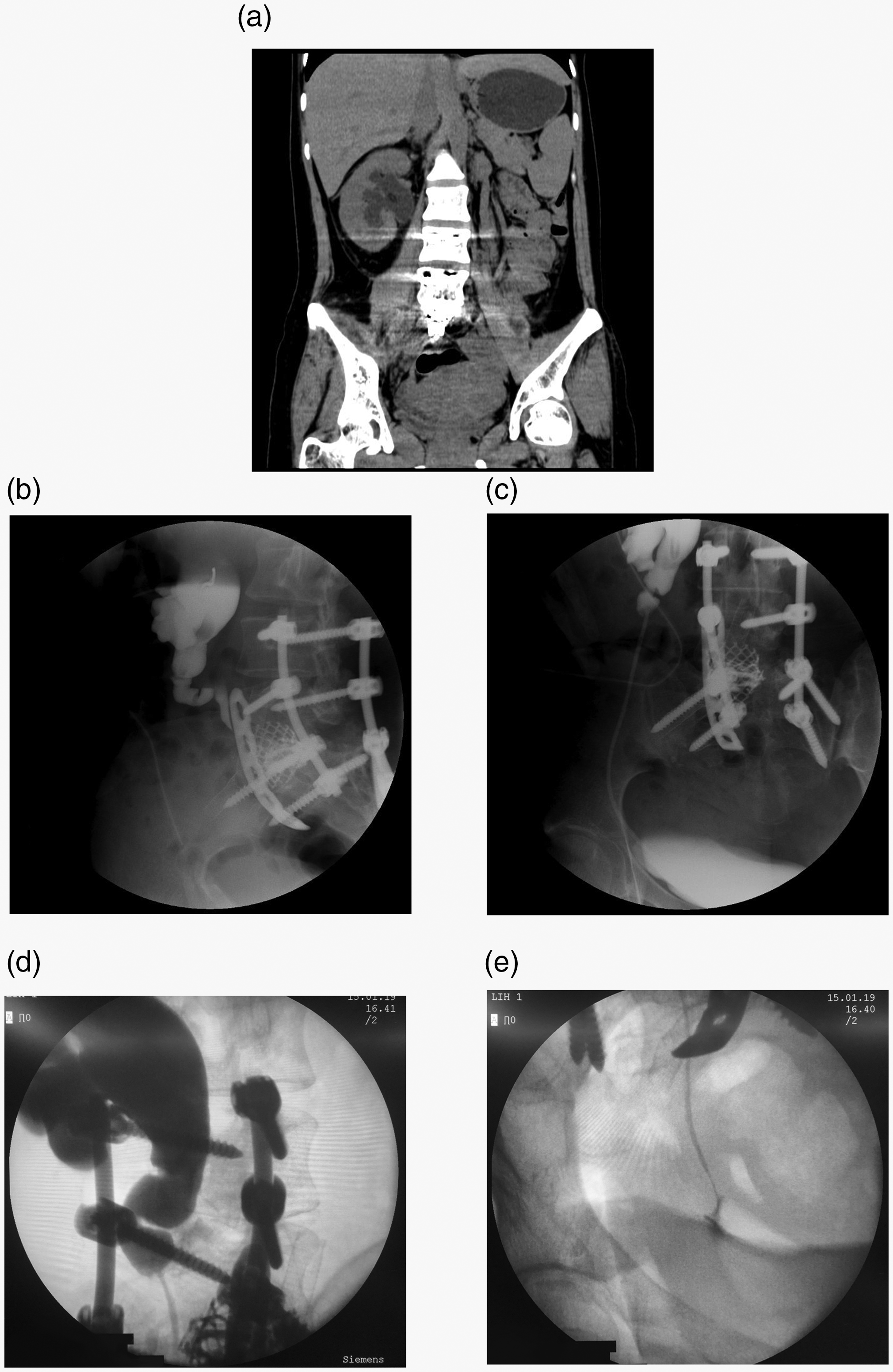
Radiologic evaluations of the clinical case. (a) Preoperative computed tomography scan. (b) Preoperative urography. (c) Urography at 6 weeks postoperatively. (d), (e) Urography after removal of the stent.
Surgical procedure
Under sufficient written informed consent, the patient underwent a reconstructive operation similar to the procedure described above. Through intraoperative exploration, we found that the injured ureter was adhered and fixed to the peripheral connective tissue, very close to the right iliac vessels. The length of the involved ureter was approximately 12 cm. The dilated proximal ureter and the bladder were dissociated for anastomosis. The proximal end of a selected ileal segment was amputated and closed, and the seromuscular fold was tubularized into a 15-cm neo-ureter to guarantee tension-free anastomosis. A 7-Fr indwelling double-J stent was placed in the neo-ureter. The proximal ileum was anastomosed to the distal ileum in a side-to-side fashion (Figure 4). A peritoneal drain was placed along the surgical field before closure of the abdominal incision.
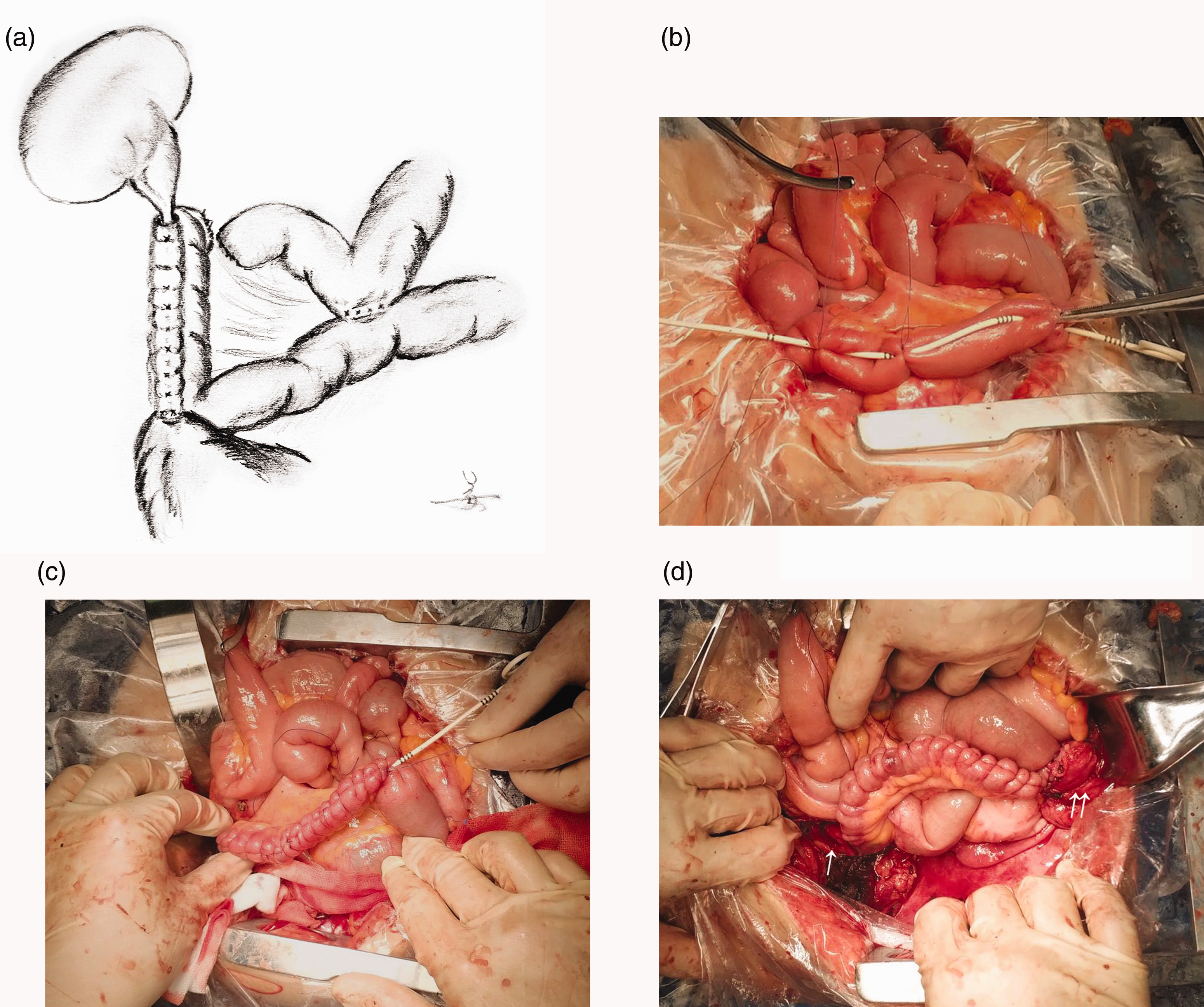
Schematic diagram and photographs of the clinical operation. (a) Schematic diagram illustrated by the corresponding author. (b) Initiation of tubularization. (c) Completion of tubularization. (d) Completion of anastomoses. Single arrow: proximal ureteral stump. Double arrow: bladder.
Postoperative follow-up assessment
The patient was fasted during the initial postoperative period and then gradually returned to a liquid and normal diet. Her vital signs, urination, intestinal recovery, and drainage were observed.
Removal of the double-J stent by cystoscopy was planned 12 weeks after the operation. Routine blood and urine examinations; measurement of serum creatinine, urea nitrogen, and electrolytes; and bacterial cultures of urine were performed after the operation and after removal of the stent. Antegrade urography was performed at 6 weeks postoperatively and after removal of the stent.
Results
Experimental canine study
All six beagles tolerated the procedure and survived with well-healed wounds at the end point of the experiment. Food intake and other activities, including urination and defecation, were regularly observed and found to be normal. There were no obvious signs of complications such as urine leakage, peritoneal infection, or ileus.
Exploration of the abdominal cavity revealed no obvious ascites or local hydrops, and the neo-ureters and anastomotic sites were intensely wrapped by peripheral tissue. An abundant blood supply was observed in the corresponding mesenteric membrane. There was no obvious enlargement of the ipsilateral kidneys, and the proximal ureters had mild hydronephrosis. Methylene blue was injected into the renal pelvis to determine whether urine leakage was present, and extravasation was undetectable along the entire length of the neo-ureters.
The results of the laboratory evaluations were mostly within the normal range, especially the serum creatinine, urea nitrogen, and electrolyte levels. Intravenous urography indicated that the neo-ureters had patent urine excretion and adequate calibers. Mild dilation of the proximal ureters was identified, which was in accordance with the macroscopic character. No obvious extravasation or retention of contrast was detected, suggesting that no fistula or stenosis of the neo-ureters was present (Figure 5).

Postoperative intravenous urography of the canine model.
Microscopic examination of the reconstructive segments demonstrated a healthy condition with slightly larger calibers than normal. The lining epithelium was continuous and vital, consistent with intestinal serosa, and showed no necrosis or detachment (Figure 6).

Histological examination of the neo-ureter in the canine model. Transverse section. (a) ×4. (b) ×10.
Clinical case
The reconstructive operation was successful. The total operation time was 210 minutes. No intraoperative or postoperative blood transfusion was required. The patient was hospitalized for 1 week after the operation. A liquid diet was started on postoperative day 4, and no signs of ileus, peritonitis, intestinal anastomotic leakage, or urinary leakage were observed. Serious urinary symptoms, such as severe hematuria, urinary irritation, or ipsilateral backache, were not observed. The nephrostomy tube remained clipped from postoperative day 5. The peritoneal drain was removed 2 weeks after the operation.
The blood examinations indicated no bloodstream infection and normal renal function. The urine tests showed an increased white blood cell count and positive leukocyte esterase (++). Both the bacterial cultures of urine showed no growth.
Compared with the preoperative CT scan, all of the postoperative urography images showed a similar extent of pelvis dilation. The first antegrade urography examination suggested that the ureteral stent was located properly. Contrast agent was observed filling the dilated pelvis, passing through the stent, and gradually filling the bladder without obvious extravasation (Figure 3(c)). During the antegrade urography examination after removal of the stent, rhythmic peristalsis of the neo-ureter was observed as shown by continuous excretion of contrast agent. No extravasation of contrast agent was recognized. There was no apparent stenosis of the ureteral lumen along the whole neo-ureter. The contrast agent flowed into the bladder through the new ureteral orifice (Figure 3(d), (e)).
Discussion
In addition to renal autotransplantation, long-segmental ureteral injuries and strictures generally require ureteral substitution. Among all tissues available for substitution, the ileum is one of the most frequently used because of its availability and feasibility. 10 Despite these benefits, the classic procedure is usually associated with several significant postoperative complications. 11 The main concern is the absorptive and secretory functions of intestinal mucosa, which may result in urinary infection, lithogenesis, electrolyte and/or acid–base imbalances, and potential loss of renal function. A neo-ureter with an inappropriate caliber can exacerbate hydronephrosis and consequently accelerate impairment of renal function.12,13 Development of the Monti and Mitrofanoff techniques has improved this limitation to a large extent.6,7
Recent experimental studies have focused on establishment of novel approaches for ureteral reconstruction, and most investigators have taken the above-mentioned issue into consideration. Several substitute materials originating from the intestine have been used, among which some can solve the problem by avoiding involvement of the intestinal mucosa. Previous reports have described the use of an intestinal seromuscular tunnel, 14 a seromuscular tapered ileal tube, 8 and an intestinal seromuscular segment with an autograft of bladder mucosa. 9 These modified approaches using intestinal segments were verified to be feasible for rebuilding the ureteral structure with a complete urothelial lining. Avoidance of the mucosal surface results in fewer absorptive and infective complications. However, demucosalized intestinal segments may increase the risk of shrinkage and regrowth of the original gastrointestinal epithelium. 15
Another important point mentioned in a prior study is the isoperistaltic direction of the neo-ureter with the native ureter. 14 We hypothesized that the intestinal peristalsis would synchronize to the neo-ureter in this model, which would facilitate urine transportation toward the bladder. In our clinical case, this hypothesis was validated at the time of the second postoperative urography examination, which demonstrated rhythmic peristalsis of the neo-ureter.
Urologists must consider that although the neo-ureter has a complete urothelial lining and potent caliber, lack of physiological peristalsis may eventually lead to hydronephrosis and impairment of renal function. The most common reason for this is that the neo-ureter usually lacks enough smooth muscle, innervation, or both. 16 Therefore, rebuilding the function of urine transportation is as crucial as structural reconstruction. The most effective techniques with which to generate effective urine transportation in the neo-ureter are worth considering and discussing in ureteral reconstruction, especially for long-segmental ureteral injuries. Because of its physiological characteristic of peristalsis, intestinal tissue may be an optimal choice for ureteral reconstruction.
In addition to the advantages of conventional ileal substitution, including efficient substitutive material, adequate blood supply, and flexibility for reconstruction, our procedure can theoretically reduce the incidence of intestine-related infection and lithogenesis. However, the potential complications associated with the absorptive characteristic of the peritoneum must be considered. A potentially disastrous complication is urinary peritonitis. In both the experimental animal study and clinical case described in the present report, the postoperative serum creatinine, urea nitrogen, and electrolytes were within normal limits; this suggested that the absorptive effect was insignificant. This may be attributed to the limited internal surface of the neo-ureter.
Conclusion
Long-segmental ureteral reconstruction is still a challenging issue for urologists worldwide. Despite the limitations of our small sample size and short-term follow-up, especially in the clinical case, our preliminary findings indicate that tubularization of the ileal seromuscular fold is anatomically possible for long-segmental ureteral reconstruction in both animal models and clinical patients. The main benefits of the procedure are avoidance of intestinal mucosa and maintenance of ureteral peristalsis. Further studies with larger sample sizes are expected to confirm the long-term functional efficacy and safety of the procedure.