
Abstract
Objective
Postoperative delirium (POD) has rarely been investigated in breast cancer patients. Herein, we assessed the association between serum levels of the inflammatory biomarker translocator protein (TP) and the occurrence of POD in breast cancer patients.
Methods
In this prospective, observational study, TP levels were detected in preoperative and postoperative serum samples from 152 elderly breast cancer patients, samples from 152 healthy elderly women, and samples from 152 elderly women with benign breast diseases. The relationship between serum TP levels and POD was investigated using multivariate analysis.
Results
TP levels in postoperative patient serum samples were significantly higher than in preoperative patient serum samples and serum from women in the two control groups. Postoperative serum TP levels were independently correlated with serum C-reactive protein levels and the occurrence of POD. Postoperative serum TP levels had a high discriminatory ability for POD under the receiver operating characteristic curve.
Conclusions
Increased postoperative serum TP levels are independently associated with the degree of inflammatory response and the risk of POD in elderly breast cancer patients, substantializing TP as an inflammatory biomarker that can efficiently discriminate POD after breast cancer surgery.
Introduction
The incidence of cancer has been increasing annually worldwide.1–3 Breast cancer is a common type of cancer that greatly affects women’s health.4–6 Surgery is an important treatment modality for various cancers, including breast cancer.7–9 However, some postoperative complications, including postoperative delirium (POD), are unavoidable during surgery.10–12 Growing data show that POD, which can easily occur in elderly patients, can increase patient mortality and prolong hospital stays.13–16 While there have been many reports of POD in cancer patients,17–19 few studies have investigated POD in breast cancer patients.20,21 Although the mechanisms underlying POD are not fully understood, it is known that cerebral neuronal damage can result in POD. Among the variety of causes, inflammation might be an important process of brain injury.22–24 Thus, we may be able to identify inflammatory biomarkers that can discriminate those at a high risk of POD among breast cancer patients.
Translocator protein 18 kDa (TP) was formerly recognized as a peripheral benzodiazepine receptor. 25 It has also been revealed that this receptor is primarily distributed in the brain. Under non-pathological conditions, TP levels are very low in glial cells, but there is accumulating evidence that TP expression increases in parallel with microglial activation. Thus, an imaging technique that traces TP has become a method to quantify neuroinflammation.26,27 Elevated TP levels in peripheral blood have been reported to be highly associated with the severity and outcome of patients with acute ischemic stroke, acute intracerebral hemorrhage, spontaneous subarachnoid hemorrhage, and severe traumatic brain injury.28–31 Thus, TP is considered an inflammatory biomarker that reflects the level of brain injury. However, it is unclear if there is a relationship between circulating TP levels and POD. This study was designed to detect serum TP levels in a group of the elderly breast cancer patients who underwent a surgery, and to further investigate the ability of serum TP to predict POD.
Materials and methods
Study population
We performed this prospective, observational study at Yinzhou People’s Hospital, Ningbo, China between January 2014 and February 2018. The study cohort was composed of three groups of elderly individuals (age ≥65 years old) as follows: (1) elderly female patients with histologically confirmed breast cancer, (2) healthy elderly women (healthy controls), and (3) elderly women with benign breast diseases (benign controls). The exclusion criteria for the breast cancer patients were previous history of any type of cancer, stage 0 (in situ breast cancer) or stage IV disease (multiple cancers, metastatic disease at diagnosis, or distant organ metastasis), recent infection, and a documented history of neurological or psychological diseases (such as dementia, stroke, or delirium). The study protocol was formed based on the World Medical Association Declaration of Helsinki. This study was performed after approval by the ethics committee of Yinzhou People’s Hospital. Written informed consent to participate in the study was obtained from all participants or their relatives.
Assessments
The recorded information included demographic data (e.g., age and body mass index), medical comorbidities (modified Charlson’s Comorbidity Index), surgical risk (American Society of Anesthesiologists rating scale), tumor size, hormone receptor status, lymph node status, histologic grade, nuclear grade, and tumor-node-metastasis stage. Patients underwent radical mastectomy or modified radical mastectomy, and twice daily during the first 7 postoperative days, we used the Confusion Assessment Method32,33 to assess POD. Adjuvant treatments comprised radiotherapy, chemotherapy, and hormone therapy.
Measurements
Peripheral blood was drawn from patients via the antecubital vein between 7 and 8 AM 1 day preoperatively and on the first postoperative day. We also obtained blood samples from healthy individuals and controls with benign breast diseases. Blood samples were centrifuged at 3000 ×g, aliquoted, and frozen at −70°C until examination. Serum TP levels were quantified in duplicate using a specific enzyme-linked immunosorbent assay kit (Cloud-Clone Corp., Katy, TX, USA) in accordance with the manufacturer’s instructions. Every 3 months, a batch of samples was gauged by the same technician blinded to the patients’ clinical information using the same equipment. The minimum detectable level of TP was 0.127 ng/mL.
Statistical analysis
The statistical analysis software used in this study included IBM SPSS Statistics for Windows, version 19.0 (IBM Corp., Armonk, NY, USA) and MedCalc, version 9.6.4.0 (MedCalc Software, Mariakerke, Belgium). This study included two types of data, namely, categorical and continuous data. Categorical data are presented as counts (percentages) and were compared with the Chi-square test or Fisher’s exact test as appropriate. Continuous data were analyzed using the Kolmogorov–Smirnov or Shapiro–Wilk tests to assess the normality of distribution. Normally distributed data were presented as mean (standard deviation), and non-normally distributed data were reported as median (interquartile range [IQR]). Subsequently, a t test, one-way ANOVA, the Mann–Whitney U test, or the Kruskal–Wallis H test were performed for two- or multiple-group comparisons. Bivariate correlation analyses were performed using the Spearman rank correlation test or Pearson correlation test as appropriate; afterwards, a multivariate linear regression model was configured to discern variables that were independently associated with serum TP levels. We also constructed a binary logistic regression model to identify independent predictors of POD. In addition, the odds ratio (OR) and 95% confidence interval (CI) values were reported. Using the receiver operating characteristic (ROC) curve with estimated area under curve (AUC) and 95% CI values, the predictive value of serum TP levels for POD was evaluated and an optimal value was selected, which was used to generate the corresponding sensitivity and specificity values. A two-tailed P value of <0.05 was designated as the cutoff for statistical significance.
Results
Clinical characteristics of the participants
In this study, we enrolled 152 elderly women with histologically confirmed breast cancer, 152 healthy elderly women (healthy controls), and 152 elderly women with benign breast diseases (benign controls). There were no statistically significant differences among the three groups regarding age or body mass index. Among the breast cancer patients, the median age was 68 years (range: 65–78 years; IQR: 67–71 years) and the median body mass index was 25.2 kg/m2 (IQR: 23.2–27.3 kg/m2; range: 20.2–32.0 kg/m2). The median Modified Charlson’s Comorbidity Index was 1 (range: 0–2; IQR: 1–2), and the American Society of Anesthesiologists rating scale was I for 88 breast cancer patients and II for 64 patients. Tumor sizes were <2 cm in 80 patients and ≥2 cm in 72 patients. Ninety-four patients had tumor-node-metastasis stage I or II disease, and 58 patients had tumor-node-metastasis stage III disease. The lymph node status was negative in 69 patients and positive in 83 patients. The histologic grade was I or II in 77 patients and grade III in 75 patients. Nuclear grade I or II was revealed in 81 breast cancer patients, and 71 were found to be nuclear grade III. A total of 67 and 85 patients presented with negative and positive estrogen receptor status, respectively, and a negative and positive progesterone receptor status was found in 77 and 75 patients, respectively. Among the 152 total elderly breast cancer patients, 30 (19.7%) suffered from POD. The onset of POD ranged from 1 to 5 days after surgery (median: 2 days; IQR: 1–3 days).
Changes in serum TP levels
TP levels were undetectable in all serum samples from healthy controls and benign controls as well as in all preoperative serum samples from breast cancer patients (<0.127 ng/mL); thus, all of these samples were regarded as 0. Postoperative serum TP levels in the elderly breast cancer patients ranged from 0 (undetectable; 113 patients) to 2.209 ng/mL, with a median of 0 ng/mL and an IQR of 0 to 0.172 ng/mL. Obviously, TP levels were substantially higher in the postoperative serum samples from patients than in serum samples from healthy controls and benign controls as well as in preoperative serum samples from the same patients (all P <0.001).
As listed in Table 1, postoperative serum TP levels were closely correlated with tumor size, tumor-node-metastasis stage, lymph node status, histologic grade, nuclear grade, estrogen receptor status, progesterone receptor status, serum C-reactive protein levels, and serum D-dimer levels. Multivariate linear regression analysis showed that postoperative serum TP levels were independently associated with serum C-reactive protein levels (t = 4.062, P<0.001) (Figure 1).
Correlative analysis between postoperative serum translocator protein levels and other variables among elderly breast cancer patients.

Bivariate correlation was analyzed using Spearman rank correlation test.
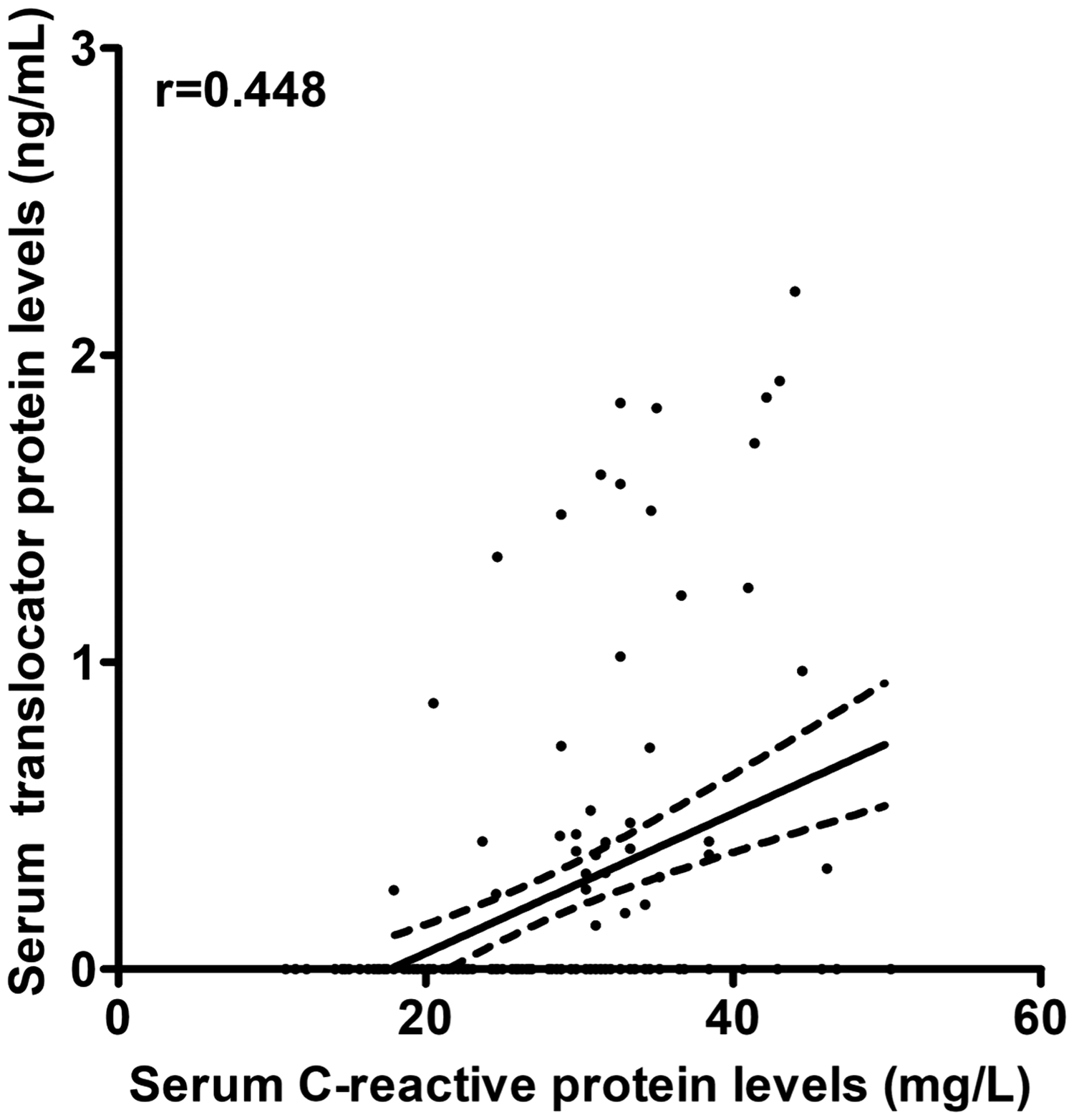
Relationship between postoperative serum translocator protein levels and serum C-reactive protein levels among elderly breast cancer patients.
POD prediction ability of serum TP levels
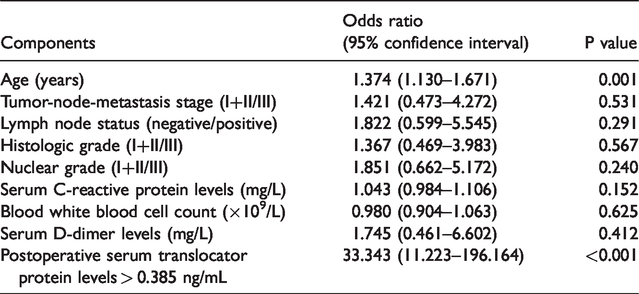
Postoperative serum TP levels were remarkably elevated in patients who developed POD compared with those who did not (Figure 2). Using ROC curve analysis, we found that postoperative serum TP levels exhibited a significantly high discriminatory ability for patients at risk of POD (Figure 3); moreover, a cutoff value of 0.385 ng/mL was found to differentiate between patients with a risk of developing POD and those without a risk of POD. This TP cutoff value presented a sensitivity of 70.0% and a specificity of 95.1%. As shown in Tables 2 and 3, compared with patients who did not present a risk of POD, those who developed POD tended to be older, were more likely to have an elevated tumor-node-metastasis stage and a positive lymph node status, were more prone to have an increased histologic and nuclear grade, had significantly increased serum C-reactive protein levels, white blood cell counts, and serum D-dimer levels, as well as substantially increased postoperative serum TP levels (>0.385 ng/mL). When these variables were incorporated into a binary multivariate logistic regression model, we found that age and postoperative serum TP levels >0.385 ng/mL were independently associated with the occurrence of POD (Table 4).
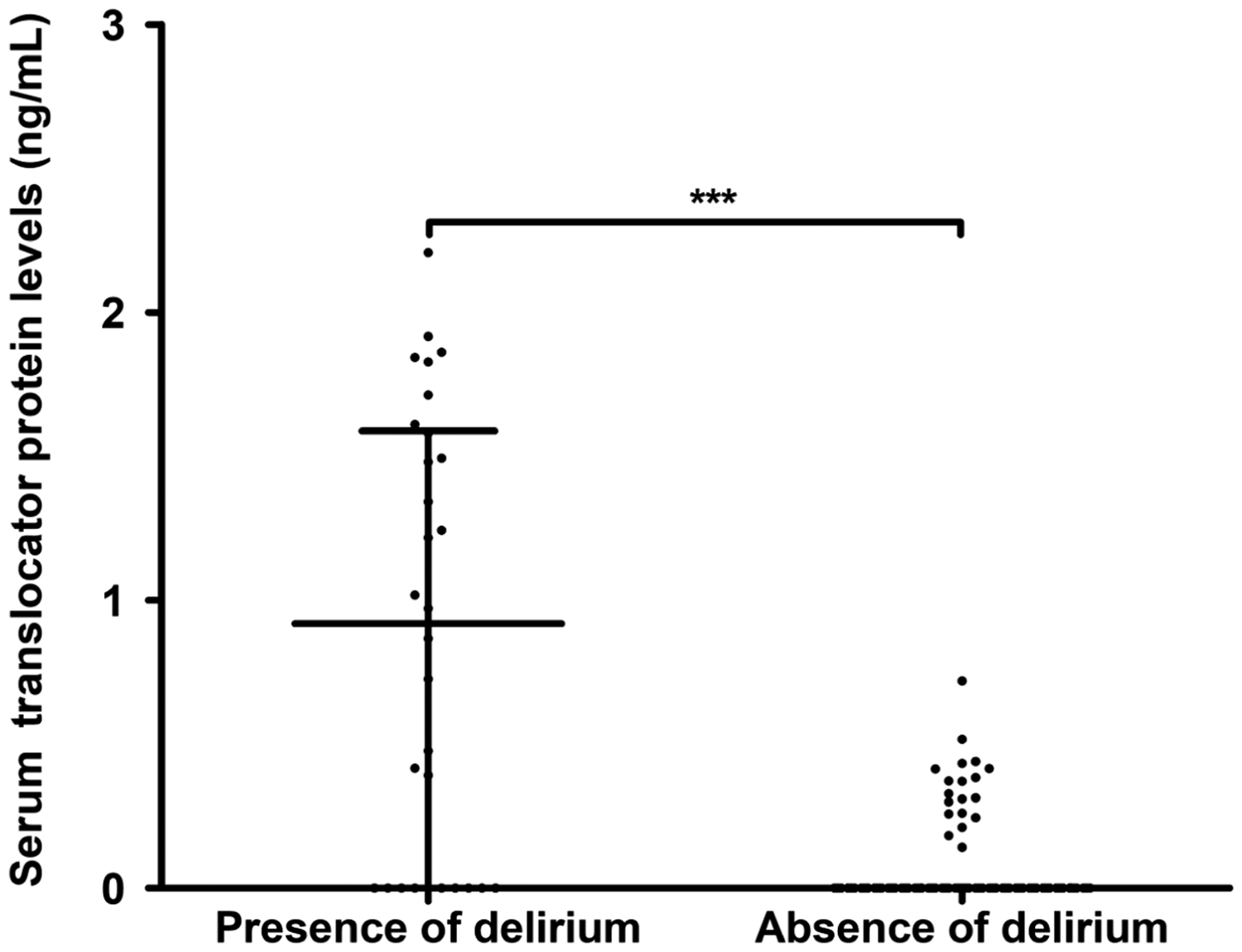
Comparison of serum translocator protein levels by postoperative delirium status after breast cancer surgery in elderly women.

Analysis of the predictive value of serum translocator protein levels for postoperative delirium among elderly breast cancer patients.
Comparison of demographic, clinical, and laboratory parameters by postoperative delirium status among elderly breast cancer patients.

Data are reported as median (interquartile range) or counts (percentage) as appropriate and were compared with the Mann–Whitney U test, chi-square test, or Fisher exact test as indicated. n denotes the number of patients.
Demographic, clinical, and laboratory parameters related to postoperative delirium in elderly breast cancer patients by univariate logistic regression analysis.

Factors associated with postoperative delirium in elderly breast cancer patients by multivariate logistic regression analysis.
Discussion
To the best of our knowledge, this is the first study to investigate serum TP levels in breast cancer patients with POD. Although many papers17–19 have reported POD cases in cancer, few reports have investigated POD in only breast cancer patients.20,21 Therefore, our data regarding POD in breast cancer are novel. The main findings of our study are that: (1) there was a 19.7% incidence rate of POD in this cohort of breast cancer patients; (2) compared with the serum from healthy controls and benign controls as well as preoperative serum from patients, TP levels were significantly increased in postoperative serum samples from patients; (3) postoperative serum TP levels were significantly higher in patients at risk of POD than in those not experiencing POD; (4) postoperative serum TP levels were independently correlated with serum C-reactive protein levels by multivariate linear regression analysis; (5) postoperative serum TP levels were highly predictive of POD; and (6) postoperative serum TP levels, which were identified as a categorical variable, in addition to age were the two independent predictors of POD in this cohort of breast cancer patients. Taken together, these findings suggest that TP could be an inflammatory biomarker that can distinguish POD in elderly breast cancer patients.
Although postoperative inflammatory brain injury is an important mechanism for the occurrence and development of POD,22–24 the biological functions of TP in the central nervous system remain to be explored. However, there is significant evidence that TP can be an inflammatory biomarker that reflects the inflammatory status of various acute brain injury diseases, such as acute intracerebral hemorrhage, ischemic stroke, acute traumatic brain injury, and spontaneous subarachnoid hemorrhage.28–31 This study showed that postoperative serum TP levels were significantly elevated compared with preoperative serum TP levels in breast cancer patients and fasting serum TP levels in healthy and benign controls. Intriguingly, serum C-reactive protein levels were also independently correlated with postoperative serum TP levels after correcting for other possible confounding factors, such as tumor size and histological type. These results indicated that postoperative brain injuries might exist in breast cancer patients.
In this study, we found that the POD incidence of breast cancer patients was 19.7%. Disappointingly, owing to the paucity of previous data regarding POD in breast cancer patients, we could not make a comparison of the POD incidence from previous reports. The other finding of this study was that postoperative serum TP levels were significantly raised in patients at high risk of POD compared with patients who did not suffer from POD. We hypothesize that neuroinflammation might be a factor that results in POD in breast cancer patients. The reasons for neuroinflammation causing POD may include intraoperative ischemic and hypoxic brain injury, to which the elderly are increasingly susceptible;34–37 however, the actual pathogenesis of POD needs to be explored in future studies of breast cancer patients.
In this study, we further clarified the predictive value of serum TP levels for POD in this group of cancer breast patients. In accordance with the AUC (0.823), serum TP levels had a medium-high predictive value for POD. Using a multivariate logistic regression analysis, age and serum TP levels were highly associated with POD among breast cancer patients. Clearly, age is the most relevant determinant for POD in a variety of diseases.38–40 Thus, it would be interesting for serum TP levels to be an independent predictor for POD only in elderly breast cancer patients. This interpretation is based on TP being a well-known candidate for neuroinflammation.26,27 Although such an explanation needs to be verified in a larger cohort, this finding might indicate that serum TP could be used as a neuroinflammatory biomarker to predict POD in elderly breast cancer patients.
In conclusion, our data showed that increased postoperative serum TP levels were closely associated with serum C-reactive protein levels and independently predicted POD among elderly women with breast cancer. Serum TP levels exhibited a high discriminatory capability, which substantialized postoperative serum TP as a promising inflammatory biomarker to distinguish elderly breast cancer patients who are at risk of POD.
Abbreviations
AUC, area under curve; CI, confidence interval; IQR, interquartile range; OR, odds ratio; POD, postoperative delirium; ROC, receiver operating characteristic; TP, translocator protein.
Footnotes
Acknowledgements
The authors thank all of the staff from the Department of Thyroid Gland and Breast Surgery, Yinzhou People’s Hospital (Ningbo, China) for their technical support.
Data availability statement
The data that support the findings of this study are available upon request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.