
Abstract
Objective
Using the Twente Medical Systems international B.V. (TMSi) electromyography (EMG) system, active signal shielding was applied to clean signals and create data without interference and cable movement artifacts. TMSi, used in high-density surface EMG pattern recognition, controls myoelectric rehabilitation robots, yet few have studied how active signal shielding influences pattern recognition. This study aimed to investigate how active signal shielding used within the TMSi influenced motion pattern recognition.
Methods
Surface EMG of dominant side forearm and hand muscles was studied in eight healthy participants. The common component’s influence was accessed by the classification performance of wrist and hand functional movements.
Results
The classification performance of EMG signals with the common component was obviously lower than signals without the common component using one to five electrodes. Conversely, a higher motion classification performance was achieved using signals with the common component using over 12 electrodes. Optimal channel distribution was examined based on the sequential feed-forward selection method, showing that the common component affected the optimal channel location.
Conclusions
Active signal shielding in the TMSi improved classification accuracy in motion pattern recognition when over 12 electrodes were used. The optimal channel distribution was related to the common component when using the TMSi.
Keywords
Introduction
Surface electromyography (EMG), which represents the electrical activity of muscles, has been frequently used to control myoelectric prostheses, assistive skeletons, and rehabilitation robots for many years.1–3 In recent years, surface EMG with a large number of recording electrodes [or high-density (HD) surface EMG] technology has been developed and combined with pattern recognition analysis to assess myoelectric control. Previous studies show that satisfactory classification accuracies can be achieved from several different movements using HD surface EMG signals.4,5 However, surface EMG recordings often have low signal-to-noise ratios (SNRs) due to noise contamination that hinders the classification accuracy of fine movements. 6 A special design called active signal shielding technology has been applied to clean signals to remove interference and cable movement artifacts. In Refa and Porti EMG recording systems, 7 all EMG recording channels are amplified against the common component, which is defined as the average value of surface EMG signals in all connected inputs. Refa and Porti EMG recording systems are widely applied in HD surface EMG pattern recognition to control myoelectric rehabilitation robots.3,5,8 Despite encouraging applications using HD surface EMG recording, few have studied the influence of the reduced common component on classification accuracy in pattern recognition when using these EMG recording systems.
In addition, the data processing is time consuming and impractical for clinical implementation when using a large number of electrodes. Thus, most of the previous studies suggested that several appropriate EMG channels and the optimal placement locations of electrodes should be selected for practical myoelectric control instead of using all channels.9–11 A previous study using the Twente Medical Systems international B.V. (TMSi) system demonstrated that the determination of the appropriate number of EMG electrodes and their locations were affected by both participant specifics and different feature sets. 11 However, few studies have reported the influence of the reduced common component on the optimal placement locations of electrodes in pattern recognition when using the TMSi recording system.
The purpose of this study was to assess the effect of the common component on the classification accuracy and optimal placement locations of electrodes in pattern recognition with healthy participants. We examined whether the classification accuracy would be affected by the common component using a different number of optimal channels. Furthermore, the optimal electrode locations of the surface EMG signals with or without the common component were compared, which can potentially help to select the suitable electrode number and location for pattern recognition when using the system to reduce the common component.
Materials and methods
Participants
Eight healthy volunteers (one female and seven males) without known neuromuscular disorders volunteered to participate in the study. The study was approved by the Committee for the Protection of Human Subjects at the University of Texas Health Science Center at Houston and TIRR Memorial Hermann Hospital (Houston, TX, USA). All procedures conformed to the Declaration of Helsinki, and all participants signed the informed consent prior to any experimental procedures.
Description of the common component problem
In the TMSi EMG recording system, active signal shielding technology was applied to clean signals and remove interference and cable movement artifacts. As an introduction of the TMSi system, the mean value, which was defined as the common component (x
common
), can be written as:
7

Experiment protocols
Each participant was seated upright in a height-adjustable chair with the right forearm resting on a customized apparatus. The wrist was held naturally, the elbow joint was flexed approximately 90°, and the shoulder was slightly abducted (45°) and flexed (30°). Prior to the EMG recording, the skin treatment was prepared by cleaning the superficial skin with adhesive paste to ensure good contact and low baseline noise, and the skin was then cleaned with water after removing the remains. In the experiment, each participant was asked to use the right arm to perform seven wrist and hand functional movements, including the sphere grip, key pinch, fine pinch, hand opening, thumb extension, OK sign, and three-finger extension (Figure 1).

Seven wrist and hand functional movements.
Each participant was then asked to maintain each movement for 6 s with moderate force and to repeat this eight times. A 10-s rest period was allowed between two movements in a trial. In addition, to avoid muscle fatigue, each participant was allowed sufficient rest between trials.
EMG acquisition
HD surface EMG signals consisting of 58 channels were collected from the forearm and hand muscles of each healthy participant. Among all of the 58 electrodes, 48 electrodes were placed in a 6 × 8 grid formation over the forearm (Figure 2). Eight electrodes in each row were equally spaced and secured with medical tape as a round group. Six round groups were attached parallel around the forearm at different locations from approximately 12.5% to 75% for every 12.5% of the entire distance from the medial epicondyle of the humerus to the ulnar styloid. In addition, nine electrodes were placed on hand muscles, with every three electrodes targeting the first dorsal interosseous (FDI) muscles, the thenar muscles, and the hypothenar muscles, respectively. In the experiment, a single electrode defined as the reference electrode was connected in the 58th channel and placed on the ulnar styloid to record the negative value of the common component.

An example of the electrode locations for a 58-channel surface EMG recording.
A ground electrode in the Refa 136 system was placed on the ulnar styloid. A single reference electrode, which was connected to the 58th channel as mentioned above, was placed beside the ground electrode on the ulnar styloid to record the common component signals. The surface EMG signals were recorded and amplified by the Refa 136 EMG Recording System (TMS International BV, the Netherlands). The sampling rate was 2048 Hz per channel, and a band pass filter was set for 20 to 500 Hz.
Data analysis
Prior to the analysis, potential power line interference in the surface EMG data were eliminated by a spectrum interpolation algorithm. 12 The onset and offset of each movement segment were marked by experienced researchers manually and simultaneously applied to all 57 channels. The data analysis consisted of two stages.
The first stage generated the required datasets from the Refa 136 data for common component analysis. First, the signal from the reference channel, which was considered to be the negative value of the common component, was subtracted from each channel to recover the original surface EMG signals. Second, when considering several represented channels for clinic practice other than the entire channel set (which is necessary owing to optimal channel selection, as introduced below), the common component of several channels selected by specified algorithms was calculated and reduced from the original signal in each selected channel. The common component of selected channels was defined as the selected common component compared with the global value for all channels.
In a second step, the three datasets (the signal without the common component, with the global common component, and with the selected common component) were processed, and their performance in pattern recognition was compared. To maximally utilize the continuous signal in the segment, an overlapping analysis window with a time length of 256 ms and an increment of 64 ms was applied to obtain more training samples. Two commonly used time and frequency domain feature series were then computed independently and provided to a pattern recognition classifier in each analysis widow. The time domain feature series, which has been shown to be simple and effective in many studies, contained four time-domain statistics of EMG signals, including the mean absolute value (MAV), the number of zero crossing (ZC), slope sign change (SSC), and waveform length (WL).13,14 In addition, the frequency domain feature series consisted of sixth-order autoregressive (AR) model coefficients combined with root mean square (RMS). Then m-dimensional feature series (
The uniform uncorrelated linear discriminant analysis was then adopted for feature dimension reduction. A linear discriminant analysis (LDA) algorithm was used to build the classifier in this study, because its low computational cost and effectiveness in myoelectric classification have been demonstrated in many previous studies.
Channel selection method
In the study, the sequential feed-forward selection (SFS) algorithm as well as the arithmetic sequence (AS) method were applied on the three datasets to form selected channel sets. The SFS algorithm, which has been proven to be effective in our previous studies, is a global algorithm that chooses the most informative channels based on empirical classification results.9,11,15 In the first iteration of the SFS method, the optimal channel that had the highest classification accuracy was selected among all of the channels. Then, for the next iteration, another channel that could achieve the maximum classification performance combined with the selected channels was added. This procedure was repeated until the number of “optimal” electrodes cumulated to a desired number, and a resulting list of channels was obtained. However, the optimal channel set would be variable for different datasets. To compare the classification performance in uniform selected channels, the AS was used to select optimal channels as well.
Alternatively, the AS is a direct channel selection method that is based on the arithmetical average of the channel index. All of the selected electrodes were added based on their index relative to other selected channels. Each increase in the number of selected channels being analyzed required a new set of evenly distributed channels that were equidistant from each other. In the study, the 29th channel, which was the point of bisection in 57 channels, was first employed as the selected channel. Then, the points of trisection (19th and 39th channels) instead of the 29th channel were selected to update the channel list for the next iteration. Similar to the SFS method, the procedure was repeated until the desired number was achieved.
Performance evaluation
The influence of the common component was assessed by the resultant classification accuracy in selected optimal channels. A two-fold cross-validation scheme was used in the study to evaluate the classification performance. The datasets within half segments were assigned as the training dataset, and the remaining half segments were used as the testing dataset. Then, the classification accuracy of a movement was calculated by the mean value of the percentage of correctly classified windows in all of the analysis windows of the testing dataset in cross-validation. The classification accuracies of seven movements were further averaged to form the global classification accuracy of all movements. Finally, the global classification accuracy of the datasets without the common component was compared with the datasets with the global common component as well as the selected common component. In addition, the common component influence on the optimal electrode location was assessed by comparing the location of the SFS optimal channels for different datasets.
Statistical analysis
The statistical analysis was performed using SPSS (SPSS Inc., 2007, Chicago, IL, USA). The Shapiro–Wilk test was used to test for possible deviations from the assumption of normality, and Student’s paired t-test was used to investigate side-to-side differences for the examined parameters if data were normally distributed, while the Wilcoxon signed-rank test was used for non-normally distributed data.
Results
Influence of the common component based on the SFS method
The influence of the common component was assessed by the resultant classification accuracies, as shown in Figure 3, where the classification accuracies achieved from the three datasets with TD+AR+RMS feature sets were compared. We observed that the datasets with the global common component achieved the best performance among the three datasets (67.40 ± 4.32% to 94.42 ± 2.96%, mean ± standard deviation). By sequentially adding the selected channels, the classification accuracy of the datasets with the selected common component dramatically increased, gradually exceeded the datasets without the common component, and then approached a maximum value (14.29 ± 1.9 × 10−15% to 92.34 ± 3.48%), which was slightly lower than the datasets with the global common component. The classification accuracy of the datasets with the global common component was significantly higher than others with an electrode number from 2 to 15 (with the global common component vs. without the common component: P = 0.05, 0.001, 0.001, 0.01, 0.01, 0.01, 0.02, 0.02, 0.01, 0.02, 0.02, 0.03, 0.02, 0.02; with the global common component vs. with the selected common component: P = 0.001, 0.001, 0.001, 0.001, 0.001, 0.001, 0.001, 0.001, 0.001, 0.002, 0.002, 0.005, 0.01, 0.01). The classification accuracy of the datasets with the selected common component was significantly lower than without the common component (P = 0.012, <0.05) when the electrode number was five, but the difference was not statistically significant (P = 0.40, >0.05) when the electrode number was 12.
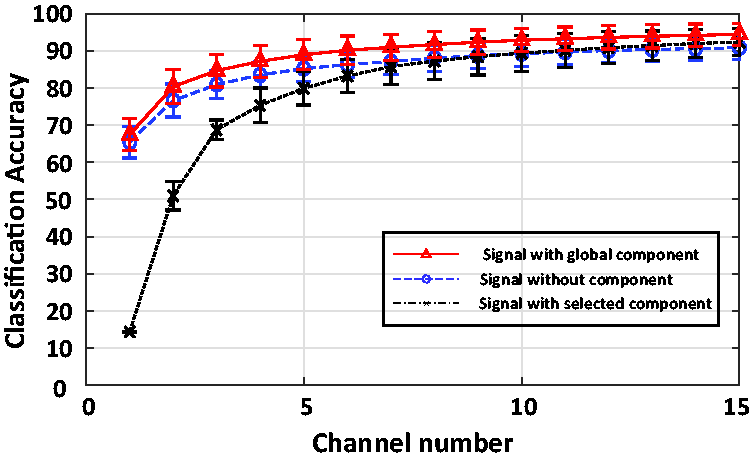
Classification accuracy of seven movements based on the sequential feed-forward selection (SFS) electrode list. The electrode numbers were increased based on the SFS electrode list. Triangle with a solid line: signal with global common component from all 57 channels. Circle with a dashed line: signal without common component. Cross with a dash-dotted line: signal with selected common component following the channel list.
Influence of the common component on the optimal distribution of channels
For each participant, we further investigated the optimal channel distribution based on the SFS method for three datasets. An example of the optimal channel distribution using the SFS method for three datasets is compared in Figure 4.
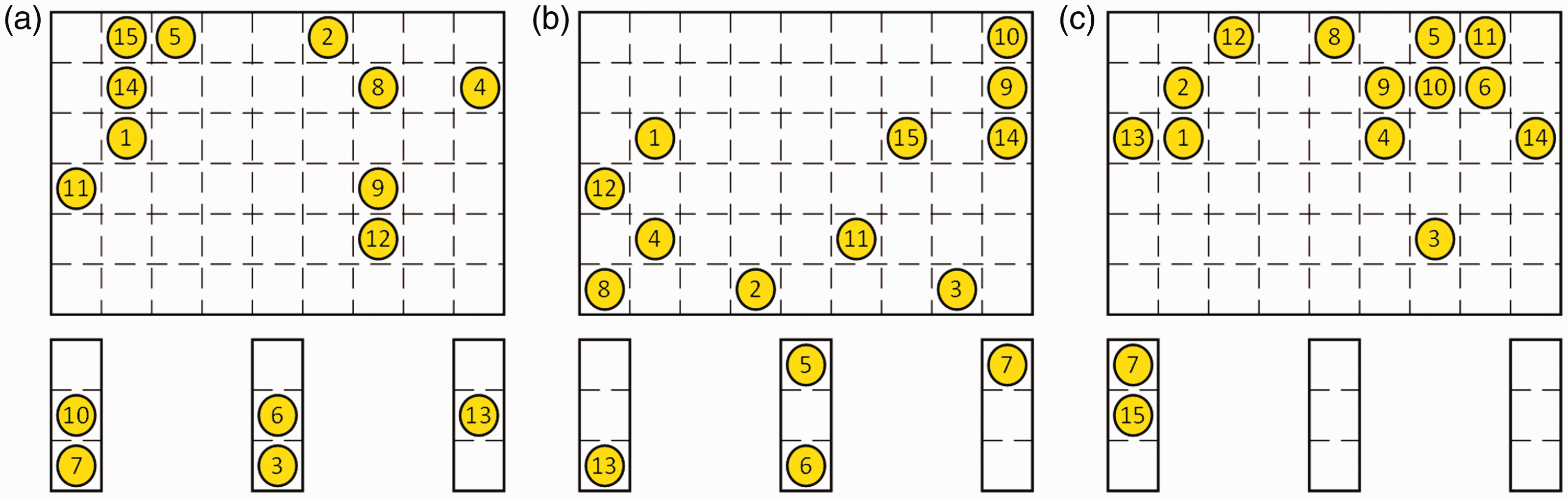
Optimal channel distribution for a participant. a: Channel distribution of original dataset without common component. b: Channel distribution of dataset with the selected common component. c: Channel distribution of dataset with the global common component.
From Figure 4, it is seen that the distribution of optimal channels varied with the three datasets. It was noted that the location of the first selected channel (channel 1), which had the highest classification accuracy in all channels, was always similar for all datasets. However, for the same participants, the location of selected channels (channels 2–15) might be partly or completely different for the three datasets. This finding showed that as an alternative, the common component would affect the optimal channel distribution.
Influence of the common component based on AS method
To investigate the influence of the common component on the uniform channel distribution, the classification accuracies of the three datasets based on the AS method were computed (Figure 5).

Classification accuracy of the seven movements based on the arithmetic sequence (AS) method. The number of electrodes was increased based on the electrode list, which was determined by the AS method. Triangle with a solid line: signal with global common component from all 57 channels. Circle with a dash line: signal without common component. Cross with a dash line: signal with selected common component following the channel list.
It was observed that the datasets with the global common component maintained the best performance among the three datasets. With an increase in channel number, the datasets with the selected common component tended to approach similar or slightly higher classification performance compared with the datasets without the common component. The classification accuracy of the signal with the selected common component (85.85 ± 4.72%) was slightly higher than the signal without the common component (84.74 ± 4.47%). Similarly, the classification accuracy of the datasets with the selected common component was significantly lower than without the common component (P = 0.035, <0.05) when the electrode number was seven, but the difference was not statistically significant (P = 0.12, >0.05) when the electrode number was 12.
Discussion
This study investigated the influence of the common component on the classification performance in limited channels for healthy participants. The main findings of the present study include the following: (1) satisfied classification accuracy in seven movements’ pattern recognition could be maintained with 12 selected channels in our study; (2) the classification accuracy of the signal with the common component was lower compared with the signal without the common component when the electrode number was limited (<5); (3) the common component improved the classification performance when the number of surface EMG electrodes was sufficient (i.e., >12); (4) the distribution of the optimal channels was related to the common component when using the TMSi system.
Generally, more electrophysiological information is captured using more surface EMG channels, which improves the classification performance of pattern recognition used to control a myoelectric rehabilitation robot. However, this is not only complex for clinical implementation but also increases the cost of data processing for the EMG-controlled systems with a large electrode number. Previous studies suggested that the number of EMG channels could be reduced while maintaining high classification accuracy.9,11,16 For example, Zhou et al. reported that it was possible to achieve satisfactory classification performance with four to nine bipolar electrodes. Another study indicated that 90% of the maximum accuracy could be maintained with eight selected channels. 14 Huang et al. reported that 12 selected channels were sufficient to extract neural control information such as HD surface EMG recording. However, the number of EMG channels that can maintain high classification accuracy in pattern recognition could not been confirmed. It is necessary to determine an appropriate number of electrodes and their locations for pattern recognition in the clinical setting while maintaining high classification accuracy. Two methods, including SFS and AS, were adopted to select channels in our study. The SFS method was used to select the appropriate EMG channels with the highest classification performance and has been considered an effective method in previous studies. In this study, we found that 12 EMG channels might be sufficient to achieve a proper motion classification performance. This finding is consistent with the conclusions obtained by Zhou and Huang. 9 Compared with SFS, the AS method provided the uniform selected channels for three datasets. The results of the AS method also confirmed that 12 electrodes were suitable for selecting EMG channels.
While the TMSi system has been widely used in previous studies,17–20 no studies have analyzed the influence of the common component that is caused by the TMSi system on the classification of movements. Thus, three datasets, including the original dataset, the dataset with the global common component, and the dataset with the selected common component were constructed to assess the influence of the common component. By examining the classification performance of these three datasets, we found that the signals with the global common component had the highest classification performance of all datasets. This may suggest that the common component improves classification accuracy when the channel number is sufficient. Furthermore, the classification accuracy of the datasets with the selected common component was lower when the channel number was less than five and higher when the channel number was above 12 compared with the original signals in both the SFS and AS results. When the channel number was small, the common component reduction would reduce the amplitude or even the quality of the recording data. However, much redundant information, which was unnecessary for pattern recognition, was contained in the HD surface EMG recordings. When the channel number was sufficient, the common component reduction would help to clean and reduce this redundant information. Meanwhile, the ground and other common noise sources were reduced as well. This finding showed that the channel number should be maintained at 12 for satisfactory classification performance in the clinical setting when using systems with the common component. In addition, these results indicated that the common component reduced the classification performance when the channel number was limited and improved the classification performance when the channel number was sufficient.
We also analyzed the distribution of the optimal EMG channels using SFS for three datasets. The results of the current study are consistent with the previous findings that the optimal EMG channels were different for each participant. In addition, the distributions of the optimal EMG channels were different for the three datasets. This finding showed that the optimal distribution of EMG channels was influenced by the common component as well.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the CAMS Innovation Fund for Medical Sciences (CIFMS, 2019-I2M-1-004), Basic Research Program for Beijing-Tianjin-Hebei Coordination (19JCZDJC65500(Z)), the National Nature Science Foundation of China (61501524), and the Fundamental Research Funds for the Central Universities and PUMC Youth Fund (No.3332017169).