
Abstract
This study describes a rare case of male granulomatous lobular mastitis (GLM) with recurrence in different sites on the ipsilateral side. A 48-year-old male patient presented with no previous history of breast-related disease, and physical examination suggested a mass in the right breast. Ultrasonography revealed a cyst and infection in the right breast. No obvious abnormality was found in laboratory analysis, and a core needle biopsy revealed GLM. Incision and drainage were applied to the right lesion, and symptoms resolved within a few weeks. At 2 years following this initial presentation, the patient reported that the right breast mass reappeared in different locations after the consumption of alcohol. Relevant examination and a core needle biopsy again suggested GLM of the right breast. The patient declined hormone therapy and was subsequently lost to follow-up. After reviewing this case, the course of the disease in this patient, and the connection between gynecomastia and GLM, along with ipsilateral recurrence, are under investigation.
Keywords
Introduction
Granulomatous lobular mastitis (GLM) is a non-caseous type of necrosis confined to the lobule of the breast, with granulomas being the main pathological features of benign, chronic inflammatory disease. 1 First described and named by Kessler and Wolloch in 1972, 2 GLM exhibits an increasing annual incidence. 3 Most cases of GLM occur in pregnant women, and the age of onset is 17–52 years. The main clinical manifestations of GLM are breast mass, pain, nipple depression, nipple overflow, axillary lymph node enlargement, oedema, and sinus tract.4,5 Modern medical research has led to multiple views about the aetiology, pathogenesis and clinical therapy associated with GLM, however, the pathogenesis of GLM remains unclear. The occurrence of GLM is more rare in male patients than in female patients, with only 14 published cases, according to previous literature reviews.6,7 Here, the case of a male patient with recurrent ipsilateral GLM is described.
Case report
A 48-year-old male patient presented at the Outpatient Clinic of Chongqing Hospital of Traditional Chinese Medicine, Chongqing, China, in January 2019, with a right breast mass that was painful without obvious inducement. Physical examination of the right breast showed pain, swelling and heat. Laboratory blood analysis revealed a mild increase in leukocytes, and ultrasonography images suggested male breast tissue, displaying a mixed echo region in the lower quadrant of approximately 1.7 × 1.0 cm in size, suggesting the possibility of cyst and infection. The patient then attended a different hospital, where he received anti-infection treatment for 3 days, with no significant relief of symptoms. In February 2019, the patient returned to Chongqing Hospital of Traditional Chinese Medicine. He reported no congenital depression, nipple discharge, previous history of breast cancer or psychiatric illness. Laboratory tests of routine blood parameters, blood coagulation function, and liver and kidney function all returned normal results. Following a core needle biopsy, the right breast mass was diagnosed as GLM due to inflammatory cell infiltration and inflammatory granulation (Figure 1). Bacterial culture of pus smear showed the growth of gram-positive cocci. According to the pathology and clinical manifestations, the diagnosis of male GLM was confirmed. The patient expressed strong opposition to glucocorticoid treatment due to steroid hormone side-effects. Incision and drainage were applied to the lesion and the patient returned home for self-administered wound care (dressing changes). The patient did not receive regular treatment or follow-up at the Breast Department of Chongqing Hospital of Traditional Chinese Medicine.

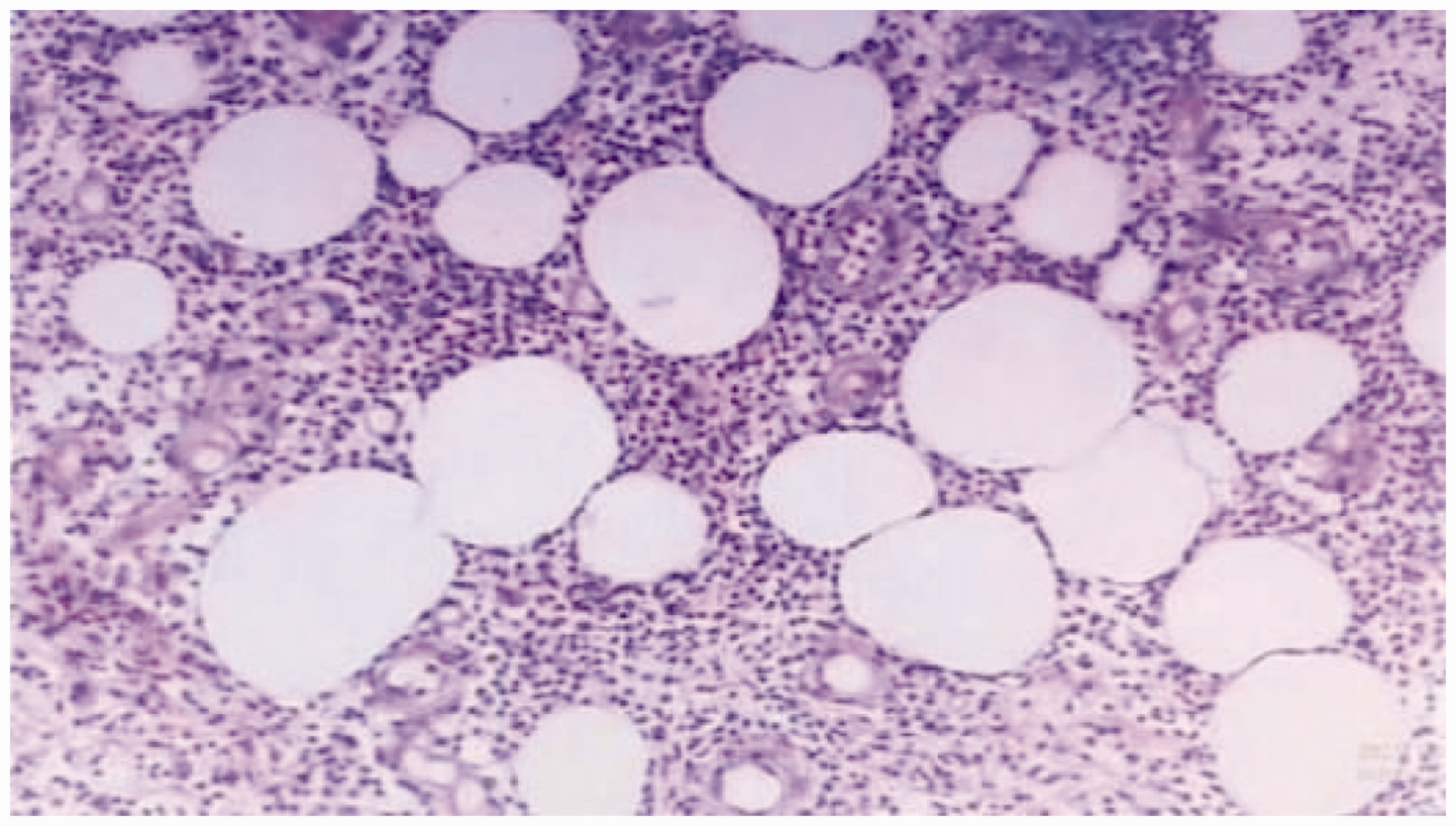
Haematoxylin–eosin-stained tissue sections from a core needle biopsy of the painful right breast of a 48-year-old male patient, showing: (a and b) infiltration of lymphocytes, neutrophils and a small amount of plasma cells in the fibroadipose tissue, and inflammatory granulation tissue (a, original magnification, × 100; and b, original magnification, × 40).
Two years later, the patient reported right breast mass with pain after heavy drinking. The pain was relieved after antibiotic treatment, but no shrinkage of the mass was observed, so the patient returned to the Breast Department of Chongqing Hospital of Traditional Chinese Medicine in April 2021. Physical examination revealed a mass of about 5 × 6 cm in the right breast, with pain and swelling (Figure 2). Ultrasonography imaging showed that the subcutaneous size of the right breast mass was approximately 2.5 × 1.1 cm, with a clear border, irregular border, and hypohomogeneous internal echo, and the possibility of abscess formation was considered (Figure 3). Laboratory examination indicated mild elevation of neutrophils, but no abnormal routine blood parameters, coagulation, or liver and kidney function. Ultrasound-guided core needle biopsy showed inflammatory cell infiltration and small plasma cells in the stroma, suggestive of GLM (Figure 4), and a pus smear bacterial culture showed gram-positive coccal growth. Based on the pathological and clinical findings, the patient was diagnosed with gynecomastia with GLM. The patient declined hormone therapy and the lesion was treated by incision and drainage, followed by self-administered care at home. The patient was subsequently lost to follow-up until March 2023, when the patient reported that the lesion had healed during a follow-up phone call.

Representative images from physical examination of the painful right breast of a 48-year-old male patient, showing: (a and b) a visibly inflamed and swollen mass of approximately 5 × 6 cm in size.

Ultrasound image of the painful right breast of a 48-year-old male patient showing a clear and irregular border, and hypohomogeneous internal echo. The possibility of abscess formation was considered.
Haematoxylin–eosin-stained tissue section from a core needle biopsy of the painful right breast of a 48-year-old male patient, showing infiltration of neutrophils, lymphocytes and small plasma cells in the stroma (original magnification, ×100).
Ethics committee approval was not deemed necessary due the case study design, and the patient provided verbal informed consent for treatment, publication of this case and associated data and images. All patient details were deidentified for the study, and the reporting of this study conforms to CARE guidelines. 8
Discussion
Granulomatous lobular mastitis is a chronic inflammatory disease characterized by non-caseous necrosis and granuloma formation. The pathogenesis and aetiology of GLM remain unclear, and GLM is generally believed to be mainly an autoimmune disease, which may be related to oral contraceptives, fungal infection, bacterial infection, hyperprolactinemia and milk hypersensitivity reaction. GLM is clinically and radiologically similar to breast cancer and has a high local recurrence rate. Generally, this disease most often occurs in the non-lactation stage, but in clinical practice, cases of GLM are increasingly being observed during lactation; however, whether GLM is a non-lactation type of granulomatous mastitis is under debate. Treatment of idiopathic granulomatous mastitis (IGM) remains controversial, with surgical treatment, immunosuppressive therapy, or a combination of the two being the most adopted current methods. 4
The occurrence of GLM in men is rare, with only 14 cases reported in the literature to date. In the present case, the 48-year-old male patient exhibited right breast mass with pain, which seems to correspond to the mean age of 45.80 ± 4.226 years (range, 21–60 years), mainly painful (70%) or painless unilateral breast mass with obvious right-sided tendency reported in the literature. 6 Male breasts are small, allowing the patient to detect a smaller mass at an early stage, which may explain the absence of advanced local signs, such as ulceration and sinus tract observed in cases of GLM in male patients, which are all concentrated in the mass stage.
Pathologically, the adult male breast contains small amounts of fat and stromal tissue, and a small number of residual ducts without lobular development. In the present study, the patient exhibited atrophy of the second puncture, and inflammatory reactions were seen in the surrounding lobules and stroma of the gynecomastia, thus, gynecomastia could be clearly diagnosed according to the pathological results. However, the clear breast lobules were not observed during the first disease examination in this patient, which may have been caused by an operative deviation during the initial puncture. This also further indicates that crude needle biopsy provides the highest accuracy in the diagnosis of GLM. 9
The aetiology of this disease is difficult to clarify due to the small number of reported cases. Most cases of IGM in females has been reported to involve parity and pregnancy, 10 suggesting that prolonged exposure to high levels of oestrogen may play a role in the pathogenesis of IGM. In the present case, male breast development was not considered at the first visit because the patient had no relevant breast history and no obvious enlargement and development of the breast, and the diagnosis of gynecomastia was not made until after the pathological prompt of the second puncture. It may have been due to operation deviation during the first biopsy, or may have been due to the effect of GLM on androgens and oestrogen, leading to the development of the male mammary gland. In addition, the patient reported a history of heavy alcohol intake at the second onset, and there is evidence to show that alcohol consumption is significantly positively associated with plasma luteal oestrogen concentrations, but not with androgen levels, or with oestrone or oestradiol measured in the follicular phase. 11 To the best of our knowledge, the association between GLM and prolactin levels is already confirmed. However, the relationship between alcohol and IGM in male patients remains unproven, and requires more case reports and further research. In addition, it currently remains unclear whether development of the male breast may be caused by GLM.
Gynecomastia is a benign hyperplasia of male glandular breast tissue. In male patients with gynecomastia, about 70% exhibit adolescent gynecomastia, and two-thirds develop palpable breast tissue.12,13 Gynecomastia is idiopathic in the majority of adolescents, and in 75% to 90% of patients, it resolves spontaneously after 1–3 years. 14 The exact pathogenesis of gynecomastia is unknown, but is thought to be due to the relative or absolute lack of androgenic action in breast tissue. 15 Chronic diseases, such as cirrhosis, hypogonadism, and renal insufficiency; use of supplements, drugs, or dangerous drugs; and in rare cases, tumours, may all cause physiological gynecomastia. 16
Gynecomastia is a common disorder in the general population and affected individuals may experience localized and radiating pain. Gynecomastia may be physiological or non-physiological due to disruption of the oestrogen-to-testosterone ratio in males; 17 when the male oestrogen-to-testosterone ratio is disrupted, breast tissue proliferates.18,19 Gynecomastia may also be caused by hyperprolactinemia, which inhibits the secretion of gonadotropin-releasing hormone, resulting in the imbalance of androgens and oestrogen in breast tissue. 20 However, to date, there is only one case report of gynecomastia associated with GLM, and the relationship between gynecomastia and IGM is so far coincidental, with no defined aetiological relationship. In addition, there is not enough data to define prolactin levels and the association between gynecomastia and GLM.
Oestrogen stimulation is thought to promote acinar and lobule formation in the male breast. The cases of male IGM described in previous reports were from transgender male to female patients who were treated with oestrogen for 6 years. 21 In a further report, a 60-year-old patient with bilateral gynecomastia was described. 6 Geriatric gynecomastia may be associated with a higher ratio of oestradiol to testosterone, and may explain the older age of onset of GLM in males relative to females.
In the present case, ultrasound imaging was only applied at the first symptom onset and second onset of symptoms two years later, with lack of support from other imaging modalities. There was no similarity in the imaging performance at the two onsets, and only ultrasound imaging conducted at the second onset was consistent with previous studies, suggesting that male GLM might show hypoechoic masses in ultrasound imaging.
With regard to treatment, after communicating with the patient, he showed strong opposition to glucocorticoid treatment after knowing the side-effects of hormone therapy. Considering the small extent of the mass with formation of the abscess, treatment by incision and drainage was applied to the lesions at the first and the second relapse visit. Following this treatment, the patient self-administered medication at home and was lost to follow-up until a later time-point, when the patient reported that the lesion had healed during a follow-up phone call.
In summary, this study describes a case of male GLM with ipsilateral recurrence and the appearance of gynecomastia.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231187815 - Supplemental material for Case report on gynecomastia with ipsilateral recurrence of granulomatous lobular mastitis
Supplemental material, sj-pdf-1-imr-10.1177_03000605231187815 for Case report on gynecomastia with ipsilateral recurrence of granulomatous lobular mastitis by Yao Ke Han, Wang Ting, Pan Ting, Xiao Bing Yv, Shu Ran Xi and Lyu Gang in Journal of International Medical Research
Footnotes
Author contributions
YKH was a major contributor in writing the manuscript. WT contributed to the collection and processing of data and images. PT, XBY, and SRX contributed to the discussion section of the case report. LG supervised the writing of the report and submission for publication, and contributed to the editing. All authors read and approved the final manuscript.
Data accessibility statement
All data generated or analysed during this study are included in this published article.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.