
Abstract
Objective
To investigate the therapeutic effects of a combination of plasma exchange (PE) and haemofiltration (HF) for the treatment for paediatric patients with severe thrombotic microangiopathy (TMA).
Methods
This retrospective study analysed data from paediatric patients who were diagnosed with severe TMA and managed with either supportive therapy and additional PE and HF (PE + HF group) or supportive therapy alone (control group). Demographic and clinical characteristics, haemopurification and blood parameters and survival of the patients were compared between the two groups.
Results
This study enrolled 32 patients: PE + HF group (n = 15) and control group (n = 17). There were no significant differences between the two groups at baseline, including specific features for differentiating the two categories of TMA. The median time between onset and recovery, defined by the markers of platelet count, lactate dehydrogenase, blood urine nitrogen and hospital stay, were all significantly longer in the control group compared with the PE + HF group. Kaplan–Meier curve analysis demonstrated that the cumulative survival rate was significantly higher in the PE + HF group compared with the control group.
Conclusion
The combination of PE and HF could be considered as one of the treatment choices for TMA.
Introduction
Thrombotic microangiopathy (TMA), formerly known as haemolytic uraemic syndrome (HUS), is a life-threatening disease with a triad of microangiopathic haemolytic anaemia, destructive thrombocytopenia and renal failure. 1 The overall incidence of TMA is estimated to be 2.1 per 100 000 people; and it mainly affects children of pre-school age who have an incidence of 6.1 per 100 000.2,3 The mortality rate is considered to be 2–5%, 4 which usually occurs in the acute phase. Even though 70% of patients recover without permanent sequelae, TMA is the main cause of acute kidney injury in children,5,6 making the timely treatment for children with suspected TMA essential.
There are two categories of TMA: (i) Shiga toxin-mediated TMA, formerly known as typical HUS; and (ii) complement-mediated TMA, formerly named as atypical HUS. 1 Treatment suggestions are different for these two categories. Shiga toxin-mediated TMA is managed supportively, but the use of antibiotics remains controversial. 7 Plasma exchange (PE) is suggested for the treatment of complement-mediated TMA, but is not considered to be of benefit for Shiga toxin-mediated TMA. 8 However in clinical settings, PE is still used to treat Shiga toxin-mediated TMA,9,10 and some case reports have described therapeutic success.11,12
Plasma exchange is a therapeutic haemopurification procedure in which the blood of the patient is passed through medical apparatus that removes high molecular weight substances and replaces them with a solution such as albumin or fresh frozen plasma, which provides missing essential factors, for example, complement factor H and I in patients with complement-mediated TMA are contained.1,13 The targeted substances that are planned to be removed include immune complexes, endotoxins, autoantibodies and lipoproteins, all of which are potentially related to immune-mediated disorders.1,14
Haemofiltration (HF) is another haemopurification technique that removes excess body fluid across a haemofilter membrane using positive pressure and accumulates substances in patients with severe loss of kidney function that are critically ill. 15 However, HF is rarely reported for the management of both categories of TMA. 7 HF not only helps the removal of toxic substances from the bloodstream, but also improves the balance of electrolytes and acid-base. 16 The therapeutic effects of this normalization of the Na2 + , Cl– and K+ concentrations by HF have been reported in a canine model of heat stroke; and this is also important in the clinical setting because of the possible reduction of the risk of associated cardiac and neurological complications. 17 In addition, some serum enzymes, for example creatine kinase (CK) and lactate dehydrogenase (LDH), are markedly deceased after HF, indicating the prevention of sequential cellular/organ damage from occurring. 17
Considering the rationales for both PE and HF, this study investigated the combined use of these two haemopurification methods in critically ill paediatric patients with severe TMA.
Patients and methods
Patients
This retrospective study analysed data from consecutive paediatric patients who were diagnosed with severe TMA and admitted to the paediatric intensive care unit at the 900th Hospital of the Joint Logistics Team of the Chinese PLA, Fuzhou, China between June 2007 and May 2017. Patients were diagnosed with severe TMA according to the following criteria: (i) anaemia (haemoglobin <60 g/l); (ii) low platelet counts (< 100 000/μl); (iii) increased blood urea nitrogen (BUN > 10 mmol/l); (iv) creatinine (> 150 μmol/l); (v) haematuria and proteinuria. All of the above should be present when establishing a diagnosis of severe TMA. All patients confirmed no prior history or other concomitant hepatic or renal disorders. Patients were divided into two treatment groups: those who were treated with both supportive therapy and additional PE and HF procedures (PE + HF group), and those that received supportive therapy alone (control group) according to the decisions made by the parents or legal guardians of the children after the detailed treatment plans were explained by the physicians.
The Institutional Review Board of the 900th Hospital of the Joint Logistics Team of the Chinese PLA reviewed and approved this study (no. 200703) and decided that informed consent could be waived due to the observational nature of this study.
Treatment
Supportive therapy included maintaining the balance of fluids and electrolytes, haemodynamic stability and controlling blood pressure. Elective options when necessary included transfusion of red blood cells (RBCs) when haemoglobin <60 g/l and prescription of dipyridamole or diuretics. In the control group, haemodialysis or peritoneal dialysis were performed when patients were anuric for more than 1 day, or there was a rapid increase in BUN, or hyperkalaemia developed, and/or there was oedema, heart failure or resistant hypertension.
For those patients that received haemopurification therapy, PE and HF were started within 24 h of hospital admission and as early as possible. A BM-25 continuous bedside blood purification machine composed of a blood testing module (BM-11) and an ultrafiltration module (BM-14) (Baxter International, Deerfield, IL, USA) with matching cardiopulmonary bypass tubing, a P2S plasma separator (membrane areas = 0.6 m2) and polysulfone hollow fibre haemofilters AV400 (membrane areas =0.7 m2) for patients with body weights ≥30 kg; or a P1 dry plasma separator (membrane area = 0.3 m2) and polysulfone hollow fibre haemofilters AV600 (membrane areas = 1.4 m2) for patients with body weights <30 kg (all from Fresenius, Bad Homburg, Germany). An 8 Fr double-lumen central venous catheter (Arrow® International, Reading, PA, USA) and 11.5 Fr double lumen haemodialysis catheters (Fresenius) were used. Electrocardiogram and arterial pressures were monitored during PE and HF using a Philips IntelliVue MP40 (Philips Healthcare, Andover, MA, USA).
The procedures were modified based on previous studies.14,17 PE was conducted first followed by HF in an intermittent haemofiltration manner. Every complete procedure was undertaken over an interval of 1–3 days depending on the results of individual patient’s blood and biochemical tests. The catheter was placed via the femoral vein or subclavian vein for paediatric patients due to the higher risk of them falling out and the subsequent bleeding if placed via the internal jugular vein. The tubing was initially flushed with 25 U/ml heparin sodium saline for 30 min. A pre-prepared 100–150 ml suspension of RBCs was then infused. Heparin was administered intra-arterially 1 min before haemofiltration with 0.20–0.40 mg/kg, the speed was maintained at 0.10–0.20 mg/kg per h, adjusted according to the transmembrane and venous pressure as well as the coagulation function. PE was conducted using fresh frozen plasma as the replacement fluid by the post-replacement method. The blood flow rate was 45–140 ml/min, the plasma exchange rate was 400–1600 ml/h, and the plasma separation rate, which was calculated as plasma exchange rate/(blood flow rate × 60) × 100, was 12.80–25.00%. The volume of exchange was based on the guidelines and set as 1 to 2 plasma volume exchanges per patient; 1 and calculated according to the following formula: plasma volume = (1 – hematocrit) × (b + c × W), where W = body weight (kg), b = constant (1530 for males and 864 for females), and c = constant (41 for males and 47.2 for females). The volume of exchange was 880–2687 ml in this study. A 10% calcium gluconate (1 ml/100 ml plasma exchanged) solution was administered to prevent hypocalcaemia. HF was conducted using the pre-replacement method: the exchange rate was 900–4000 ml/h; and the volume of exchange was 11.00–56.80 l for 9–22 h. The net fluid removed (the volume of substitution fluids was not included) was 0–1200 ml. During HF, a suspension of RBCs was infused when necessary. Heparin was ceased 15 min before the end of HF.
Outcome measurements
The demographic characteristics were recorded for all patients. Arterial and venous blood samples were collected at days 1, 3, 5 and 10 after admission. Heparin-anticoagulated arterial blood samples were used for the assessment of blood gas parameters immediately using an ABL800 FLEX blood gas analyser (Radiometer, Thalwil, Switzerland). Ethylenediamine tetra-acetic acid anticoagulated venous blood samples were used to assess the complete blood count within 2 h using a Sysmex XE-2100 haematology analyser (Sysmex, Kobe, Japan). Sodium citrate-anticoagulated venous blood samples were used for coagulation testing using a CS-5100 Haemostasis System analyser (Sysmex). Serum was collected from venous blood samples within 2 h and biochemistry analyses were conducted within 4 h using a Cobas c 702 modular analyser (Roche Diagnostics, Mannheim, Germany). Before assessment, serum was stored at 4 °C. The biochemical parameters included aspartate aminotransferase (AST), alanine aminotransferase (ALT), bilirubin, BUN, cholinesterase, CK, creatinine, α-hydroxybutyrate dehydrogenase (α-HBDH), LDH and the concentrations of electrolytes including Na+, K+, Cl– and Ca2 + . The Paediatric Clinical Illness Score (PCIS) was assessed at days 1, 3, 5 and 10 after admission. 18 A PCIS > 90 was defined as ‘not critically ill’, 90–70 as ‘critically ill’ and <70 as ‘very critically ill’.
Statistical analyses
All statistical analyses were performed using IBM SPSS Statistics for Windows®, Version 24.0 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as the median and interquartile range (P25–P75) and categorical variables are presented as number of patients (%). The comparison between the PE + HF group and the control group was performed using Mann–Whitney U-test for continuous variables and using χ2-test or Fisher’s exact test for categorical variables. The comparisons among hospital admission (baseline), 3, 5 and 10 days after treatment were performed using Friedman test for continuous variables and Cochran’s Q test for categorical variables. The results were Bonferroni corrected to take into account the number of pairwise comparisons. Kaplan–Meier curve analysis with log-rank test was performed to compare the cumulative survival rate between the PE + HF and control groups. Propensity score was constructed by the demographic and vital sign variables, including age, sex, weight, PCIS, heart rate, respiratory rate, systolic blood pressure and diastolic blood pressure, and used to adjust the survival effect for the group comparison. A P-value <0.05 was considered statistically significant.
Results
This retrospective study enrolled 32 patients: 15 patients in the PE + HF group and 17 patients in the control group. There were no significant differences between the two groups at baseline, including specific features for differentiating the two categories of TMA (Table 1). The median time between onset and recovery, defined as platelet count > 150 × 109/l, LDH <500 U/l and BUN <8.2 mmol/l, and duration of hospital stay were all significantly longer in the control group compared with the PE + HF group (P ≤ 0.033 for all comparisons).
Baseline demographic, clinical characteristics and outcomes between two groups of paediatric patients with severe thrombotic microangiopathy (TMA) treated with either supportive therapy alone (control) or with a combination of plasma exchange (PE) and haemofiltration (HF).

Data presented as median (interquartile range) or n of patients (%).
aThe PE + HF and control group comparisons were performed using Mann–Whitney U-test for continuous variables and χ2-test or Fisher’s exact test for categorical variables.
bOnly eight patients had available data; cOnly 10 patients had available data.
PCIS, Paediatric Clinical Illness Score; RBC, red blood cell; PLT, platelet; WBC, white blood cell; C3, complement component 3; LDH, lactate dehydrogenase; α-HBDH, α-hydroxybutyrate dehydrogenase; BUN, blood urea nitrogen; CK, creatine phosphokinase; CK-MB, creatine kinase MB isoenzyme; ALT, alanine transaminase; AST, aspartate transaminase; NS, no significant between-group difference (P ≥ 0.05).
The volume of RBC suspension significantly decreased in the fourth round of haemopurification compared with the first round of haemopurification (median, 150 ml versus 350 ml; P = 0.027) (Table 2). The volume of HF exchange significantly decreased in the third round of haemopurification compared with the first round of haemopurification (median, 21 ml versus 25 ml; P = 0.048). The blood flow rate, venous pressures, transmembrane pressures, durations of the procedures, exchange rates and plasma separation rate of PE and volume of net fluid removed for HF were all consistent among the different rounds of treatment.
Haemopurification parameters during different rounds of the plasma exchange (PE) and haemofiltration (HF) procedures in paediatric patients with severe thrombotic microangiopathy.

Data presented as median (interquartile range).
aFriedman test.
*P < 0.05 indicates a significant difference compared with the first round of treatment; NS, no significant difference (P ≥ 0.05).
†Represents a significant difference across the first, second and third rounds of treatment.
The severity of TMA was measured using PCIS, cholinesterase, LDH and α-HBDH levels (Table 3). At the end of treatment (day 10), both the control and PE + HF groups showed significant improvements in all of these markers compared with baseline (P < 0.05 for all comparisons). For PCIS, LDH and α-HBDH levels, the PE + HF group demonstrated significantly earlier reductions in severity, represented by significant differences between the PE + HF and control groups at days 3, 5 and 10 (P < 0.05 for all comparisons). Compared with baseline, PCIS, LDH and α-HBDH levels were all significantly improved in the PE + HF group from day 5 to day 10; in the control group, the significance from baseline was delayed to day 10. For cholinesterase, there were no significant differences between the PE + HF and control groups at each time-point after treatment. Cholinesterase level was significantly increased at days 5 and 10 compared with baseline in the PE + HF group (P ≤ 0.005 for both comparisons). In the control group, cholinesterase level was significantly increased at day 10 after treatment compared with baseline (P = 0.045).
Severity of thrombotic microangiopathy before and after treatment in two groups of paediatric patients treated with either supportive therapy alone (control) or with a combination of plasma exchange (PE) and haemofiltration (HF).

Data presented as median (interquartile range).
aFriedman test.
*P < 0.05 indicates a significant difference compared with baseline.
†P < 0.05 indicates a significant difference compared with day 3.
‡P < 0.05 indicates a significant difference compared with day 5.
#P < 0.05 indicates a significant difference between the PE + HF group and control group.
PCIS, Paediatric Clinical Illness Score; LDH, lactate dehydrogenase; α-HBDH, α-hydroxybutyrate dehydrogenase.
At the end of treatment (day 10), all of the parameters, except creatinine, were significantly improved in both the PE + HF and control groups compared with baseline (P < 0.05 for all comparisons) (Table 4). The creatinine level demonstrated no significant differences at all of the time-points compared with baseline in the control group. RBC counts, haemoglobin, CK-MB, total and direct bilirubin were significantly better at the earliest time-point (day 3 after treatment) in the PE + HF group compared with the control group (P ≤ 0.001 for all comparisons). The significant differences between the two treatment groups were delayed to day 5 for platelet count, BUN, CK and ALT (P < 0.05 for all comparisons). Neutrophil level, creatinine and AST only showed significant differences between the two groups at day 10 (P < 0.05 for all comparisons).
Haematological and biochemical parameters before and after treatment in two groups of paediatric patients treated with either supportive therapy alone (control) or with a combination of plasma exchange (PE) and haemofiltration (HF).
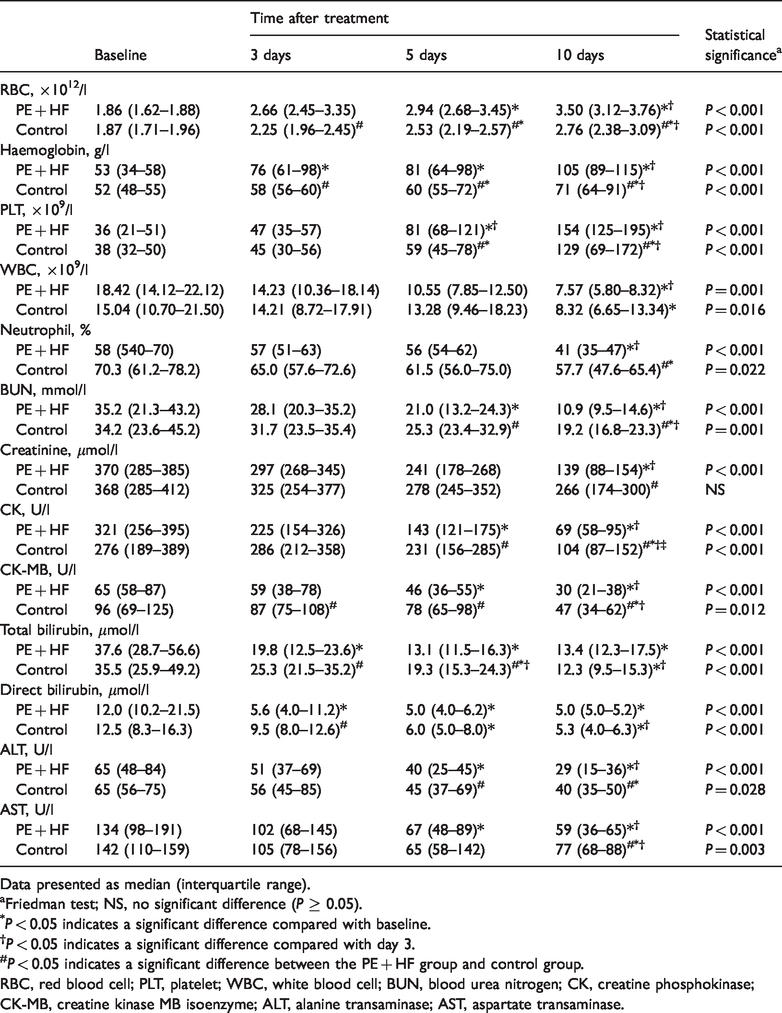
Data presented as median (interquartile range).
aFriedman test; NS, no significant difference (P ≥ 0.05).
*P < 0.05 indicates a significant difference compared with baseline.
†P < 0.05 indicates a significant difference compared with day 3.
#P < 0.05 indicates a significant difference between the PE + HF group and control group.
RBC, red blood cell; PLT, platelet; WBC, white blood cell; BUN, blood urea nitrogen; CK, creatine phosphokinase; CK-MB, creatine kinase MB isoenzyme; ALT, alanine transaminase; AST, aspartate transaminase.
Comparing the differences between the two groups at each time-point after treatment, the abnormal rates of Na+ and Cl– significantly decreased in the PE + HF group compared with the control group at 10 days (P = 0.038 for both comparisons); and the abnormal rate of Cl– significantly decreased in the PE + HF group compared with the control group 5 days after treatment (P = 0.024) (Table 5). Comparing the differences among different time-points in the PE + HF group, the abnormal rates of Na+ and Cl– significantly decreased after 5 and 10 days of treatment compared with baseline (P ≤ 0.013 for all comparisons). No significant differences in the abnormal rates of Na+ and Cl– were found between the different time-points in the control group.
The abnormal distribution of electrolytes and blood gases before and after treatment in two groups of paediatric patients treated with either supportive therapy alone (control; n = 17) or with a combination of plasma exchange (PE) and haemofiltration (HF) (n = 15).

Data presented as n of patients (%) with abnormal values.
aMissing data for one patient for days 5 and 10 in both groups: PE + HF (n = 14) and control group (n = 16).
bCochran’s Q test; NS, no significant difference (P ≥ 0.05).
*P < 0.05 indicates a significant difference compared with baseline.
†P < 0.05 indicates a significant difference compared with day 3.
#P < 0.05 indicates a significant difference between the PE + HF group and control group.
Comparing the differences between the two groups at each time-point after treatment, the abnormal rates of pH, HCO3– and base excess decreased more significantly in the PE + HF group than the control group 3 days after treatment (P ≤ 0.016 for all comparisons) (Table 5). Comparing the differences among the different time-points in the PE + HF group, the abnormal rates of pH, PaCO2, HCO3– and base excess significantly decreased after treatment at day 3 and 10 compared with baseline (P ≤ 0.020 for all comparisons); the abnormal rate of pH and HCO3– significantly decreased 5 days after treatment compared with baseline (P ≤ 0.012 for both comparisons). Comparing the differences among different time-points in the control group, the abnormal rate of pH, PaCO2 and HCO3– significantly decreased 10 days after treatment compared with baseline (P ≤ 0.031 for all comparisons); and the abnormal rate of pH and HCO3– significantly decreased 10 days after treatment compared with day 3 (P ≤ 0.026 for both comparisons).
There were 14 of 15 (93.3%) patients and nine of 17 (52.9%) patients that survived at the last follow-up in the PE + HF and the control groups, respectively. Kaplan–Meier curve analysis demonstrated that the cumulative survival rate was significantly higher in the PE + HF group compared with the control group (P = 0.015) (Figure 1A). A propensity score constructed to adjust the survival effect demonstrated that the adjusted cumulative survival rate of the PE + HF group was still higher compared with the control group, but the difference was not statistically significant (Figure 1B).

Kaplan–Meier survival curves for two groups of paediatric patients with severe thrombotic microangiopathy treated with either supportive therapy alone (control) or with a combination of plasma exchange (PE) and haemofiltration (HF). (a) original; (b) adjusted by propensity score.
Discussion
This current retrospective study intensively monitored many parameters due to the critical condition of the paediatric patients that were enrolled in the study. In addition, these current results support the rationale for the therapeutic effects of this haemopurification procedure. Compared with transfusion, using an infusion of a suspension of RBCs allowed for the faster administration of a larger volume to treat the anaemia in paediatric patients with TMA; with the blood volume and haemodynamics being controlled well by HF. Using HF alone can improve and maintain fluid balance, electrolyte status and acid-base balance, which reduces impairments to the circulatory system, liver and heart; and is probably also related to a reduction in the risk of more severe complications like multiple organ failure.12,19 Keeping a higher central venous pressure (8–10 cmH2O; normal range for paediatric patients: 5.79–11.08 cmH2O) during HF could contribute to the recovery of renal function due to the avoidance of hypoperfusion and ischaemia.
The major limitation of this current study was that it was not able to specify the two TMA categories of the paediatric patients because the essential clinical examinations for differential diagnosis were not available to the physicians. As the diagnostic categories of patients represent different pathologies, the effects of PE and HF might be different depending upon the diagnostic category and warrants further investigation. On a practical level, it is a time-consuming process to confirm the differential diagnosis of the two categories of TMA and many hospitals worldwide face the same difficulty. The clinical presentation was similar between the two study groups in this current study, including the rates of respiratory infection and gastroenteritis-like symptoms, which might be of use for specifying the TMA category. This suggests that the distribution of the two TMA categories was similar in the two study groups. Thus, this experimental strategy of supportive treatment with additional haemopurification may offer a more practical and easier approach that would enable rapid medical decision-making in emergency departments or intensive care units for critically ill patients. PE is considered ineffective for the treatment of Shiga toxin-mediated TMA.4,20 However, the remission and survival of the PE + HF group was significantly better than that of the control group in this current study. It should be noted that after adjusting for the propensity score constructed using the demographic and vital sign variables of the patients, the survival rate was still higher in the PE + HF group, but it did not reach statistical significance. This may reflect the small sample size, but the effects of the heterogeneity of the patients in each group cannot be ruled out. The retrospective design also limited data acquisition. A better study design with clearly specified TMA categories is required in the future.
The severity of TMA was monitored using PCIS, cholinesterase, LDH and α-HBDH. PCIS is a widely used scoring system in China, which was developed by the Chinese Paediatric Society and the Chinese Emergency Medicine Society. 18 The items include heart rate, blood pressure, blood gases, biochemistry and electrolytes, which aims to evaluate the physical condition of paediatric patients. The PCIS has not been translated into English, or validated in other countries, and a tool that transfers data from the PCIS to more internationally familiar scores, such as the Paediatric Index of Mortality 2, remains unavailable. This limitation might result in international researchers in this field failing to understand the severity of TMA that the PCIS represents. Due to the retrospective design of this current study, the PCIS data can only be presented with a translated supplementary table as a reference. Cholinesterase has been reported as a prognostic or severity marker for several diseases, including severe injury, 21 sepsis, 22 dementia, 23 and acute organophosphate pesticide poisoning. 24 LDH and α-HBDH levels are associated with renal damage and infection.25,26 Although these biomarkers are non-specific and increase in many other diseases, they can be easily measured using automated haematological analysers, which are routinely available in most healthcare settings. From these current results, all four parameters have the potential to be developed as markers or individual items of a combined scoring system to simply evaluate the severity of TMA when monitoring the therapeutic effects of emergency treatment.
Eculizumab is a humanized monoclonal antibody that inhibits C5 activation and blocks the production of the proinflammatory C5a anaphylatoxin, which is recommended for the treatment of complement-mediated TMA both in paediatric and adult patients. 27 However, financial constraints and non-availability of eculizumab limit its use in many clinical settings. The current findings, along with those of a previously published study that investigated 30 paediatric patients with complement-mediated TMA that were treated with PE, 28 suggest that haemopurification might be a viable and more cost-effective alternative to eculizumab.
This current study had several other limitations that should be acknowledged in addition to those described above. These include the relatively small sample size and the retrospective study design. For paediatric patients, smaller plasma separators and haemofilters should be used for decreasing the volume of the extracorporeal circulation. However due to limited resources, pre-prepared 100–150 ml suspensions of RBCs were infused instead. As discussed above, the outcomes should be analysed in groups stratified according to the category of TMA, with the aim of understanding the mechanisms involved more clearly so that appropriate modifications can be made to the procedures as required.
In conclusion, the treatment of paediatric patients with severe TMA using a combination of PE and HF significantly increased their survival compared with routine supportive treatment. These current findings suggest that PE + HF could be considered as one of the treatment choices for patients with TMA.