
Abstract
Pulmonary sequestration is a rare congenital lung anomaly that is characterized by a nonfunctioning pulmonary parenchyma, which typically lacks connection to the tracheobronchial airways, and thus has an anomalous systemic blood supply. Here we report the case of a 37-year-old man who was diagnosed with pulmonary sequestration and also presented with high levels of the serum tumor marker cancer antigen 125 (CA125). Computed tomography of the chest indicated the presence of a heterogeneous mass with low attenuation in the right S10 region that had a single aberrant artery supplying blood from the descending aorta. The patient eventually underwent thoracoscopic surgery with resection of the right sequestrated lung. Immunohistochemistry showed positive staining for CA125 in bronchial epithelial and epithelioid cells. After surgery, CA125 levels returned to the normal range. In summary, this report describes a case of pulmonary sequestration associated with elevated serum CA125 levels, and further provides relevant literature for this presentation.
Keywords
Introduction
Pulmonary sequestration is a congenital disorder that typically evolves from an abnormal caudal accessory budding of the foregut. This condition can lead to dissociation from the tracheobronchial tree and consequently, retention of the embryonic arterial supply system. 1 As a result, a single nonfunctional mass of lung tissue will receive no arterial blood from the pulmonary circulation but instead, blood is supplied from the systemic circulation. 2 This pulmonary malformation is usually classified into two types: intralobar or extralobar sequestration. Intralobar pulmonary sequestration shares the visceral pleura with an otherwise normal pulmonary lobe, while extralobar pulmonary sequestration is separated from normal lung tissue by its pleural covering. 3
Cancer antigen 125 (CA125), which is also known as mucin 16 (MUC16), is a cell surface glycoprotein with a high molecular weight (∼152 kDa). CA125 is expressed in various mesothelial-derived tissues, but it has also been identified in tissues of non-mesothelial origin, such as the tracheobronchial epithelium, stomach, and kidney. 4 Serum CA125 levels are typically increased in malignancies such as ovarian and lung cancer, but can also be increased in some benign chronic diseases. 5 Previous studies have reported that levels of certain tumor markers may be elevated in patients with intralobar pulmonary sequestration.6,7 However, a case of pulmonary sequestration with elevated CA125 alone has not been reported. Here, we characterize the first case of pulmonary sequestration with increased serum CA125 levels and further analyze the impact of this correlation in the context of the current literature.
Case report
A 37-year-old Chinese man was admitted to the Xuanwu Hospital Capital Medical University (Beijing, China) with the major complaints of coughing and mild fever for 2 weeks, with daily expectoration of yellow or white sputum. The patient was a non-smoker and also denied use of alcohol or any illicit drugs. The patient also presented with a medical history of recurrent pneumonia during childhood. During chest auscultation, a few moist rales were audible from basilar areas of the right back. Chest X-ray analysis showed a large opaque area in the lower right lobe, with a slightly blurred edge. Chest radiography was not improved after intravenous administration of 2.0 g cefminox twice daily for 7 days. Tests of liver and renal function, blood cell counts, and coagulation tests were normal. Both sputum culture and acid-fast staining were negative. Galactomannan and β-D-glucan detection, latex agglutination, and a T-SPOT test for tuberculosis were also negative. Remarkably, laboratory analysis of tumor markers in the patient’s serum showed a significant increase in CA125 levels (Table 1).
Laboratory examination of tumor markers.

CA125, cancer antigen 125; CA199, cancer antigen 199; CEA, carcinoembryonic antigen; NSE, neuron-specific enolase; CYFRA21-1 cytokeratin 19 fragment; PSA, prostate-specific antigen; FPSA, free prostate-specific antigen.
After admission, a chest computed tomography (CT) examination was performed. The CT scan showed a heterogeneous mass in the right S10 region that was scattered in the low attenuation area. A single systemic artery provided vascular supply from the descending aorta (Figure 1, arrow), while venous drainage was via the pulmonary venous system. The patient was diagnosed with right intralobar pulmonary sequestration and eventually underwent thoracotomy to remove the right sequestrated lung (measured size of the mass = 12 × 6×3 cm3). Epithelioid cells, lymphocytes, and polynuclear giant cells were visualized in the mucus-containing dilated bronchi by standard microscopy (Figure 2). Immunohistochemical staining of the sequestrated lung showed positive staining for CA125 in some area of bronchial epithelial cells and epithelioid cells (Figure 3).

Computed tomography scan of the patient’s chest. The imaging revealed a single systemic artery (white arrow) that provided vascular supply from the descending aorta.

Microscopic findings of the sequestrated lung. Epithelioid cells, lymphocytes, and polynuclear giant cells were detected in the mucus-containing dilated bronchi (hematoxylin and eosin staining; scale bars = 200 µm).

Immunohistochemical staining for CA125 in some area of bronchial epithelial cells (a) and epithelioid (b) cells (scale bars = 200 µm). CA125, cancer antigen 125.
After surgery, the patient was discharged according to standard procedures. No further treatments were administered after discharge. Six months after surgery, the patient was clinically re-assessed and no post-surgical complaints were noted. A set of exams to evaluate whole blood cell counts, liver and kidney function, coagulation function, and other indicators were also performed. All test results were within the normal range. Additionally, CA125 levels were within the normal range (14.08 U/mL).
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. Ethics approval was not applicable because there was no special treatment for the patient.
Discussion
The pathogenesis of pulmonary sequestration involves the development of a distinctive lesion within part of the lung tissue during embryogenesis. The affected region lacks respiratory function and typically shows an aberrant arterial supply from the systemic circulation. 8 In this case, the arterial supply came mostly from the aorta or one of its large branches. Intralobar pulmonary sequestration is more common than extralobar pulmonary sequestration and typically occurs in patients with a history of recurrent infections of the respiratory tract, hemoptysis, pleural effusion, or dyspnea. 9 A chest CT may reveal a solid or fluid (cystic) lesion in the lower lobes that involves the posterior basal segment. Intralobar sequestration accounts for 75% of all pulmonary sequestrations and has the same incidence in men and women. 10
CA125 is a biomarker for the differential diagnosis of pelvic masses. Dramatic increases in serum CA125 titers have also been reported in benign lung lesions, such as tuberculosis, 11 non-tuberculous mycobacteria, 12 interstitial lung disease, 13 silicosis, 14 lymphangioleiomyomatosis, 5 sarcoidosis, 15 thoracic endometriosis, 16 pulmonary alveolar proteinosis, 17 and bronchogenic cyst of the esophagus 18 (Table 2). In some of these diseases, CA125 levels may be associated with the clinical course of the disease. Measuring CA125 levels has also been used to monitor treatment outcomes.11,14
Examples of pathological conditions that feature elevated CA125 levels.
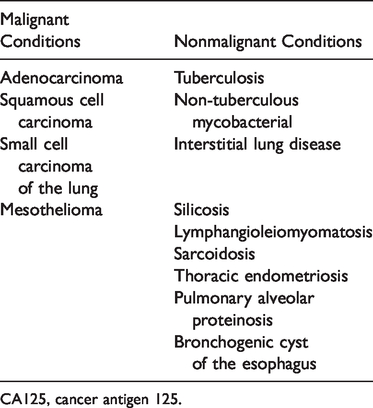
CA125, cancer antigen 125.
Pulmonary sequestration is poorly studied for such a frequent condition and an association with serum CA125 levels has rarely been reported. To better assess this case, we performed a literature search of the PubMed database (NCBI, Bethesda, MD, USA) to identify related published works, using “pulmonary sequestration” and “CA125” as keywords. We found six clinical cases (including ours), which are summarized in Table 3.1,6,19–21 All the described patients with intralobar pulmonary sequestration, including four women and two men (n = 6), had ages ranging between 34 and 44 years old. Serum CA125 levels ranged from 50.3 to 185.7 U/mL. After surgery, all patients recovered serum CA125 values to the normal range. Some patients presented CA125-positive sequestrated lung tissue by immunohistochemical staining, suggesting that pulmonary sequestration could lead to elevated serum CA125 levels.
Current literature that has correlated increased CA125 levels with pulmonary sequestration.
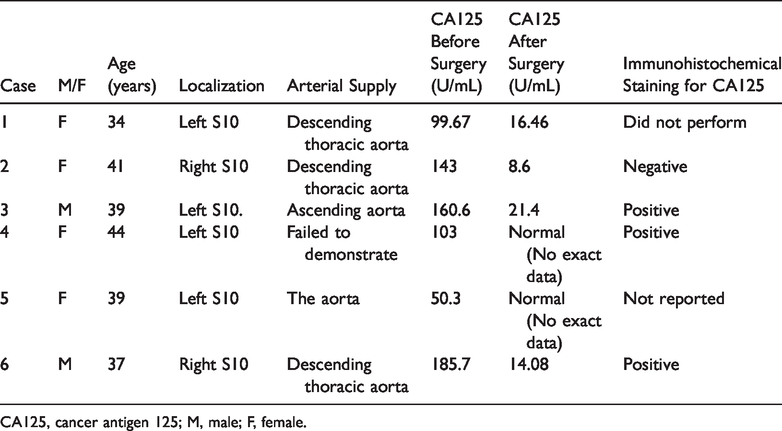
CA125, cancer antigen 125; M, male; F, female.
The reasons for increased CA125 levels in pulmonary sequestration patients remain controversial. Pulmonary sequestration is considered a childhood disease and, as such, is rarely diagnosed during adulthood. We found that all patients with pulmonary sequestration accompanied by increased CA125 levels were >34 years old. No reports of elevated CA125 levels in infants or adolescents with pulmonary sequestration have been described. We hypothesize that elevated CA125 in pulmonary sequestration patients may be caused by long-term stimulation of the sequestrated lung, as in up to several decades. Various stimulating factors may promote a sequestrated lung to secrete CA125, of which chronic inflammation may be the primary factor. It has been reported that under benign conditions, serum CA125 is elevated in response to inflammation. A significant positive correlation has been also observed between serum CA125 levels and the inflammation markers erythrocyte sedimentation rate and C- reactive protein in silicosis. 14 Increased serum CA125 levels are also positively correlated with serum TNF‐Ρ, IL‐6, and IL‐10 levels in patients with chronic heart failure. 22 Because patients with pulmonary sequestration tend to be associated with recurrent infections of the isolated lung tissues (including bacteria and fungi), the stimulation from this chronic inflammation may drive the elevation in CA125 levels. Therefore, upon surgical removal of the diseased lung tissue, this persistent stimuli might disappear, consequently restoring CA125 levels to a normal range.
Conclusion
Pulmonary sequestration can lead to elevated levels of serum CA125. An in-depth characterization of the putative inflammatory stimuli that are responsible for increased CA125 levels in this disease is warranted in future investigations.