
Abstract
Objective
To evaluate the apical surgery-related anatomy of two-rooted and three-rooted mandibular first molars (MFMs) in a Mongoloid population.
Methods
A total of 502 cone-beam computed tomographic images were used to evaluate the root configuration, the distance from the buccal bone to each root, root dimensions, and the complete root resection distance at the resection level for roots of MFMs.
Results
The prevalence of two-rooted and three-rooted MFMs was 85.1% and 14.9%, respectively. At the resection level, the distance from the buccal bone to the mesial and distal roots of two-rooted MFMs was 2.24 and 3.15 mm, respectively, while the distance was 2.44, 2.01, and 8.55 mm for the mesial, distobuccal, and distolingual roots of three-rooted MFMs, respectively. The distance from the buccal bone to each root was longer in men than in women. The largest distance for complete root resection was detected for the distal root in two-rooted MFMs and for the distolingual root in three-rooted MFMs.
Conclusions
The prevalence of three-rooted MFMs is common in the Mongoloid population. The distance from the buccal bone to root apex differs according to root configurations and sex. Surgical access to the distolingual root is difficult because of the long access distance.
Keywords
Introduction
Periapical microsurgery is usually performed after failure of endodontic retreatment.1,2 However, endodontic microsurgery is challenging in the mandibular first molars (MFMs) because of the limited space, the thick buccal bone plate, and the proximity of teeth apices to the mandibular canal. These factors may cause serious complications, such as the need for anesthesia or paresthesia.3–5 More comprehensive knowledge of the bony architecture around the MFMs, such as the distance from the buccal cortical bone to each root and the vertical distance from the root apex to the inferior alveolar nerve are prerequisites, not only for efficient osteotomy and resection, but also for planning the surgical approach
Radiological examinations are often used as a preoperative diagnostic tool to provide insight of the operative site before surgery. Cone-beam computed tomography (CBCT) provides more accurate three-dimensional (3D) images by eliminating superimpositions and distortions compared with 2D radiography.3,6,7 The use of CBCT allows comprehensive analysis of the bone structure and its relationship to the mandibular canal in the mandibular molar region before periapical microsurgery. 8
The MFM is the most frequently endodontically treated tooth and its anatomy is extremely challenging.9,10 MFMs typically have two roots located mesiodistally and three root canals. 11 Several studies have suggested that the morphology of MFMs varies according to ethnicity. MFMs with an extra distolingual root in Mongoloid populations are the most common variant.12–15 The prevalence of MFMs with an extra distolingual root in the Asian population is as high as 17.8% to 29.0%, while this prevalence is 0.7% to 4.2% in those of Caucasian heritage.16–20
At least 3 mm of the root end must be resected to remove 98% of the apical ramifications and 93% of the lateral canals. 21 The distance from the buccal bone to each root at the surgical resection level is important in treatment planning for endodontic microsurgery. 22 At the root resection level, the distance from the buccal bone to each root of two-rooted MFMs among Western populations has been reported.4,5 For three-rooted MFMs, the extra distolingual root is usually small, curved, and located far from the buccal bone plate. Zhang et al. 23 evaluated the surgical access distance from the distolingual root apex to the buccal bone plate surface in MFMs.
Currently, no study has assessed the distance from the buccal bone to each root of three-rooted MFMs at the resection level using CBCT. Therefore, this study aimed to evaluate the distance from the buccal bone to each root in two-rooted and three-rooted MFMs at the apical level and at the root resection level in a Mongoloid population to provide guidance for endodontic surgery. The root dimensions of MFMs at the resection level and the complete resection distance were also investigated. Knowledge of the prevalence of a distolingual root and apical surgery-related anatomy of MFMs is important for planning surgical access and improving the success rate of endodontic microsurgery for MFMs, especially when CBCT is not easily available.
Materials and methods
Subjects
The study was approved by the Ethics Committee of the Hospital of Stomatology, Sun Yat-sen University, Guangzhou, China (ERC-2017-09). Consent of patients was not required because the present study was a retrospective and descriptive study of archival radiographs without therapeutic intervention. A total of 697 CBCT images were randomly selected from an archive of images with a field of view of 16 × 7 cm and a voxel size of 0.20 mm. These images were sufficient for displaying the complete upper and lower dentition and were of adequately high resolution. These CBCT scans had been taken for diagnostic purposes by several different departments, including endodontics, oral surgery, prosthetics, and orthodontics in the Hospital of Stomatology, Sun Yat-sen University from 2010 to 2017.
The inclusion criterion was any existing MFMs. CBCT images were excluded from this study for the following reasons: (1) the mandible had congenital deformities; (2) the apices of MFMs were not fully formed; (3) MFMs were associated with a cyst, trauma, tumors, resorption, periapical lesions, or severe bone loss in the region of interest; and (4) the patient had formerly undergone orthodontic treatment.4,5,24
Only one MFM from each patient was selected in this study to avoid the potential for selection bias. Therefore, when both right and left MFMs of the same patient satisfied the criteria mentioned above, only one MFM was randomly included.
Imaging procedure
All images were acquired by using a CBCT scanner (DCTPRO; VATECH, Yongin-Si, Republic of Korea). The operating parameters were set at 90.0 kV and 9 mA with a scanning time of 24 seconds. The measurements were made using Ez3D 2009 software (Vatech Corporation, Hwaseong-si, Gyeonggi-do, Republic of Korea).
Radiographic assessment
All images of MFMs were evaluated in axial and coronal planes to assess the distance from the buccal bone to the root and the root thickness in buccolingual and mesiodistal directions. The following data were measured and determined. (1) The root configurations of MFMs were investigated and classified as two-rooted or three-rooted MFMs (Figure 1). (2) The distance from the buccal bone to the root apex was determined. At the level of the root apex in the axial view, the distance was recorded from the center of the apex perpendicular to the external part of the cortex (Figure 2a). The apex was identified on a 1-mm cross-sectional axial image when the last root apex was observed on each previous cross section, but it was no longer seen in the next image. 25 (3) The distance from the buccal bone to each root at the resection level was determined. A line of 3 mm was drawn from the root apex along the longitudinal axis of the root in CBCT in the coronal plane (Figure 2b). After the root resection level was obtained, the distance was determined from the most convex part of the root surface perpendicular to the external part of the cortical bone on the axial plane (Figure 2c). 5 (4) The thickness of the roots of MFMs at the root resection level was determined. The measurements of the mesiodistal and buccolingual root dimensions were assessed at the level of root resection on the axial view. The mesiodistal and buccolingual widths were recorded between the most convex parts of the root (Figure 2d). 5
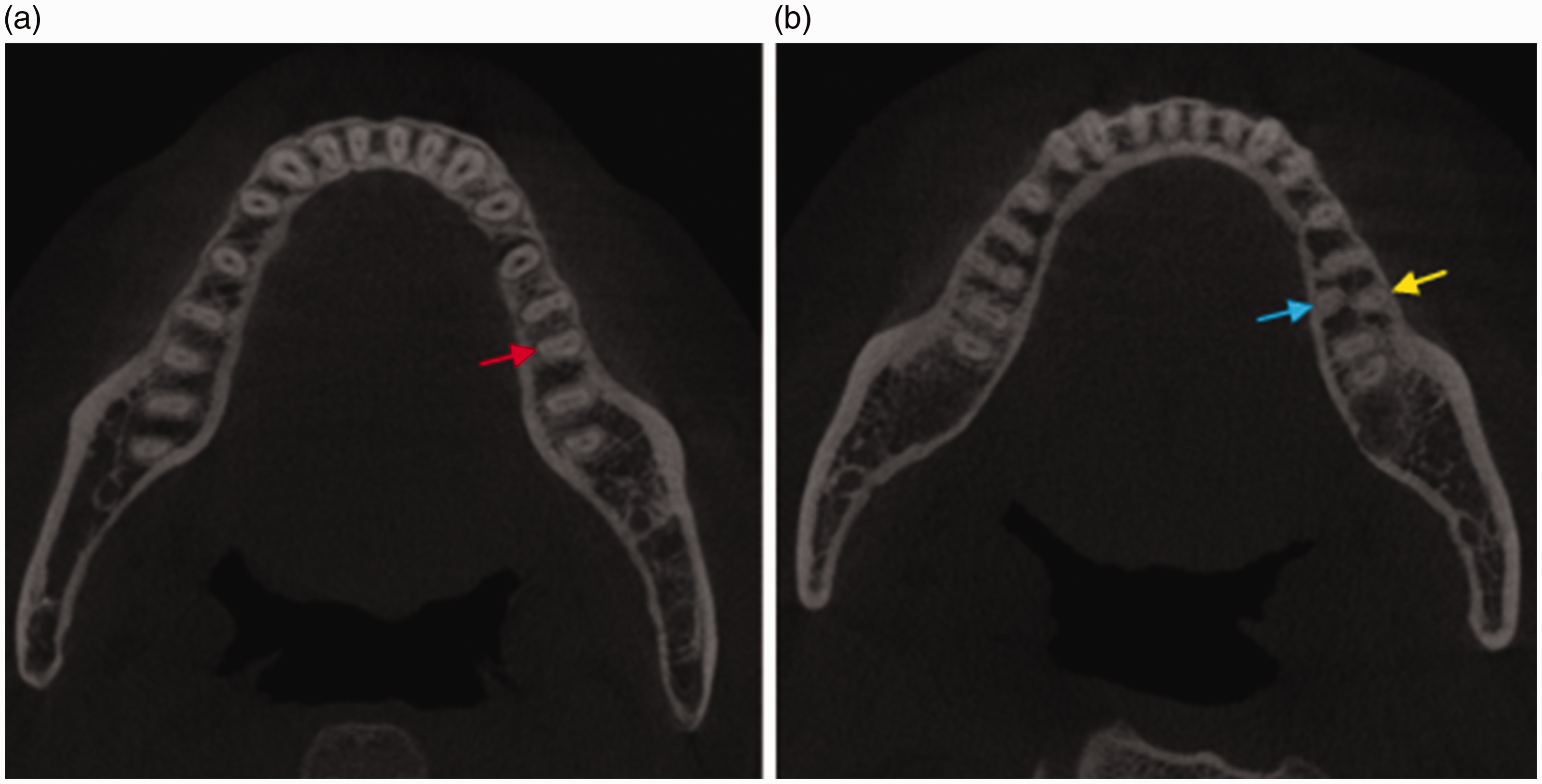
Different root configurations of mandibular first molars in the axial plane. (a) Two-rooted mandibular first molar with mesial and distal roots (red arrow). (b) Three-rooted mandibular first molar with mesial, distobuccal (yellow arrow), and distolingual roots (blue arrow).
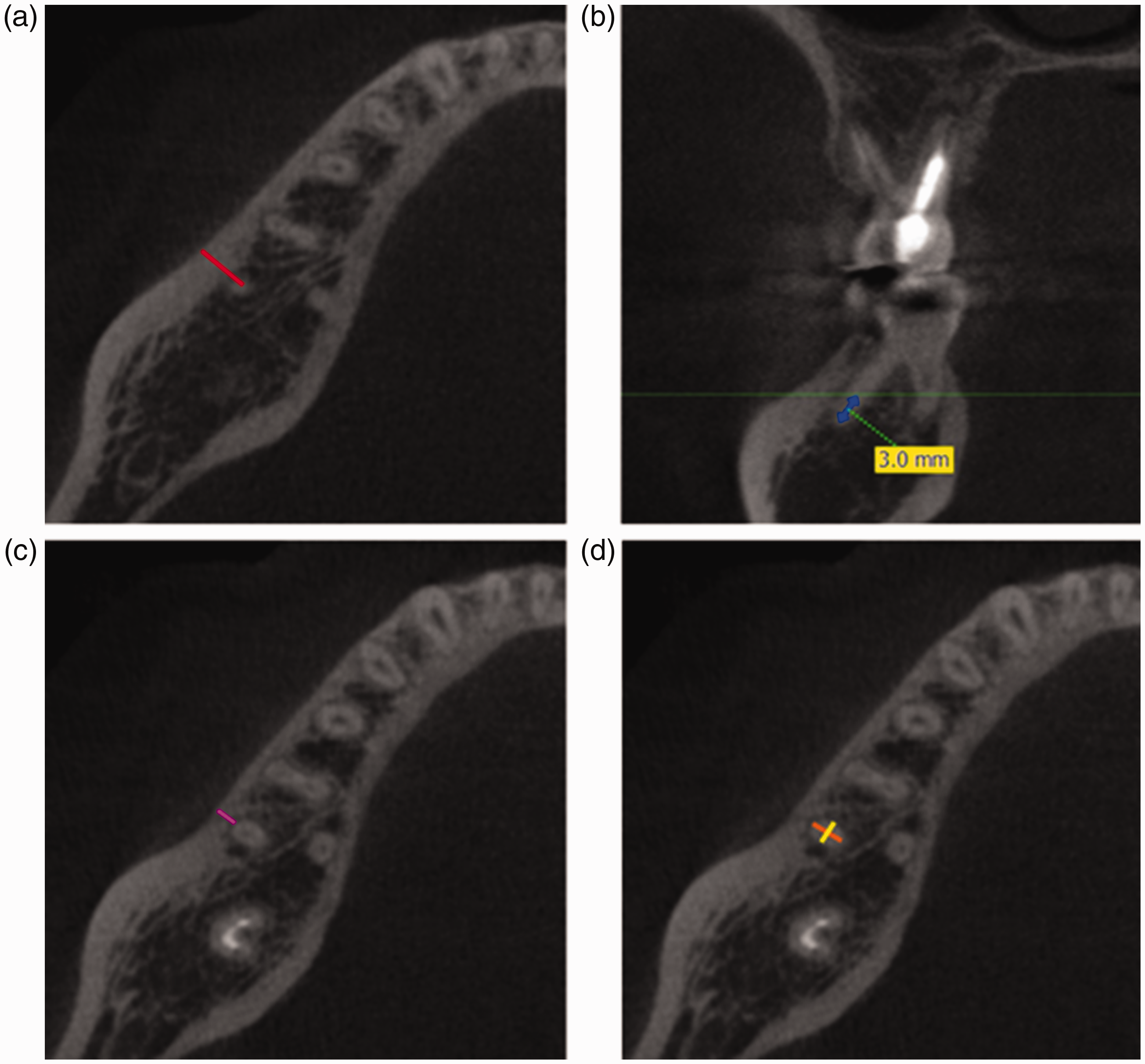
Measurements of the distance from the buccal bone to the root apex and root dimensions. (a) The distance from the buccal bone to the root apex was measured from the apex to the buccal bone plate in the axial plane (red line). 25 (b) A line of 3 mm was drawn from the root apex along the longitudinal axis of the root in the coronal plane of cone-beam computed tomography. (c) The distance from the buccal bone to the root at the resection level was measured in the axial plane (purple line). (d) In the axial plane, the mesiodistal (yellow line) and buccolingual (orange line) widths of the root were measured at the resection level. 5
Two observers assessed the images. The two observers evaluated 10% of the CBCT scans at the beginning of the study for standardization. Each measurement was carried out by the two observers independently. If the difference of assessment between the two observers was more than 2 mm, they reviewed the image again to reach a final agreement. During the evaluation, the observers were allowed to magnify the images or use enhancement filters to change the density, contrast, or brightness of the images. After the measurements were finished, 10% of the CBCT scans were re-evaluated by the two observers. The intra-observer and inter-observer reliability were evaluated by computing the intraclass correlation coefficient.
Statistical analysis
Data were analyzed using SPSS software, version 25.0 for Windows (IBM Corp., Armonk, NY, USA). The means and standard deviations of the distances from the buccal bone to each root and the root dimensions are shown using descriptive statistics. To compare the distance from the buccal bone to each root and root dimensions according to sex or root configurations, the independent samples t test and one-way analysis of variance with the post-hoc Bonferroni test were used. P values of <0.05 were considered as statistically significant.
Results
CBCT scans of 502 patients (228 men and 274 women) were included, with an average age of 38 years (range, 16–81 years). A total of 502 MFMs were assessed (427 two-rooted and 75 three-rooted MFMs; 237 of the left and 265 of the right mandible). The prevalence of two-rooted MTMs was 85.1% and that of three-rooted MFMs was 14.9%. The frequency distribution of root configuration was not significantly different between men and women (P = 0.322). According to the intraclass correlation coefficient for evaluation of intra- and inter-observer reliability, the levels of agreement of intra- and inter-observers were >0.89 and >0.82, respectively.
Distance from the buccal bone to the root apex and to each root at the resection level
Table 1 shows the means and standard deviations of the distance from the buccal bone to the root. Men had a longer distance from the buccal bone to each root than women, both at the apical level and at the resection level. This difference was significant for the mesial root at three-rooted MFMs at the apical level, for the mesial root at two-rooted MFMs at the resection level, and for the distolingual root at three-rooted MFMs at the resection level (all P < 0.05). Figure 3 shows the distance from the buccal bone to each root according to the root configuration. The distance from the buccal bone to the distolingual root of three-rooted MFMs was longer than that to the distal root of two-rooted MFMs and to the distobuccal root of three-rooted MFMs, both at the apex and at the resection level in men and women (Figure 3a–3d, all P < 0.01). The distance from the buccal bone to the mesial root apex of two-rooted MFMs was thinner than that of three-rooted MFMs in men (Figure 3a, P < 0.05).
Distance (mm) from the buccal bone to the root apex and to the root surface at the resection level.

Values are mean ± standard deviation. Different superscript letters indicate a significant difference in the same column according to the independent samples t test (P<0.05).
MR, mesial root; DR, distal root; DB, distobuccal root; DL, distolingual root; R2, two-rooted mandibular first molars; R3, three-rooted mandibular first molars.

Distance from the buccal bone to the root (mm) at different levels. (a) Measurements for the distance from the buccal bone to the root apex in men. (b) Measurements for the distance from the buccal bone to the root apex in women. (c) Measurements for the distance from the buccal bone to the root at the resection level in men. (d) Measurements for the distance from the buccal bone to the root at the resection level in women. MR, mesial root; DR, distal root; DB, distobuccal root; DL, distolingual root; R2, two-rooted mandibular first molars; R3, three-rooted mandibular first molars. *P < 0.05, **P < 0.01.
Root dimensions at the resection level
Table 2 shows the dimensions of each root of MFMs at the resection level. The distolingual root had the smallest dimension in both the mesiodistal and buccolingual directions among the three roots of three-rooted MFMs. For two-rooted MFMs, the buccolingual width was larger than the mesiodistal width in both the mesial and distal roots. For three-rooted MFMs, the buccolingual width was also larger than the mesiodistal width in the mesial root and distobuccal root, while the root dimensions in these two directions were relatively close for the distolingual root. However, none of these differences were significant. The mesiodistal and buccolingual widths of each root were not significantly different between men and women.
Mesiodistal and buccolingual root dimensions (mm) at the resection level.

Values are mean ± standard deviation. MFMs, mandibular first molars; MR, mesial root; DR, distal root; DB, distobuccal root; DL, distolingual root; M-D, mesiodistal width; B-L, buccolingual width.
Complete resection distance
The complete resection distance at the resection level was determined by combining the distance from the buccal cortical bone to the root surface and the buccolingual width of the root (Figure 4). For two-rooted MFMs, the mean value of the complete resection distance was greater for the distal root (8.54 mm) than for the mesial root (7.90 mm). For three-rooted MFMs, the greatest complete width of resection was for the distolingual root (11.30 mm), followed by the complete resection distance for the mesial root (7.98 mm), and distobuccal root (5.93 mm). Generally, regardless of root configurations, men had a greater mean value of the complete resection distance than did women for each root.
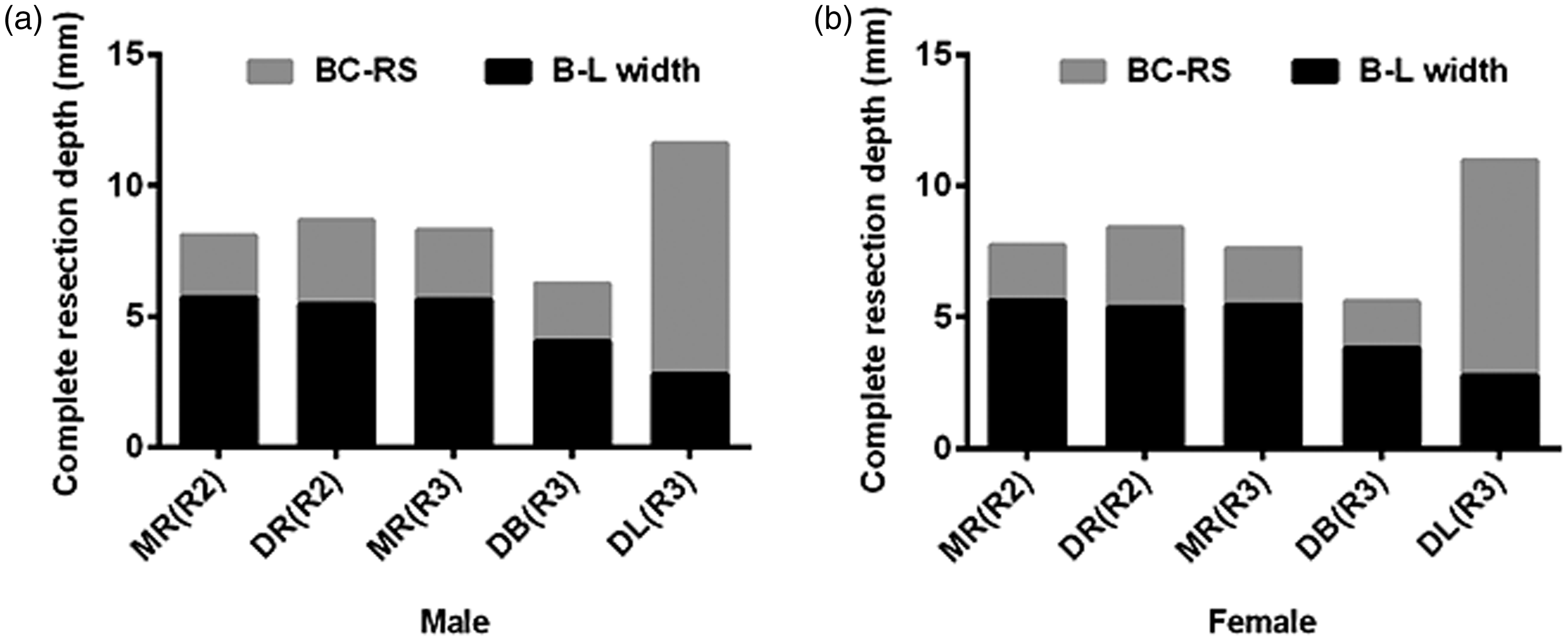
Complete resection depth (mm) of each root of mandibular first molars at the resection level. (a) Measurements for complete buccal resection of each root of mandibular first molars in men. (b) Measurements for complete buccal resection of each root of mandibular first molars in women. MR, mesial root; DR, distal root; DB, distobuccal root; DL, distolingual root; R2, two-rooted mandibular first molars; R3, three-rooted mandibular first molars; BC-RS, buccal cortex to the root surface; B-L width, buccolingual width.
Discussion
The distance from the buccal bone to the root surface is an important factors that should be taken into consideration before endodontic surgery in the posterior mandibular region.3–5,25 Few studies have evaluated the bony structures around MFMs in different populations.4,5,26 In these studies, the distance from the buccal bone to each root at the resection level in two-rooted MFMs was reported in Iranian, Turkish, and Saudi populations. Our study evaluated the distance from the buccal bone to each root at the resection level for two-rooted and three-rooted MFMs. For two-rooted MFMs in our study, the distance from the buccal bone to the root at the resection level was 2.24 and 3.15 mm for the mesial and distal roots, respectively. This distance was 1.43 and 2.57 mm on the left side and 1.66 and 2.76 mm on the right side, respectively, in the Iranian population. 4 In the Turkish population, this distance was 2.59 mm for the mesial root and 4.39 mm for the distal root on the left side (1.91 and 3.66 mm on the right side, respectively). 5 Aljarbou et al. reported that the distance from buccal bone to the root was 2.33 mm for the mesial root and 3.49 mm for the distal root in the Saudi population. 26 The distance from buccal bone to the mesial and distal roots was found to be shortest in the Iranian population, whereas the distance from buccal bone to the distal root in the Turkish population was greatest among these populations.4,5,26 These discrepancies are likely due to ethnic genetic differences, varying bone thicknesses, and distinctive topographical and anatomical relationships. 27 In all of these reports, the distance from the buccal bone to the distal root was longer than to the mesial root in two-rooted MFMs. This finding indicates that buccal bone thickness increases with posterior movement in the mandible because of the proximity to the external oblique ridge. 5 Therefore, access to the distal root is more difficult than that to the mesial root in apical surgery of two-rooted MFMs.
During endodontic surgery, the apical part of the tooth root should be removed to eliminate the ramifications and lateral canals, which are likely to harbor infection. For two-rooted MFMs, the buccolingual dimension of the mesial root was 5.66 mm in this Mongoloid population. This value is similar to that reported in the Iranian population and Turkish population.4,5 However, the buccolingual dimension of the distal root (5.39 mm) in our study is larger than those reported in the Iranian population (4.84 and 4.68 mm on the left and right sides, respectively) and in the Turkish population (4.42 and 4.54 mm on the left and right sides, respectively).4,5 In our study, the complete resection distance for the mesial root in two-rooted MFMs is similar to values reported in other populations.4,5 This distance was also similar to the distance for the mesial root in three-rooted MFMs. The complete resection distance of the distobuccal root of three-rooted MFMs (5.93 mm) was smaller than that of distal root of two-rooted MFMs (8.54 mm). Notably, the greatest complete resection distance of the distolingual root (11.30 mm) might pose a challenge to endodontic surgery for the distolingual root of three-rooted MFMs.
In this Mongoloid population, at the apical level, the distance from buccal bone to the root apex was 5.89, 4.63, and 9.96 mm for the mesial, distobuccal, and distolingual roots, respectively, of three-rooted MFMs, which are similar to those reported in a Korean population. 25 At the resection level, this distance was 2.44, 2.01, and 8.55 mm for the mesial, distobuccal, and distolingual roots, respectively, in the present study. When comparing the distance from the buccal bone plate to each root at the apical and resection levels, the distance at the apical level appears to be relatively greater than that at the resection level, which is in agreement with a study by Lavasani et al. 22
In the current study, the distance from buccal cortical bone to each root was longer in men than in women, regardless of the configuration of MFMs. However, this difference was not significant for some roots, which is consistent with other studies.4,25 Men also had a larger resection distance than did women, which might be explained by the generally thicker and bigger skeleton of men compared with women. Surgeons planning apical surgery are advised to be aware of these differences between sexes.
The distance from the distolingual root surface to buccal bone in our study was determined as the shortest distance between them, which could provide a reference for apical surgery. However, in practice, because endodontists operate through either the mesial or distobuccal root apex to access the distolingual root apex, the distance from the distolingual root surface to the buccal bone opposite the mesial or distobuccal root could be used to guide clinical treatment. 23 This distance would be better for guiding clinical treatment than the vertical distance measured in our study. In a recent study, Zhang et al. 23 proposed a new classification for distolingual roots based on root curvature using CBCT and discussed the feasible surgical access for different types of distolingual roots. The root of type I was inappropriate for apical surgery. The root of type II should be operated on through the distobuccal root apex, while access to the type III root should be through the mesial root apex. Overall, endodontists should bear in mind that a careful approach is required in apical surgery for MFMs with a separate distolingual root.
In conclusion, three-rooted MFMs with an extra distolingual root are common in the Mongoloid population. The distance from the buccal bone to the root apex of MFMs differs according to root configurations and sex. A separate distolingual root is located more lingual than the other roots, indicating that a careful approach is required in apical surgery. Knowledge of the prevalence of a distolingual root and apical surgery-related anatomy of MFMs can improve the success rate of endodontic microsurgery for MFMs.