
Abstract
de Winter syndrome, also termed anterior ST-segment elevation myocardial infarction (STEMI) equivalent, is estimated to be present in approximately 2% of patients with acute myocardial infarction, but is often under-recognized by clinicians. Therefore, de Winter syndrome is associated with increased morbidity and mortality. We report a 51-year-old man with typical chest tightness and a characteristic electrocardiographic pattern without classic ST-segment elevation, but with acute nearly total occlusion of the left anterior descending coronary artery. Although the patient presented as a non-STEMI case, the definite diagnosis of de Winter syndrome was made on the basis of clinical and electrocardiographic findings. The patient’s symptom of chest tightness was relieved immediately after acute percutaneous coronary intervention and the left ventricular ejection fraction had not deteriorated at 1 month of follow-up.
Keywords
Introduction
Current guidelines define ST-segment elevation myocardial infarction (STEMI) as a clinical syndrome characterized by typical symptoms of myocardial ischemia in association with typical ST-segment elevation on an electrocardiogram (ECG) and subsequent release of biomarkers of myocardial necrosis. 1 However, ECG abnormalities other than ST-segment elevation may indicate transmural myocardial infarction. 2
In 2008, de Winter et al. 3 recognized a characteristic ECG pattern in 30 of 1532 patients with anterior myocardial infarction, which suggested proximal left anterior descending (LAD) coronary artery occlusion as follows. (1) There were tall and positive symmetrical T waves in leads V1 to V6 following 1 to 3-mm upsloping ST-segment depression at the J point. (2) Non-widened or only slightly widened QRS complexes were observed. (3) Precordial R wave progression might disappear. (4) In most patients, there was a 1- to 2-mm ST elevation in lead aVR. The positive predictive value of this ECG pattern is 100%; therefore, this strongly suggests the clinical diagnosis of de Winter syndrome.
Recognition of characteristic ECG changes associated with acute occlusion of a coronary artery guides decisions about reperfusion therapy. In China, improving the capacity of discriminating this rare ECG pattern is important because such patients must be provided emergency revascularization. We report here a man with typical chest tightness and a characteristic ECG pattern without classic ST-segment elevation, but who had acute nearly total occlusion of the LAD coronary artery. Although the patient presented as a non-STEMI case, the definite diagnosis of de Winter syndrome was made by clinical and ECG findings.
Case presentation
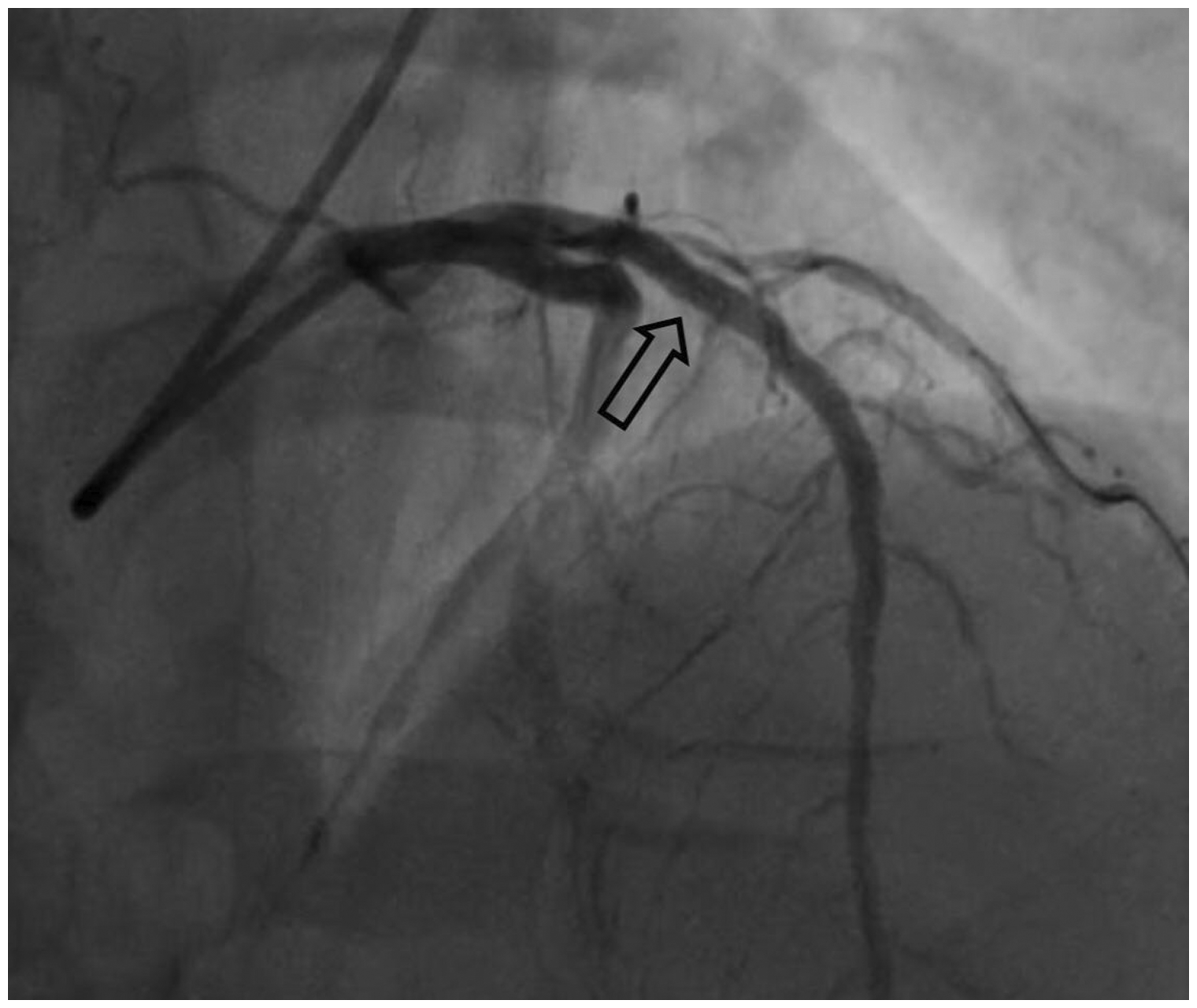
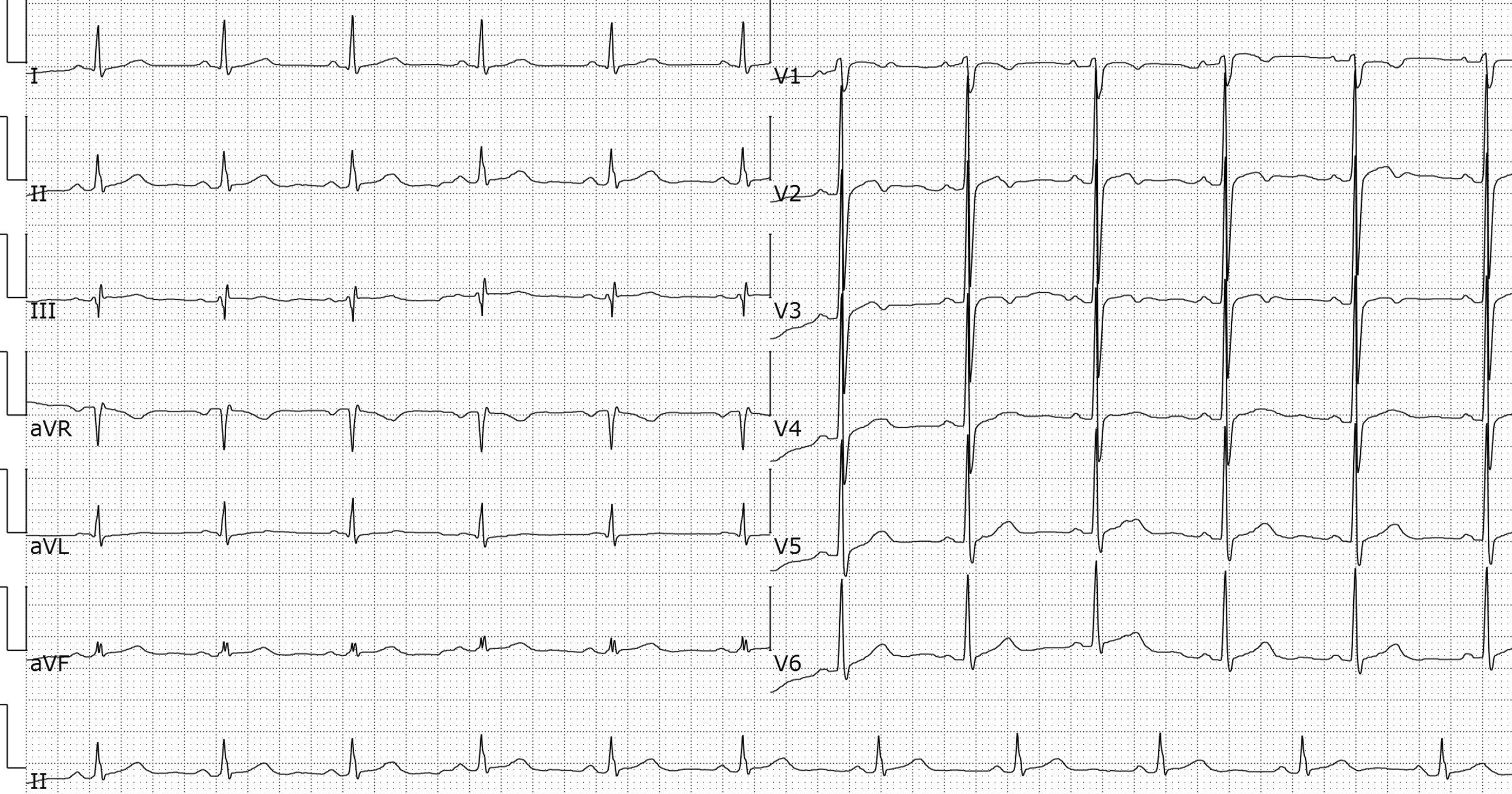
A 51-year-old man presented to our Emergency Department with chest tightness that had been ongoing for 5 hours. The patient had a well-controlled history of hypertension for longer than 1 year by taking amlodipine and metoprolol. His vital signs on admission were a blood pressure of 132/93 mmHg, heart rate of 97 beats/minute, and respiratory rate of 18 breaths/minute. ECG showed 1- to 2-mm upsloping ST-segment depression in the precordial leads, with tall and positive symmetric T waves, loss of precordial R wave progression, and a small ST-segment elevation (0.5 mm) in lead aVR (Figure 1). However, the troponin I level at presentation was negative. Bedside transthoracic ultrasound showed mild tricuspid and mitral valve regurgitation with an overall left ventricular ejection fraction (LVEF) of 60%. In the next 30 minutes, ongoing ECG monitoring showed a similar static pattern, without evolving to precordial ST-segment elevation. These ECG changes suggested de Winter syndrome, which is a condition associated with acute occlusion of the LAD coronary artery and no ST-segment elevation. Dual antiplatelet therapy with aspirin and a direct-acting P2Y12 receptor inhibitor (clopidogrel) was provided in the Emergency Department. Urgent coronary angiography showed nearly complete occlusion of the proximal LAD coronary artery (Figure 2), which was then successfully treated with angioplasty and two drug-eluting stents (Figure 3). After angiography, the cardiac troponin I level rose to a peak of 0.76 ng/mL. One month later, outpatient ECG showed sinus rhythm with mild T wave changes in the anterior wall (Figure 4). Repeated transthoracic cardiac ultrasound showed that the overall LVEF was improved to 72.3%.

Electrocardiogram showing 1- to 2-mm upsloping ST-segment depression in the precordial leads of a 51-year-old man who presented with substantial chest tightness. There are tall and positive symmetric T waves, loss of precordial R wave progression, and small ST-segment elevation in the aVR lead.

A left coronary angiogram shows complete occlusion of the proximal left anterior descending coronary artery (arrow).
An angiogram showing that blood flow is restored after successful treatment with angioplasty and two drug-eluting stents of the left anterior descending coronary artery (arrow).
Outpatient follow-up electrocardiogram shows sinus rhythm with mild T wave changes in the anterior wall.
Discussion
ST elevation and ST depression are suggestive of myocardial ischemia/infarction. 4 With regard to ST depression, horizontal and down-sloping ST depression might be of greater clinical significance, while upsloping ST depression is often ignored. However, in the de Winter ECG pattern, upsloping ST depression in the precordial leads is an ECG finding that is highly indicative of acute myocardial infarction. Therefore, this ECG finding indicates occlusion of the proximal LAD coronary artery, which requires urgent reperfusion therapy. If this therapy is not performed, patients are prone to serious adverse cardiovascular events. Consequently, the de Winter ECG pattern is regarded as equivalent to STEMI. 5 Nevertheless, the definite electrophysiological mechanisms involved in ECG changes of de Winter syndrome have not been fully determined. Verouden et al. 6 proposed a theory that, because of the large transmural ischemia in de Winter syndrome, cardiac injury currents are directed upwards to the standard aVR lead, rather than generated towards the precordial leads. One theory for the de Winter ECG pattern may be related to a delay in endocardial conduction in an anatomical variant of the Purkinje fibers. 2 Another explanation might be that a mutation of sarcolemmal K-ATP channels prevents elevation of the ST segment. 7 Although the de Winter ECG pattern does not always indicate proximal LAD coronary artery occlusion, 8 identifying this ECG pattern early and preventing a delay in definite management are still important.
In conclusion, data on the ECG pattern associated with de Winter syndrome are limited. There are currently no reports or recommendations in any Chinese guidelines on management of de Winter syndrome, probably because of the lack of reports. Our case showed typical chest tightness and a de Winter ECG pattern (upsloping ST depression and prominent T waves in the precordial leads, while ST elevation in the aVR lead of 0.5 mm was observed). Urgent coronary angiography showed nearly complete occlusion of the LAD coronary artery in this patient, who was successfully treated via mechanical reperfusion therapy and stenting. We hope that our findings can add evidence to the literature on the optimal clinical diagnosis and treatment of similar patients. Early recognition of the de Winter ECG pattern in patients and timely reperfusion therapy are important to avoid further myocardial necrosis and improve the clinical prognosis of these patients.
Footnotes
Ethics statement
Written approval was obtained from the local Ethics Committee of Sir Run Run Shaw Hospital (approval no.: 20210422044303538) for reporting of this case. Verbal consent was obtained from the patient for publication of this case.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.