
Abstract
Objective
Type 2 diabetes mellitus (T2DM) is a main risk factor for development of cardiovascular diseases (CVDs) and endothelial dysfunction. This study aimed to investigate serum levels of soluble vascular cell adhesion molecule 1 (sVCAM-1), intercellular adhesion molecule 1 (sICAM-1), and endothelium selectin (sE-selectin) in T2DM patients with macrovascular complications.
Methods
A cross-sectional study of 21 controls, 30 T2DM patients without CVDs, and 30 T2DM patients with CVDs was conducted. Serum levels of soluble adhesion molecules including sVCAM-1, sICAM-1, and sE-selectin were determined using ELISA.
Results
Serum levels of sVCAM-1, sICAM-1, and sE-selectin were higher in T2DM patients than in controls. Levels of serum sVCAM-1 were higher in T2DM patients with CVDs compared with T2DM patients without CVDs. In T2DM patients with CVDs, significant positive associations were observed between sVCAM-1, sICAM-1, and sE-selectin levels (r = 0.575, p = 0.001 and r = 0.378, p = 0.040).
Conclusions
Circulating levels of soluble adhesion molecules were elevated in T2DM patients, regardless of whether the patients had cardiovascular complications. Only sVCAM-1 was considered a useful marker for the prediction of CVDs in T2DM patients.
Keywords
Introduction
Diabetes mellitus (DM) has been recognized as one of the most chronic endocrine illnesses. According to the International Diabetes Federation (IDF), approximately 425 million people worldwide, representing 8.8% of adults 20 to 79 years old, were living with diabetes in 2019. By 2045, this figure will rise to 629 million people. 1 Of individuals with type 2 diabetes mellitus (T2DM), 80% live in low- or middle-income countries. It is expected that roughly 439 million individuals will have T2DM by 2030. 1 T2DM prevalence differs by region. 2 According to the World Health Organization, the Kingdom of Saudi Arabia (KSA) has the seventh-highest DM prevalence globally and the second-highest prevalence in the Middle East. 3 The IDF has also listed the KSA among the 10 countries globally with the highest estimated prevalence of DM (16.2%). This figure is expected to rise to 20.8% by 2030. 4
Patients with uncontrolled and chronic DM experience high blood glucose levels, leading to oxidative stress and endothelial dysfunction due to inflammation. The complications of T2DM can be classified as acute or chronic. Acute complications include hyperglycemia, a hyperosmolar hypertonic nonketotic state, and diabetic ketoacidosis. Chronic complications include macrovascular, microvascular, and non-vascular difficulties. 5
Atherosclerosis is the most common macrovascular complication of T2DM, and endothelial injury and attachment of monocytes to endothelial cells are the earliest steps in atherosclerosis. Under normal conditions, vascular endothelial cells interact with few leukocytes. Upon activation, vascular endothelial cells express cell adhesion molecules (CAMs) that increase their stickiness, leading to attachment of leukocytes to the endothelium of blood vessels and causing cardiovascular diseases (CVDs) in diabetic patients. CAMs act as intermediators between chronic inflammation, endothelial dysfunction, and vascular diseases in diabetics and include members of the immunoglobulin superfamily (IgSF), integrins, cadherins, and selectins. Selectins comprise a group of carbohydrate-binding molecules that are expressed on the membrane of activated platelets, leukocytes, and endothelial cells in inflamed areas; E-selectin, L-selectin, and P-selectin are members of this family. E-selectin is expressed by activated endothelial cells. 6 Intracellular adhesion molecule 1 (ICAM-1) is an IgSF member and is expressed by endothelial cells and white blood cells upon stimulation by cytokines. ICAM-1 has five immunoglobulin-like domains, a transmembrane area, and a short cytoplasmic tail. 6 VCAM-1 is another IgSF member and is expressed by endothelial cells, smooth muscle cells, and macrophages following their activation by hyperglycemia or by various inflammatory cytokines including interleukin 1-β, tumor necrosis factor (TNF)–α, lipopolysaccharide, and Toll-like receptor agonists. 7 VCAM-1 mediates leukocyte interaction with endothelial cells via its interaction with very late antigen-4, which is expressed on monocytes and lymphocytes. In DM, perturbations of endothelial cells are partially due to the interactions between advanced glycation end-products and their receptors, thus leading to increased VCAM-1 expression. VCAM-1 is also involved in atherosclerotic plaque formation, and its soluble forms play an important role in retinopathy due to their proangiogenic action. 8
Early detection of elevated levels of endothelial biomarkers may help in the design of new strategies to mitigate CVD complications, as these biomarkers could enable early prediction of endothelial dysfunction and activation. Thus, this study aimed to measure serum levels of soluble (s) ICAM-1, VCAM-1, and E-selectin in T2DM patients with macrovascular complications. Serum levels of these CADs might reflect their expression by endothelial cells and their possible association with glucose and lipid metabolism parameters.
Subjects and methods
This cross-sectional study was conducted on 81 participants (both male and female) aged between 29 and 77 years old. The participants were categorized into three groups: healthy controls (n = 21), T2DM patients without CVDs (n = 30), and T2DM patients with CVDs (n = 30). The criteria of the American Diabetes Association were used to classify T2DM for all diabetic patients, and patients who had a fasting blood glucose (FBG) level of ≥7.0 mmol/L on two occasions were diagnosed with T2DM. 2 T2DM patients were selected by endocrinologists and cardiologists at King Abdul Aziz University Hospital, Jeddah, Saudi Arabia, between October 2017 and October 2018. Individuals with type 1 DM, cancer, or inflammatory diseases (e.g., gout, bronchial asthma, eczema, hepatitis, thyroiditis, allergic reactions, multiple sclerosis, rheumatoid arthritis, or ulcerative colitis) and individuals being treated with corticosteroids were excluded. The study was conducted in accordance with the principles laid out in the Declaration of Helsinki and was approved by the Ethics Committee of King Abdul Aziz University Hospital. Informed written consent was obtained from all participants.
The control group, consisting of individuals with normal oral glucose tolerance curves and no history of T2DM among first-degree relatives, were selected from blood donors, hospital staff, and healthy individuals from checkup clinics who fell within the same age range as T2DM patients. The healthy controls underwent the same anthropometric and biochemical evaluations as T2DM patients. The T2DM patients with CVDs had coronary heart diseases (n = 15), cerebrovascular diseases (n = 10), or peripheral vascular diseases (n = 5). Coronary heart diseases were detected in this group using electrocardiography, hospital reports of myocardium infarctions, bypass grafting of coronary arteries or angina pectoris. Cerebrovascular diseases were evaluated through clinical examinations and hospital reports of stroke. Peripheral vascular diseases were diagnosed by an infrequent history of claudication pain and by measuring the brachial pressure index of the ankle (normal value >0.9) using a Multi-Dopplex instrument (Huntleigh Nesbit Evans Healthcare, UK).
Among DM patients (n = 60), five individuals (8.33%) were managed by diet alone, 40 patients (66.67%) were managed using oral hypoglycemic drugs (a combination of sulfonylureas and biguanides or sulfonylureas), and 15 patients (25%) were managed using insulin. In total, 54 patients were hypertensive and received anti-hypertensive medication; 26 of these patients had T2DM without CVDs while 28 patients had T2DM with CVDs.
All participants underwent physical examinations and laboratory investigations before being included in this study. Their weight in kilograms and height in centimeters were recorded using a digital scale and stadiometer, and their body mass index (BMI) was also calculated. Clinical information (i.e., disease duration and medication usage) was obtained after the participants were interviewed.
Venous blood from the antecubital vein was obtained from the participants after overnight fasting. The blood was divided into a plain tube for serum separation and into ethylenediaminetetraacetic acid-coated tubes to obtain plasma for routine chemistry tests. The plasma and serum were obtained after centrifugation for 10 minutes at 3000 rpm (round per minute) and frozen at –80°C at King Fahd Center for Medical Research. FBG, hemoglobin A1c (HbA1c), high-density lipoprotein-cholesterol, total cholesterol and triglycerides were evaluated using available commercial kits. The estimated glomerular filtration rate (eGFR) was calculated using the Modification of Diet in Renal Disease Study GFR equation, which is based on serum creatinine values and patient characteristics. 9 Based on their eGFR levels, the patients were categorized into four stages as follows: stage I (≥90 mL/minute/1.73 m2), stage II (60–89 mL/minute /1.73 m2), stage IIIa (45–59 mL/minute/1.73 m2), stage IIIb (30–44 mL/minute/1.73 m2), and stage IV (15–29 mL/minute/1.73 m2). 9 Serum levels of sE-selectin (Cat # RAF098R), sICAM-1 (Cat # RAF102R), and sVCAM-1 (Cat # RAF118R) were quantitated using ELISA (BioVendor Research and Diagnostic Products, Brno, Czech Republic).
Statistical analyses were conducted using the Statistical Package for Social Sciences (SPSS), version 22 (IBM Corp., Armonk, NY, USA). Descriptive statistics included the mean (+/−) and standard deviation (SD) for continuous values and the number (%) for categorical values. A one-way analysis of variance (ANOVA) test was used to assess differences among the three groups. A least significant difference test was applied for continuous data. Pearson’s bivariate correlation coefficient was calculated to detect associations between variables and levels of soluble adhesion molecules. Values of P <0.05 were considered statistically significant.
Results
Eighty-one participants (43 men and 38 women) were divided into three groups according to their medical condition. Of the men who participated in this study, 11 (52.38%) were controls, 9 (30.00%) had T2DM without CVDs, and 23 (76.67%) had T2DM with CVDs. Of the women who participated, 10 (47.62%) were controls, 21 (70.00%) had T2DM without CVDs, and 7 (23.33%) had T2DM with CVDs. The mean BMI (kg/m2) was higher in the T2DM without CVDs group than in the control group (p = 0.003), while disease duration was longer in patients with T2DM with CVDs compared with patients with T2DM without CVDs (p = 0.001). Fifty-four patients were hypertensive and received anti-hypertensive medication, representing 26 (86.7%) individuals with T2DM without CVDs and 28 (93.3%) individuals with T2DM with CVDs (Table 1).
Demographic data of the study participants.

Data were expressed as means +/− SDs or number (%) as appropriate. CVDs: cardiovascular diseases; T2DM: type 2 diabetes mellitus; BMI: body mass index; 1p: significance versus control; 2p: significance versus T2DM without CVD.
FBG and HbA1c levels were higher in patients in both T2DM groups compared with the control group (both p = 0.001), and FBG levels were higher in the T2DM with CVDs group compared with the T2DM without CVDs group (p = 0.014). Total cholesterol levels were higher in both T2DM groups compared with the control group (T2DM with CVDs: p = 0.013; 2DM without CVDs: p = 0.001), and were higher in patients without CVDs compared with patients with CVDs (p = 0.001). There were no significant changes in serum albumin between the three groups. Serum creatinine was significantly higher in both T2DM groups compared with the control group (T2DM with CVDs: p = 0.0001; T2DM without CVDs: p = 0.013). Serum creatinine was significantly higher in the T2DM with CVDs group compared with the T2DM without CVDs group (p = 0.004). eGFR was significantly higher in both T2DM groups compared with the control group (both p = 0.0001). We analyzed the distributions of eGFR levels and found that individuals with T2DM without CVDs group were staged as follows: stage I (n = 16, 26.7%), stage II (n = 18, 60.0%), stage IIIa (n = 2, 6.7%), and stage IIIb (n = 2, 6.7%). Similarly, individuals in the T2DM with CVDs group were staged as follows: stage I (n = 5, 16.7%), stage II (n = 18, 60.0%), stage IIIa (n = 2, 6.7%), stage IIIb (n = 4, 13.3%), and stage IV (n = 1, 3.3%). Serum levels of sICAM-1, sVCAM-1, and sE-selectin were significantly higher in T2DM patients with and without CVDs compared with the control group, while sVCAM-1 levels were higher in the T2DM with CVDs group than in the T2DM without CVDs group (p = 0.037) (Table 2).
Comparison of measured biomarkers in different groups.
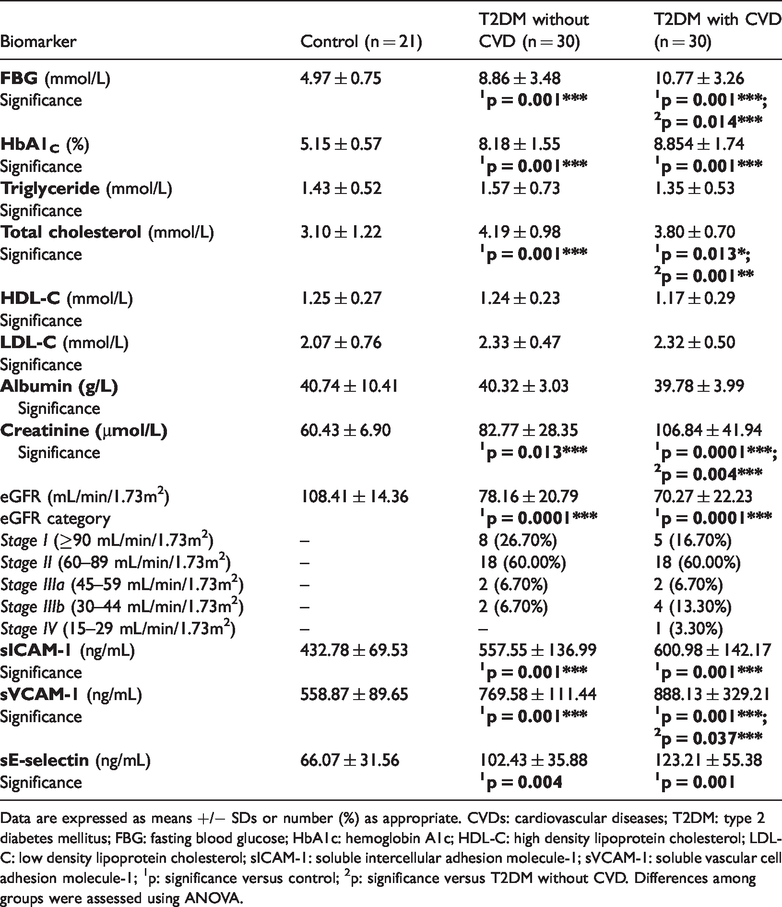
Data are expressed as means +/− SDs or number (%) as appropriate. CVDs: cardiovascular diseases; T2DM: type 2 diabetes mellitus; FBG: fasting blood glucose; HbA1c: hemoglobin A1c; HDL-C: high density lipoprotein cholesterol; LDL-C: low density lipoprotein cholesterol; sICAM-1: soluble intercellular adhesion molecule-1; sVCAM-1: soluble vascular cell adhesion molecule-1; 1p: significance versus control; 2p: significance versus T2DM without CVD. Differences among groups were assessed using ANOVA.
In T2DM patients with CVDs, there were significant positive correlations between serum levels of sVCAM-1 and sICAM-1 (r = 0.575, p = 0.001) and between serum levels of sVCAM-1 and sE-selectin (r = 0.387, p = 0.040). This highlights the potential mechanistic association between these adhesion molecules and the factors that lead to their release (Table 3).
Correlation between serum CAM levels in T2DM patients without and with cardiovascular diseases.
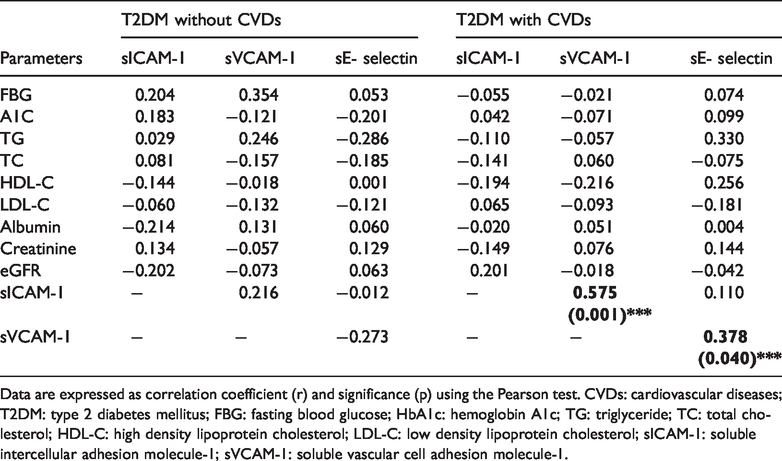
Data are expressed as correlation coefficient (r) and significance (p) using the Pearson test. CVDs: cardiovascular diseases; T2DM: type 2 diabetes mellitus; FBG: fasting blood glucose; HbA1c: hemoglobin A1c; TG: triglyceride; TC: total cholesterol; HDL-C: high density lipoprotein cholesterol; LDL-C: low density lipoprotein cholesterol; sICAM-1: soluble intercellular adhesion molecule-1; sVCAM-1: soluble vascular cell adhesion molecule-1.
Discussion
Hyperglycemia hastens atherogenesis and the occurrence of macrovascular diseases in diabetic patients. Meanwhile, risk factors for DM other than hyperglycemia play an important role in the development of macrovascular diseases. CAMs enhance the attachment of leukocytes to endothelial cells leading to acute and chronic inflammatory lesions of the blood vessel walls. This contributes to the development of CVDs. 10
In this study, elevated serum levels of sE-selectin were detected in both T2DM groups compared with the healthy control group. Our results agree with those of previous studies, which showed raised levels of sE-selectin in T2DM patients compared with control groups.6,11,12 We found no significant difference between sE-selectin serum levels in T2DM patients with and without CVDs. However, previous studies reported that sE-selectin concentrations were significantly increased in T2DM patients with CVDs compared with T2DM patients without CVDs.13,14 The high level of sE-selectin observed in both diabetic groups compared with controls may be due to endothelial activation and inflammation in response to hyperglycemia; this activation and inflammation may occur regardless the presence or absence of CVDs. 15 In 2014, Sandoval-Pinto et al. 16 evaluated serum levels of sE-selectin in 283 patients with acute coronary syndrome (ACS) and compared them with levels in 205 healthy subjects. They found that sE-selectin levels were significantly higher in ACS patients compared with controls (54.58 versus 40.41 ng/ml, p = 0.02). Positive associations between sE-selectin and oxidative stress, pro-inflammatory chemokines, dysfunctions of the endothelium, and the incidences of T2DM and CVD were also reported.17,18
In this study, sICAM-1 serum levels were higher in both T2DM groups compared with the control group. This finding could be explained by the effect of hyperglycemia, which causes endothelial dysfunction and inflammation and leads to stimulation of ICAM-1 expression. 15 Song et al. 12 showed that there was a significantly higher sICAM-1 concentration in diabetic women compared with controls. However, we found no significant difference sICAM-1 levels in both diabetic groups in the present study. In agreement with our results, Matsumoto et al. 13 reported that sICAM-1 levels could not predict CVD events in T2DM patients. ICAM-1 and E-selectin levels, however, predicted carotid artery atherosclerosis. 19 The prospective Physicians Health Study implicated ICAM-1 in the occurrence of atherogenesis and coronary artery diseases. 20 Meanwhile, other studies have reported that sICAM-1 is associated with risk of angina pectoris and myocardial infarction. 21 sICAM-1 levels were associated with CVD mortality and morbidity in T2DM patients with diabetic nephropathy. 22 Elevated ICAM-1 levels were detected in the retinas of diabetic patients in the early stages of retinopathy, thus suggesting that ICAM-1 is accountable for the adhesion and trans-endothelial movement of circulating leukocytes through the retinal vessel walls. 23 ICAM-1 may primarily more to microangiopathy rather than macroangiopathy, which is associated with chronic hyperglycemia due to insulin resistance. 24
In agreement with the results of our study, most of the extant literature has shown that sVCAM-1 levels are elevated in T2DM subjects compared with nondiabetic subjects.6,12,20,25 However, this consensus has not been unanimous.26,27 Hyperglycemia is responsible for changes to endothelial cell functions, thus leading to elevated sVCAM-1 concentrations. We also found that sVCAM-1 serum levels were significantly higher in T2DM patients with macrovascular complications compared with those without complications. ICAM-1 and VCAM-1 levels have been found to increase in patients with peripheral arterial diseases and hypercholesterolaemia. 28 Endothelial cells isolated from patients with DM expressed higher levels of VCAM-1 than ICAM-1 when stimulated by cytokines in a high-glucose microenvironment.15,29 In this respect, it was reported that sICAM-1 and sVCAM-1 concentrations were both elevated in T2DM patients. However, plasma sVCAM-1 but not sICAM-1 was independently positively correlated with diabetic kidney diseases, indicating that sICAM-1 and sVCAM-1 play different roles at different stages of the same disease. 23 Cross-sectional studies showed that sVCAM-1 levels were positively associated with the intima-media thickness of the carotid artery.30,31 Studies also showed that sVCAM-1 levels were positively associated with peripheral arterial disease severity, which was assessed using angiography. 32 sVCAM-1 in T2DM subjects was independently and markedly correlated with CVDs and all-cause mortality. 33 sVCAM-1 levels also correlated positively with atherosclerosis in the early stages of T2DM. 34 In contrast to our results, Matsumoto et al. 13 suggested that sVCAM-1 levels were not predictive of CVD in T2DM patients. In a large cohort of healthy men, de Lemos et al. 35 concluded that sVCAM-1 levels were not correlated with risk of later infarction of myocardial tissue. In prospective studies, however, elevated sVCAM-1 levels were not related to cardiovascular risk events.19,28 This finding is in contrast to the results of other studies of CAMs, such as ICAM-1 and E-selectin.19,20 These differences may be because of the small sample sizes or the absence of information on complications and classification.
Studies have shown that VCAM-1 and ICAM-1 differ in their tissue distribution, their specificity for receptors, and their responses to inflammatory cytokines. Endotoxins stimulate more ICAM-1 and VCAM-1 expression in cells of the endothelium and stimulate p38 expression; PTEN/Akt and protein kinase C were primed to induce VCAM-1 expression but not ICAM-1 expression. 36 Meanwhile, ERK-1/2 stimulation is required for TNF-α stimulation of ICAM-1 over-expression in endothelial cells. 37 These results suggest that VCAM-1 and ICAM-1 had different levels of participation at different stages of the same disease (T2DM).
Potential explanations for the variable associations of VCAM-1, ICAM-1, and E-selectin levels with CVDs include the following. First, in vitro studies reported that endothelial cells isolated from patients with DM express more VCAM-1 than ICAM-1 when stimulated by inflammatory cytokines in high glucose media. 38 In CVD patients, endothelial cells trigger VCAM-1 expression due to increased inflammation levels. Second, elevated plasma VCAM-1 levels occur along with elevation of VCAM-1 membrane expression at the atherosclerotic plaque on the neo-vasculature bed. Thus, increased VCAM-1 levels in CVD patients may reflect higher atherosclerotic pathology compared with patients without CVD.
In this study, sVCAM-1 levels were positively correlated with sICAM-1 and sE-selectin levels in T2DM patients with CVDs, thus reflecting inflammatory changes of the endothelium. Although individual CAM levels were correlated to various degrees in this study, their origins and methods of stimulation differ. Because the release of E-selectin and VCAM-1 were almost solely restricted to endothelial cells, their elevated serum concentrations seem to more reliably reflect endothelial activation and vascular endothelial damage than sICAM-1, which is associated with lymphocyte activation and non-endothelial tissue injury. 39
Conclusion
This study found an elevation in all endothelial cell dysfunction markers (i.e., sICAM-1, sVCAM-1, and sE-selectin) in T2DM patients, regardless of the presence or absence of CVDs. Serum levels of sVCAM-1 were significantly increased in T2DM patients with CVDs compared with T2DM patients without CVDs. Meanwhile, levels of sICAM-1 and sE-selectin did not differ between these two groups. Strong positive correlations between levels of sVCAM-1 and both sICAM and sE-selectin in T2DM patients with CVDs suggest that a dysfunctional endothelium leads to increased expression of these markers. Thus, sVCAM-1 could be considered a useful biomarker for prediction of CVD events in T2DM patients. More studies on endothelial biomarkers are recommended to decipher the mechanisms that may be involved in vascular complications during T2DM. The association between sVCAM-1 and atherosclerotic plaque formation and intima-media thickness also requires further study. Understanding the relationship between VCAM-1 and blood vessel walls will help to establish new strategies to reduce CVD complications in T2DM patients.