
Abstract
Few cases of portal vein thrombosis secondary to gastric cancer surgery have been reported. Here we report the diagnosis and management of two such cases. Case 1: Gastric carcinoma with acute hematemesis was detected by endoscopy in the gastric body of a 48-year-old woman. Histologic examination revealed signet-ring cell carcinoma with marked invasion of the vessels and nerves. Laparoscopic partial gastrectomy and Roux-en-Y gastrogastrostomy were performed. One month after surgery, imaging examination showed the formation of thrombi in the main portal vein and the right hepatic vein. Case 2: Gastric carcinoma with pyloric obstruction was clinically diagnosed in a 66-year-old woman. Laparoscopic partial gastrectomy and Billroth Roux-en-Y gastrogastrostomy were again performed. Two months after surgery, an abdominal imaging examination detected a thrombus in the right hepatic vein. Clinicians should consider portal vein thrombosis in patients with hyperthermia combined with an abnormal increase in procalcitonin.
Keywords
Introduction
Several studies have described the occurrence of portal vein thrombosis in patients with liver cirrhosis and neoplasms of the pancreas and the liver. In terms of postoperative complications, however, few cases of portal vein thrombosis secondary to gastric cancer surgery have been reported and the condition is therefore underappreciated. We recently encountered two cases of portal vein thrombosis following gastric cancer surgery, which has raised our awareness of this condition as a severe complication after gastric cancer surgery.
Case reports
The study was approved by the institutional review board of The Affiliated Hospital of Inner Mongolia Medical University. Both patients provided written informed consent for their patient information and images to be published.
Case 1
A 48-year-old woman was admitted to our hospital with pain in the upper abdomen, substantial weight loss, and hematemesis. Laboratory examination showed a serum carcinoembryonic antigen (CEA) level of 41.53 ng/ml. All other laboratory tests were within the normal range. An auxiliary examination using a gastroscope revealed a lesion in the body of the stomach with a depressed shape (Figure 1a). Abdominal computed tomography (CT) revealed lymph node invasion of the surrounding gastric tissue. There were no signs of metastasis to the liver, spleen, or lungs. Preoperative staging was cT3N1M0, and a laparoscopic partial gastrectomy and Roux-en-Y gastrogastrostomy were performed after the preoperative assessment. Histological examination of the resected specimens showed tumor cells invasion of the serosa layer and lymph node metastasis in Stage II. Staging was updated to pT4aN2M0 Stage III B. The postoperative course was uneventful until day 5, when the patient abruptly developed a high-grade fever of 38.5°C without other specific symptoms. Laboratory examination showed an elevated C-reactive protein level (60.7 mg/L) and white blood cell count (11.34 × 109/L). An abdominal plane scan showed a slight anastomotic fistula in the lesser curvature of the stomach (Figure 1b). A diagnosis of abdominal cavity infection was made and antibiotic treatment was initiated (cefoperazone and sodium sulbactam; 3 g b.i.d intravenous infusion). The fever gradually subsided and the laboratory parameters slowly returned to normal without the patient developing further complications. The patient was discharged on postoperative day 15. In accordance with the Japanese Gastric Cancer Treatment Guidelines 2014 for SOX (S-1 plus oxaliplatin) regimens, oxaliplatin was administered by intravenous infusion at a dose of 130 mg/day for 1 day and S-1 was administered orally at a dose of 100 mg/day on day 2 to 14, followed by a 7-day drug-free period. After one course of chemotherapy, the patient abruptly developed a high-grade fever of 39.5°C along with chills, fatigue, and loss of appetite. The laboratory data showed elevated procalcitonin (93.17 ng/ml), white blood cell count (13.34 × 109/L), C-reactive protein (60.7 mg/L), D-dimer (1.17 μg/ml), and aspartate transaminase (46 IU/L), and a reduction in albumin (22.3 mg/L). Other laboratory data were normal. A contrast-enhanced CT showed a clot embolism along the main portal vein and the right hepatic vein (Figure 1c). Cefoperazone and sodium sulbactam (3 g, b.i.d, intravenous infusion) and low-molecular-weight heparin calcium (0.6 ml, b.i.d, s.c.) were immediately administered, and chemotherapy was discontinued. Two weeks later, the fever diminished and the laboratory data returned to normal. An imaging examination showed the appearance of a smaller clot and a cavernous transformation of the portal vein. The patient was discharged on oral rivaroxaban. During 6 months of follow up, no hepatic decompensation or liver cirrhosis was observed.

(a) Lesion in the body of the stomach with a depressed shape. (b) Anastomotic fistula in the lesser curvature of the stomach. (c) Portal vein thrombosis.
Case 2
A 66-year-old woman was admitted to a neighboring hospital with upper abdominal pain, heartburn, and vomiting. Gastroscopy and CT suggested Borrmann type 4 gastric carcinoma, and the pathological characteristics indicated adenocarcinoma. The patient was transferred to our hospital for surgery. The patient was in good condition. Tumor marker tests showed elevated CEA and alpha-fetoprotein (AFP) levels (41.53 ng/ml and 54.62 ng/ml, respectively). The blood cell counts and aspartate transaminase levels were normal. Following preoperative preparation, a laparoscopic partial gastrectomy and Roux-en-Y gastrogastrostomy were performed. Histological characteristics of the resected specimens indicated poorly differentiated adenocarcinoma along with tumor cell invasion of the serosa layer and lymph node metastasis to the greater curvature of the stomach. The disease was staged as pT4aN1M0 Stage IIIA. The postoperative course was uneventful. Before the patient was discharged from hospital, an abdominal CT showed a partial effusion in the lesser curvature of the stomach (Figure 2b). The patient was discharged on postoperative day 12 with no further discomfort. Three weeks later, the patient’s condition had improved and an abdominal CT showed that the partial effusion had disappeared. The patient was initiated on a SOX plan for chemotherapy. On day 13 after starting chemotherapy, the patient abruptly developed a high-grade fever of 39.3°C with chills, fatigue, and herpes simplex outbreaks around her mouth. Laboratory examination showed elevated procalcitonin (12.27 ng/ml), white blood cell count (2.9 × 109/L), C-reactive protein (98.2 mg/L), and D-dimer (2.4 μg/ml), and reduced albumin (23.2 mg/L). Contrast-enhanced CT showed a thrombus located in the right hepatic vein and a small amount of ascites (Figure 2a, c, and d). Other data were normal. The patient was administered antibiotics and heparin, and after 6 days of treatment her fever had resolved and laboratory data were normal so the patient was discharged on oral rivaroxaban. Two weeks later, ultrasonography of the portal vein showed partial recanalization of the blood clots and a cavernous transformation around the portal vein. Follow-up is ongoing, and no evidence of hepatic decompensation or liver cirrhosis has been identified at 2 months.
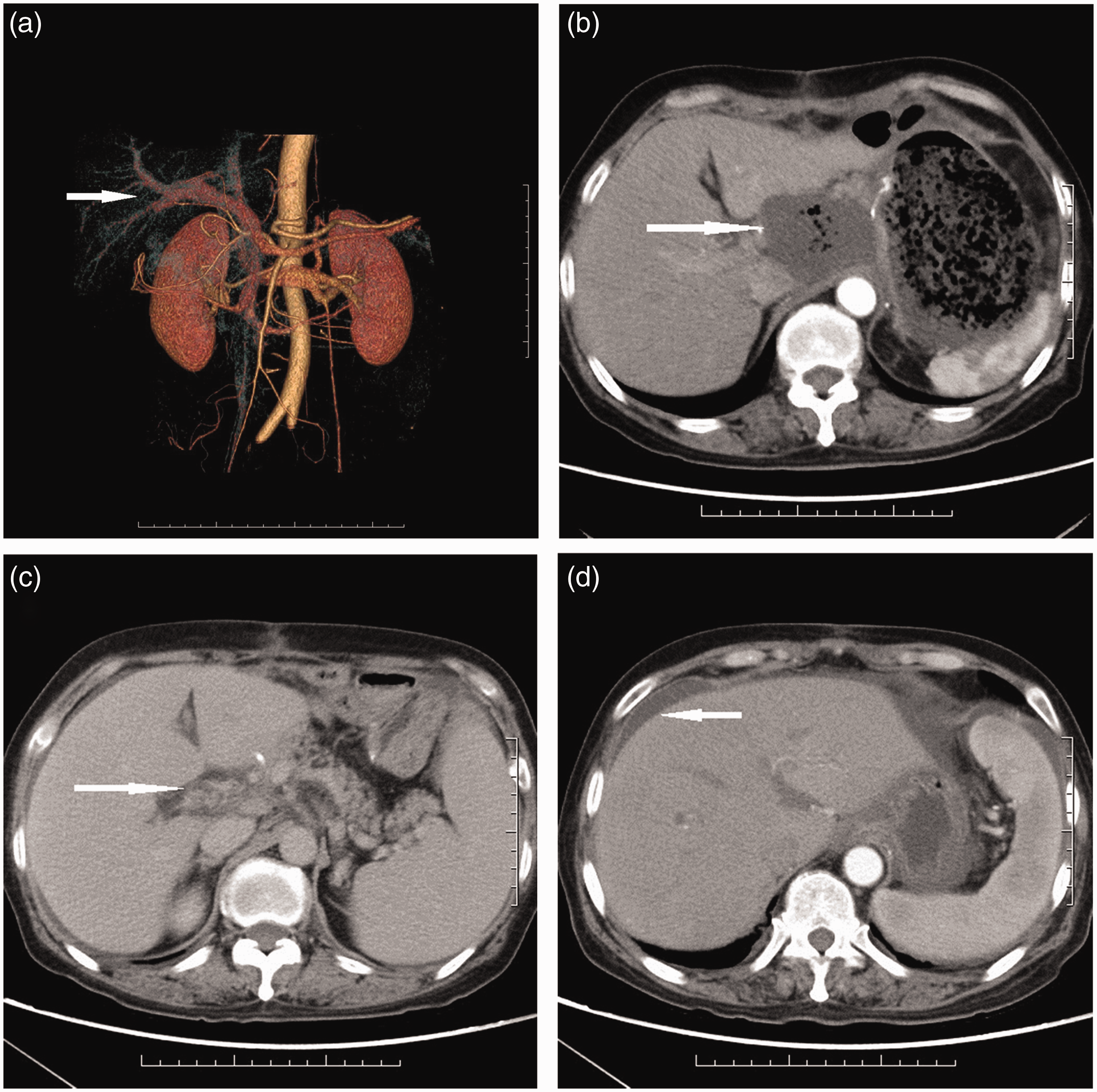
(a) Three-dimensional reconstruction of the portal vein. (b) Partial effusion in the lesser curvature of the stomach. (c) Portal vein thrombosis. (d) Ascites.
Discussion
Portal vein thrombosis refers to the formation of a thrombus within the extrahepatic main portal vein and/or intrahepatic portal vein branches. In terms of etiology, in addition to hyperhomocysteinemia, antiphospholipid syndrome, liver cirrhosis, and other diseases have been associated with thrombosis.1–3 Most studies linking portal vein thrombosis to postsurgical complications have focused on disease in the liver, spleen, or pancreas. 4 Portal vein thrombosis secondary to postoperative gastric cancer has rarely been reported. We recently identified two cases of portal vein thrombosis after gastric cancer surgery. Both patients were women with tumors located in the gastric body and distal stomach. Regarding preoperative staging, previous studies have reported a low detection rate with PET/CT because of low tracer accumulation in diffuse and mucinous tumor types and a significantly lower sensitivity compared with CT in the detection of local lymph node involvement,5–6 as well as a high cost. We therefore used CT in the management of these patients. Given their severe preoperative complications, both patients underwent laparoscopic partial gastrectomy following preoperative assessment. In the perioperative period, both patients developed high-grade fever. Abdominal CT showed an infection or effusion in the lesser curvature of the gastric tissue. After treatment, despite resolution of the infection and effusion and a return to normal eating and defecation habits, both patients again developed high-grade fever within 1 month after discharge. In subsequent laboratory tests, we specifically noted an abnormal elevation in procalcitonin. Procalcitonin is mainly used for evaluating the severity of infection, and there are no reports to date on whether portal vein thrombosis leads to an abnormal increase in procalcitonin.7–8 The diagnosis of portal vein thrombosis frequently uses color Doppler ultrasound, for reasons of precision and low cost. 9 In the two cases described here, abdominal contrast-enhanced CT was used preferentially as it performs better than color Doppler ultrasound in diagnosing digestive tract diseases and is equally capable of diagnosing portal vein thrombosis. 8 To the best of our knowledge, thrombus formation requires the presence of risk factors, namely Virchow’s triad of prothrombotic disorders, circulatory stasis, and vascular wall injury. 10 In a study by Regnault et al., 11 tumor cells were shown to release small molecules that can promote blood coagulation, damage vascular endothelial cells, and even cause vascular compression leading to circulatory stasis. Therefore, patients with tumors can easily develop clots. Other researchers have noted that laparoscopic surgery may lead to portal vein thrombosis attributable to elevated intra-abdominal pressure. 12 Ogrenet al. 13 reported that abdominal local infection was a risk factor for portal vein thrombosis; both patients described here had this underlying risk. However, there are no reports to date of portal vein thrombosis caused by chemotherapy. The cases reported here were of advanced gastric cancer that required regular postoperative adjuvant chemotherapy to delay tumor recurrence. However, the occurrence of portal vein thrombosis interrupted treatment. These cases demonstrate the seriousness of portal vein thrombosis secondary to postoperative gastric cancer. Previous studies have shown that anticoagulation therapy significantly increased the rate of portal vein recanalization without increasing the risk of bleeding. 14 We chose low-molecular-weight heparin calcium and rivaroxaban for anticoagulation, with satisfactory results. However, in gastric cancer patients with a high risk for portal vein thrombosis, management of the factors described above, particularly local infection, is more urgent than treatment. Although it remains unclear whether anticoagulation therapy should be used to prevent this serious postoperative complication, we consider this approach to be necessary based on our clinical experience.
In conclusion, the administration of anticoagulant drugs is necessary in postoperative gastric carcinoma patients with a high risk of portal vein thrombosis. The presence of portal vein thrombosis should be considered in patients with hyperthermia combined with an abnormal increase in procalcitonin.
Footnotes
Declaration of conflicting interest
The authors declare there is no conflict of interest.
Funding
This study was supported by grants from the National Natural Science Foundation of China (nos. 81260364 and 81860416); the National Clinical Key Specialist Construction Project in China (no. 2018); and the Natural Science Foundation of Inner Mongolian Autonomous Region, (no. 2017MS (LH) 0826).