
Abstract
Timely recognition of the characteristic electrocardiographic pattern of de Winter syndrome is important for providing immediate reperfusion therapy for acute anterior myocardial infarction. In this case, an electrocardiogram showed 1- to 3-mm upsloping ST-segment depression at the J point in leads V1 to V6, with loss of R wave progression in leads V1 to V4. Urgent angiography showed occlusion of the proximal left anterior descending coronary artery and 70% stenosis in the ostial first diagonal branch (Medina type 1.1.1.). For this bifurcation lesion, we successfully performed a modified jailed-balloon technique to protect the side branch during percutaneous coronary intervention stenting. Thereafter, thrombolysis in myocardial infarction 3 flow was restored in both branches. This modified jailed-balloon technique is safe and effective in stent placement for de Winter syndrome without any loss of side branches.
Keywords
Introduction
De Winter syndrome, also termed anterior ST-segment elevation myocardial infarction equivalent, refers to a rare clinical condition with occlusion of the proximal left anterior descending (LAD) coronary artery and no ST-segment elevation.1,2 This syndrome only occurs in 2% to 3% of patients with acute anterior myocardial infarction and is under-recognized by clinicians. 3 Patients with this syndrome present with a characteristic electrocardiographic (ECG) pattern, which shows a 1- to 3-mm upsloping ST-segment depression at the J point in leads V1 to V6. This is followed by tall and positive symmetrical T waves, loss of precordial R wave progression, and 1- to 2-mm ST-elevation in lead aVR. Rapid recognition of the ECG pattern followed by appropriate emergency percutaneous coronary intervention (PCI) reperfusion therapy is important for improving the clinical outcomes of these patients. 4 We report a typical case of a patient with de Winter syndrome who received successful stenting for a bifurcation lesion of the LAD coronary artery. Our findings will hopefully help physicians rapidly recognize the diagnostic features of the ECG pattern in this condition and ensure appropriate emergency reperfusion therapy.
Case report
A 45-year-old male smoker with hypercholesterolemia was admitted to the Emergency Department with acute compressive chest pain of 1.5 hours in duration. He was conscious on admission. A physical examination showed a heart rate of 79 bpm and a blood pressure of 100/70 mm Hg. An ECG showed 1- to 3-mm upsloping ST-segment depression at the J point in leads V1 to V6, with loss of R wave progression in leads V1 to V4 (Figure 1). Such an ECG profile suggested de Winter syndrome. Ultrasound cardiography showed left ventricular segmental wall motion abnormality and a depressed left ventricular ejection fraction of 49%. This study was approved by the Tianjin Chest Hospital Review Board and written informed consent for publication was obtained from the patient.

Electrocardiogram showing 1- to 3-mm upsloping ST-segment depression at the J point in leads V1 to V6, with loss of R wave progression in leads V1 to V4.
Urgent coronary angiography showed complete occlusion of the proximal LAD coronary artery, with diffuse calcification and 70% stenosis in the ostial first diagonal branch (Medina type 1.1.1., Figure 2a). For this bifurcation lesion, there was a high risk of side branch (SB) occlusion during stenting of the main branch (MB). We used a modified jailed-balloon technique (M-JBT) to protect the SB during MB stenting. A jailed balloon (2.0 × 20 mm) was carefully placed into the SB with an adequate length of balloon advanced to cannulate the ostium. A drug-eluting stent (3.0 × 25 mm) was then advanced into the MB covering the target lesion. The stent in the MB was inflated at 8 atm and the jailed-balloon in the SB was not inflated (Figure 2b, c). Arterial blood flow was re-established. The SB balloon was removed and the MB stent was then fully expanded with 14 atm. During final angiography, we confirmed thrombolysis in myocardial infarction (TIMI) 3 flow in the MB and SB (Figure 2d), and then finished the procedure. The de Winter ECG pattern disappeared (Figure 3). A subsequent 8-month follow-up was uneventful.

Coronary angiography showing the modified jailed-balloon technique for de Winter syndrome. (a) Left anterior descending artery (MB) occlusion and 70% stenosis in the ostial first diagonal branch (SB; Medina type 1.1.1.). (b) A jailed-balloon (2.0 × 20 mm) was advanced into the SB to project the ostium. A stent (3.0 × 25 mm) was positioned over the target lesion in the MB. (c) The MB stent was inflated to 8 atm. (d) No residual stenosis in the MB after stenting was observed. Thrombolysis in myocardial infarction 3 flow was established in the MB and SB. (e and f) Follow-up angiography at 2 and 8 months. MB: main branch; SB: side branch.

An electrocardiogram performed after stent placement with a modified jailed-balloon technique showing improved ST-T waves. The typical de Winter pattern has disappeared.
The patient received aspirin (300 mg) and clopidogrel (600 mg) before PCI. During PCI, an intra-arterial bolus of unfractionated heparin was administered at 70 to 100 IU/kg. 5 The patient was discharged with dual antiplatelet therapy (aspirin 100 mg/day and clopidogrel 75 mg/day) and closely followed with hospital visits three times at 2, 5, and 8 months after PCI. Coronary angiography was undertaken and showed good flow (TIMI 3) in the LAD coronary artery (MB) and in the first diagonal branch (SB) at 2 and 8 months, respectively (Figure 2e, f). The left ventricular ejection fraction, left ventricular end-diastolic diameter, N-terminal pro-B type natriuretic peptide levels, and low-density lipoprotein cholesterol levels were monitored for 8 months. These variables showed excellent immediate and long-term clinical outcomes (Figure 4).
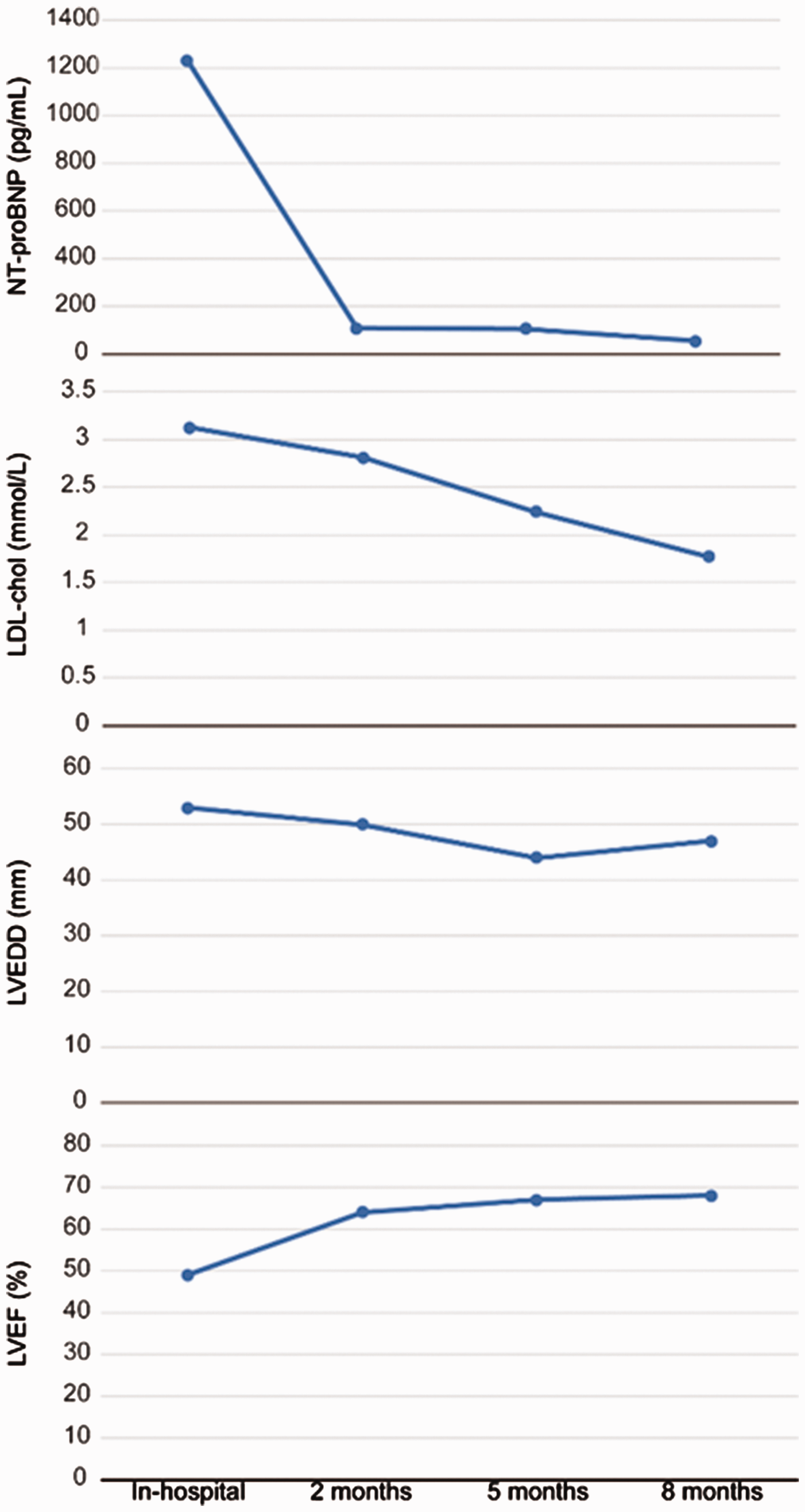
Graphs showing LVEF, LVEDD, NT-proBNP levels, and LDL-chol levels during the in-hospital stay and at an 8-month follow-up. LVEF: left ventricular ejection fraction; LVEDD: left ventricular end-diastolic diameter; NT-proBNP: N-terminal pro-B type natriuretic peptide; LDL-chol: low-density lipoprotein cholesterol.
Discussion
Substantial chest pain and acute anterior myocardial infarction caused by LAD coronary artery occlusion are associated with de Winter syndrome. Patients with a de Winter ECG pattern are young and require immediate mechanical reperfusion therapy for complete resolution of ST-T waves. 6 However, this syndrome is often under-recognized or not treated as an ST-segment elevation myocardial infarction equivalent by clinicians. Therefore, de Winter syndrome is accompanied by increased morbidity and mortality rates.
Timely recognition of the ECG pattern in patients with de Winter syndrome and immediate transfer to a PCI center for mechanical reperfusion therapy avoid potential delay of treatment and improve clinical outcomes of these patients. In the current case, we rapidly recognized the particular ECG pattern of de Winter syndrome to ensure immediate, successful reperfusion treatment. The patient arrived at the hospital by 1.5 hours after onset of symptoms. Additionally, the door-to-balloon time was only 45 minutes because of use of an M-JBT for the bifurcation lesion. The patient suffered from a proximal LAD occlusion (MB) and 70% stenosis in the ostial first diagonal branch (SB), which was defined as Medina type 1.1.1. There was a high risk of SB branch occlusion during MB stenting. In this case, use of an M-JBT was effective for protecting SB patency and restoring SB flow to TIMI 3 after PCI stenting. In our M-JBT, the jailed-balloon in the SB was not inflated during the whole PCI procedure. Our M-JBT does not induce severe dissection of the SB, plaque shifting, or MB stent deformation compared with the conventional jailed-balloon technique (both the stent and jailed-balloon are inflated). Therefore, we successfully treated the bifurcation lesion for our patient with de Winter syndrome without any loss of the SB.
Conclusion
We recommend using an M-JBT during PCI stenting for patients with de Winter syndrome and bifurcation lesions. This technique is safe and effective for preserving SB patency during MB stenting.