
Abstract
Objective
The objective was to investigate the frequency and type of chromosomal abnormalities and Y chromosome microdeletions in infertile men with azoospermia and oligozoospermia to ensure appropriate genetic counseling before assisted reproduction in Eastern China.
Methods
A total of 201 infertile men (148 with azoospermia and 53 with oligozoospermia) were enrolled. Real-time PCR using six Y-specific sequence-tagged sites of the azoospermia factor (AZF) region was performed to screen for microdeletions. Karyotype analyses were performed on peripheral blood lymphocytes with standard G-banding.
Results
Out of 201 infertile patients, 22 (10.95%) had Y microdeletions [17/148 (11.49%) men with azoospermia and 5/53 (9.43%) men with oligozoospermia]. The most frequent microdeletions were in the AZFc region, followed by the AZFa+b + c, AZFb+c, AZFa, and AZFb regions. Chromosomal abnormalities were detected in 18.91% (38/201) of patients, 34 of which were sex chromosome abnormalities (16.92%) and 4 of which were autosomal abnormalities (1.99%). Chromosomal abnormalities were more prevalent in men with azoospermia (22.97%) than in those with oligozoospermia (7.55%).
Conclusions
We detected a high incidence of chromosomal abnormalities and Y chromosomal microdeletions in infertile Chinese men with azoospermia and oligozoospermia. These findings suggest the need for genetic testing before the use of assisted reproduction techniques.
Keywords
Introduction
Infertility is a public health problem that affects approximately 10% to 15% of couples around the world; half of infertility cases are caused by male factors.1,2 Genetic defects occur in more than 30% of cases of male infertility. 3 Y chromosome microdeletion is the second most common cause of male infertility following Klinefelter syndrome. 4 Chromosome abnormalities are considered one of the most important causes of male infertility, estimated to occur in 2.1% to 28.4% of infertile men and in only 0.7% to 1% of the general male population. 5
Azoospermia factor (AZF) microdeletion on the Y chromosome is a major genetic cause of male infertility.6,7 The AZF locus is subdivided into three regions: AZFa, AZFb, and AZFc, and microdeletions often occur in AZFc and AZFb.8,9 Microdeletion of AZFa is relevant to complete Sertoli cell-only syndrome and azoospermia. Therefore, the technique of intracytoplasmic sperm injection (ICSI) is not recommended in patients with complete AZFa microdeletion. 10 Additionally, no mature spermatozoa are found in patients with entire AZFb microdeletion, so ICSI is only recommended for patients with partial AZFb microdeletion. 11 Moreover, because patients with AZFc microdeletion may have sperm in the ejaculate, ICSI is highly recommended for patients with AZFc microdeletion. 11
At present, genetic analysis of male infertility is rarely reported in Eastern China. Therefore, the main purpose of this study was to investigate the frequency and type of chromosomal abnormalities and Y chromosome microdeletions in infertile men with azoospermia and oligozoospermia, assess the correlation of Y chromosome microdeletion and chromosome abnormalities with male infertility, and provide a theoretical basis for the clinical diagnosis and treatment of male infertility.
Material and methods
Patients
A total of 201 infertile men with azoospermia (n = 148) and oligozoospermia (n = 53, sperm concentration <15 × 106/mL) were recruited from the Xuzhou Central Hospital (Xuzhou, China) from October 2015 to August 2018 (retrospective analysis). All of the patients underwent physical examination, semen analysis, reproductive hormone estimation, karyotyping, and Y chromosome microdeletion analysis. The semen analysis was done according to World Health Organization (WHO) guidelines. 12 Men with obstructive azoospermia were excluded. Semen samples were obtained by masturbation after 3 to 7 days of sexual abstinence. Each patient had to have at least two abnormal semen analyses to be included. Each participant provided written informed consent prior to enrollment and the study received ethical approval.
Cytogenetic analysis
In the 201 infertile patients, karyotype analysis was performed on peripheral blood lymphocytes by chromosome G-banding. In brief, peripheral blood was collected in heparinized Vacutainers (Hu Nan, China). Cultures were incubated in RPMI-1640 medium for 72 hours at 37°C and treated with 40 µg/mL colchicine for 30 minutes. G-banding of metaphase chromosomes was performed by hypotension (0.075 M KCl), fixation, trypsinization, and Giemsa staining. At least 20 metaphase spreads per subject were analyzed. The chromosomal abnormalities were described according to the International System for Human Cytogenomic Nomenclature. 13
Detection of AZF microdeletions
Real-time PCR was used to detect AZF microdeletions. Genomic DNA (gDNA) was isolated from peripheral blood lymphocytes by using the QIAamp Blood Mini Kit (Qiagen, Hilden, Germany). Two sequence-tagged sites (STSs) were chosen for each AZF subregion (AZFa, b, and c loci) and organized into two PCRs, including a PCR internal control Y14 (SRY). The gDNA was amplified by two four-plex (FAM/HEX/ROX/Cy5) real-time PCRs using the STSs, including SRY, sY84, sY127, and sY255 in group A, and ZFX/ZFY, sY86, sY134, and sY254 in group B. SRY was used as an internal quantity control and the ZFX/Y gene, located on both X and Y chromosomes, as an internal control for PCR. 14 The primer sequences are shown in Table 1.
STS and gene-specific primer sequences for Y chromosome microdeletion analysis.

STS, sequence-tagged site.
Each 25-µL reaction included 22.5 µL of PCR Mix, primers, probes, Taq DNA polymerase, and 50 ng of gDNA. A blank sample used ultrapure water instead of gDNA as an external control. Reactions were run on an ABI 7500 real-time PCR system (Life Technologies, Carlsbad, CA, USA) with the following program: 2 minutes at 50°C, 5 minutes at 95°C, and 38 cycles of 15 s at 95°C, 35 s at 60°C, and 30 s at 72°C. The results were considered positive when the cycle threshold (Ct) was <32, as shown in Table 2.
Ct values obtained for each STS tested.

Ct, cycle threshold; STS, sequence-tagged site.
Statistical analysis
Statistical analysis was performed by using SPSS software (version 16.0; SPSS Inc., Chicago, IL, USA) using Student’s t-test as appropriate. A value of P < 0.05 was used to indicate statistical significance.
Results
A total of 201 infertile men were studied, 148 (148/201; 73.63%) of whom were azoospermic (where no sperm was found in the ejaculate even after centrifugation) and 53 (53/201; 26.37%) were oligozoospermic. The age (mean ± SD) of infertile males was 29.46 years (range 19 to 43 years). Toxic exposure or medication-related factors were not apparent in these infertile men by review of case histories.
Of 201 cases of male infertility, 38 (34 azoospermic and 4 oligozoospermic men) had abnormal karyotypes (numerical or structural chromosomal abnormalities), corresponding to a frequency of 18.91%. The proportion of chromosomal abnormalities in azoospermic men (22.97%) was significantly higher than that in men with severe oligozoospermia (7.55%) (P < 0.05). Klinefelter syndrome (47,XXY) was detected in 25 patients (12.44%), deletions in 2 patients (1%), mosaic chromosomes in 3 patients (1.49%), 46,XX male in 3 patients (1.49%), chromosome translocations in 4 patients (1.99%), and a ring chromosome 12 in 1 patient (0.5%) (Figure 1). The 47,XXY karyotype was more common in men with azoospermia (15.54%) than in those with severe oligozoospermia (3.77%) (P < 0.05). The remaining 163 patients (81.09%) had a normal male karyotype (46,XY). Six patients had both chromosomal abnormalities and Y chromosome microdeletions. The results are shown in Table 3.
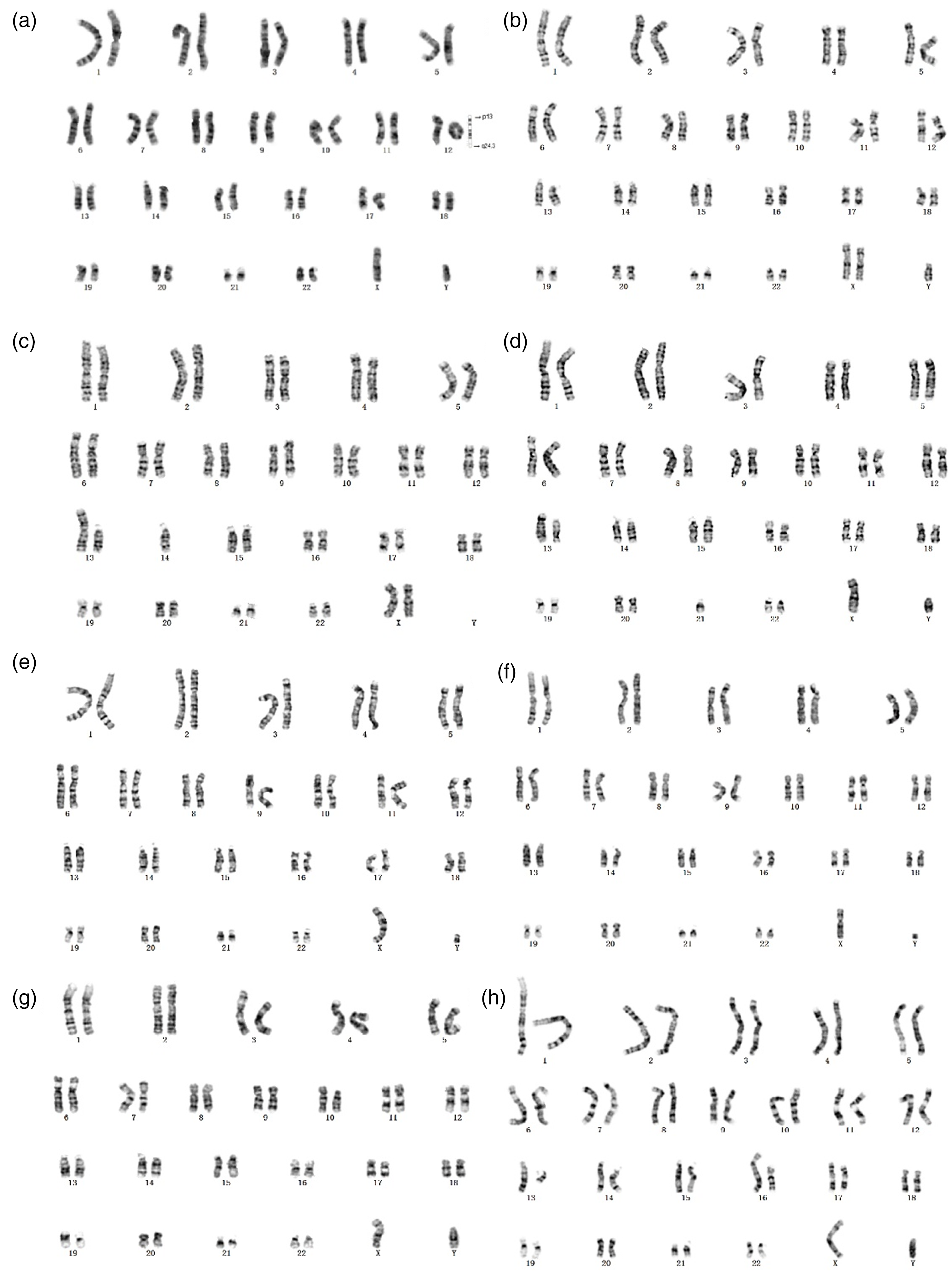
Karyograms of patients with chromosomal abnormalities: (a) r(12)(p13q24.3); (b) 47,XXY; (c) rob(13;14); (d) rob(13;21); (e) del(Y)(q11); (f) del(Y)(q11.23); (g) t(Y;10)(q12;p11.2); (h) t(13;16)(q12;q13).
Distribution of abnormal karyotypes in infertile patients with non-obstructive azoospermia or oligozoospermia (n = 201).

Of 201 infertile patients, 22 (10.95%) had AZF region microdeletions on the Y chromosome; 17 of these (11.49%) had azoospermia and 5 (9.43%) had oligozoospermia. The most frequent microdeletions were in the AZFc region, followed by AZFa+b + c, AZFb+c, AZFa, and AZFb regions (Table 4). Of these, one patient had a partial AZFa microdeletion (absence of the sY86 marker). By using real-time PCR with two AZFa STS markers, we found that marker sY86 was absent but sY84 was present in this case. The amplification plots for these mutations are shown in Figure 2.
Frequency of different AZF microdeletions on the Y chromosome in infertile male patients (n = 201) with azoospermia or oligozoospermia.

AZF, azoospermia factor.

Amplification curves for a partial AZFa microdeletion. (a) SRY, sY84, sY127, and sY255; and (b) ZFX/ZFY, sY86, sY134, and sY254 amplification curves. One AZFa marker (sY86) was absent in group B, and another marker (sY84) was detected in group A. AZF, azoospermia factor.
Discussion
Spermatogenesis is regulated by a number of genes on the Y chromosome and on autosomes.15,16 In this study, the proportion of chromosomal abnormalities in infertile men (azoospermic and oligozoospermic) was 18.91%, which is similar to that reported in earlier studies.17,18 The proportion of chromosomal abnormalities in azoospermic men (22.97%) was significantly higher than that in men with severe oligozoospermia (7.55%). The results were comparable to those of previous studies. 18
Among sex chromosome abnormalities, Klinefelter syndrome is the most frequent cause of infertility. 19 In this study, we found 25 men with the 47,XXY karyotype (12.44%), which was more common in men with azoospermia (15.54%) than in those with severe oligozoospermia (3.77%). The overall frequency was higher than that reported in a previous study. 20 Most men with Klinefelter syndrome are azoospermic. 21 Patients with Klinefelter syndrome can have offspring by using the testicular sperm extraction (TESE) technique and ICSI.22,23
After Klinefelter syndrome, Yq deletions are the next most frequent cause of male infertility. In our study, two patients with Yq deletions were found and both were azoospermic. In fact, the long arm of the Y chromosome has a critical role in the process of spermatogenesis. Three patients had karyotype 46,XX, called “XX male syndrome.” Men with this syndrome can have normal male external genitalia, similar to patients with Klinefelter syndrome. 24 The proportion of XX male syndrome in our patients was 1.49%. Three patients had mosaic karyotypes: 45,X[22]/46,XY[78], 47,XXY[78]/46,XY[22], and 47,XXY[77]/46,XY[23]; all of these patients were azoospermic.
Ring chromosome 12 is a rare structural chromosome abnormality. 25 One patient in our study had the karyotype 46,XY,r(12)(p13q24.3). Ring chromosomes can result from breakage of an end segment of both arms of a chromosome and subsequent end joining. 26 Patients with a ring chromosome may have physical and mental defects, as well as spermatogenic arrest. However, the underlying mechanisms of spermatogenetic failure in infertile patients with ring chromosomes are unclear.
Sex chromosome abnormalities were more frequent than autosomal abnormalities in the current study: 16.92% versus 1.99%. In our study, autosomal chromosomal abnormalities included the ring chromosome and translocations (reciprocal, Robertsonian). One case was a reciprocal translocation between different chromosomes and two cases were Robertsonian translocations; all translocations were balanced.
Y chromosome microdeletions are the second most frequent genetic factor underlying infertility. 19 In our study, we used real-time PCR instead of a conventional gel-based PCR assay, because it is a rapid, automatic, cost-effective, and repeatable method. Real-time PCR has been used successfully to estimate the prevalence of Y chromosome microdeletions. 24 The overall frequency of AZF deletions in our population of Eastern Chinese men with infertility was 10.95% (22/201 patients), and the frequency in azoospermic and oligozoospermic men was 11.49% (17/148 patients) and 9.43% (5/53 patients), respectively. This frequency is similar to those reported by Wang et al. 27 (9.2%), Yousefi-Razin et al. 28 (12%), and Kim et al. 29 (10.93%). Our data showed that AZFc deletions were the most frequent microdeletions (as reported previously 30 ), followed by deletions in the AZFa+b + c, AZFb+c, AZFa, and AZFb regions. One patient had a partial AZFa microdeletion (indicated by absence of the sY86 marker). Studies have shown that men with AZFc deletion can produce sperm but some do not have any sperm inside their seminiferous tubules. 31 In a previous study, patients with AZFc deletion had a good prognosis for successful retrieval of sperm by TESE, whereas patients with deletions in the AZFa and AZFb regions did not have a good prognosis. 32 In our study, only the AZFc deletion was found in an oligozoospermic patient, which was in agreement with results from previous studies.
In conclusion, we detected a high incidence of Y chromosome microdeletions and chromosomal abnormalities in Chinese patients with azoospermia and oligozoospermia. It is important for patients with azoospermia or oligospermia to undergo these examinations to determine the underlying cause of infertility. Based on the results of chromosomal and Y microdeletion analyses, we can determine whether patients need assisted reproductive therapy, and patients can avoid the physical and mental trauma caused by unnecessary surgery. It is also important for infertile male patients to obtain reliable screening for genetic defects before ICSI and in vitro fertilization is performed to prevent AZF microdeletions and chromosomal abnormalities from being passed on to their offspring.