
Abstract
Introduction
Although the effects of U2 small nuclear RNA auxiliary factor 1 gene (U2AF1) mutations on the outcomes of patients with myelodysplastic syndromes (MDS) have previously been investigated, their prognostic significance remains controversial. We performed a meta-analysis to investigate the impact of U2AF1 mutations on MDS progression.
Methods
Two reviewers independently extracted information such as hazard ratios (HRs) and 95% confidential intervals (CIs) for overall survival (OS) and leukemia-free survival (LFS) as well as the number of surviving patients each year after diagnosis from the included studies.
Results
Thirteen studies with a total of 3038 patients were included. The summary odds ratio (OR) for U2AF1 mutations with an OS of 5 years was 0.37, the summary HR for U2AF1 mutations in OS was 1.60, and the summary OR for an OS of 5 years in patients with U2AF1S34 and U2AF1Q157 was 3.68. There were no significant differences in leukemia-free survival or hypomethylating therapy response between patients with and without U2AF1 mutations.
Conclusion
U2AF1 mutations were associated with poor survival in MDS patients, and patients with U2AF1Q157 had a worse OS than those with U2AF1S34. Our findings suggest that MDS patients with U2AF1 mutations could benefit more from hypomethylation therapy.
Introduction
Myelodysplastic syndromes (MDS) are a group of clonal hematopoietic diseases characterized by ineffective hematopoiesis leading to peripheral blood cytopenias, and are likely to evolve into acute myelogenous leukemia (AML).1–3 The prognosis of MDS is very diverse because of the background of their genetic heterogeneity. Common karyotypic abnormalities have been included in the Revised International Prognostic Scoring System (IPSS-R), 4 and the development of next-generation sequencing (NGS) has revealed that approximately 90% of MDS patients have a somatic mutation in at least one driver gene. 5 The number of these driver genes is large, but they can be organized into a limited number of categories such as RNA splicing genes, epigenetic regulators, transcription factors, cohesin components, DNA damage response, and signal transduction molecules. 6 Some somatic mutations, such as those in TP53, EZH2, ETV6, RUNX1, and ASXL1, were demonstrated to be associated with poor outcome, and only the SF3B1 mutation was reported to be associated with a more favorable prognosis. 7 However, the prognostic values of many mutations remain to be confirmed.
U2 small nuclear RNA auxiliary factor 1 (U2AF1) is a member of the SR protein family and a subunit of the U2 small nuclear ribonucleoprotein responsible for recognition of the AG dinucleotide in 30 pre-mRNA splice sites. A total of 5% to 12% patients with MDS carry U2AF1 mutations,8–10 and these almost exclusively affect one of two codons, S34 and Q157, which are located in separate conserved zinc finger domains. U2AF1 mutations can lead to variable post-transcriptional splicing of genomes, including exons and introns that cannot be spliced, 11 which results in the downregulation of many genes. 8 U2AF1 mutations were also reported to be an early, initiating genetic event in MDS. 12 Previous research found that U2AF1 mutations are closely related to sole trisomy 8 and isolated del(20q).13,14 Trisomy 8 was reported not to influence the outcome of MDS patients, while isolated del(20q) is a good factor for prognosis. Some studies showed that U2AF1 mutations had no impact on the outcomes of MDS patients,13,15,16 while others revealed them to be negative factors in MDS prognosis.17–20
Hypomethylating agents such as azacytidine and decitabine have been shown by randomized phase III trials to decrease the risk of leukemic transformation and, in a portion of patients, to improve survival. 7 Thus, hypomethylating therapy (HTM) is considered a conventional treatment for MDS patients, and U2AF1 mutations have been reported to affect the response to HTM.13,17 Therefore, this meta-analysis was conducted to gain a full insight into the prognostic value of U2AF1 mutations in patients with MDS.
Materials and methods
Study selection
A systematic literature search of Chinese Biological Medical Disc, PubMed, Embase, and the Cochrane library databases was performed by two independent reviewers (B.L. and D.Z.). Relevant papers published between 2013 and 2019 were obtained using the search terms ((MDS) OR (myelodysplastic syndrome) OR (myelodysplasia) OR (preleukemia) AND ((U2AF1) OR (U2 Auxiliary factor 1)) in PubMed and the Cochrane library, and (myelodysplastic AND syndrome OR MDS OR myelodysplasia OR ‘preleukemia':af) AND u2af1 AND [2013-2019]/py in Embase. Independent search terms were used to search the Chinese Biological Medical Disc database. The search was restricted to human studies with no language limitation. References were also reviewed to obtain missing information.
Both prospective and retrospective research literature was included in the meta-analysis. Inclusion criteria were as follows: (1) published between 2013 and 2019 as original articles; (2) assessed the association between U2AF1 mutations and outcomes in MDS; and (3) provided detailed survival information of patients with U2AF1 mutations, including the number of surviving patients every year after diagnosis or a clear survival curve or corresponding hazard rations (HRs), 95% confidence intervals (CIs) and P-values. Overall survival (OS) was defined as the length of time from the date of the first sample to the time of death or the last visit. Leukemia-free survival (LFS) was calculated from the date of the first sample to the AML diagnostic time.
Five hundred and ninety-seven studies were identified by the search strategy. By screening titles and reviewing abstracts, animal studies, reviews, case reports, letters to the editor, duplicate publications, and other articles which did not meet the selection criteria were excluded. After this, 62 articles underwent a further screening process which is outlined in Figure 1. Finally, 13 studies were included in the meta-analysis.13,15–21
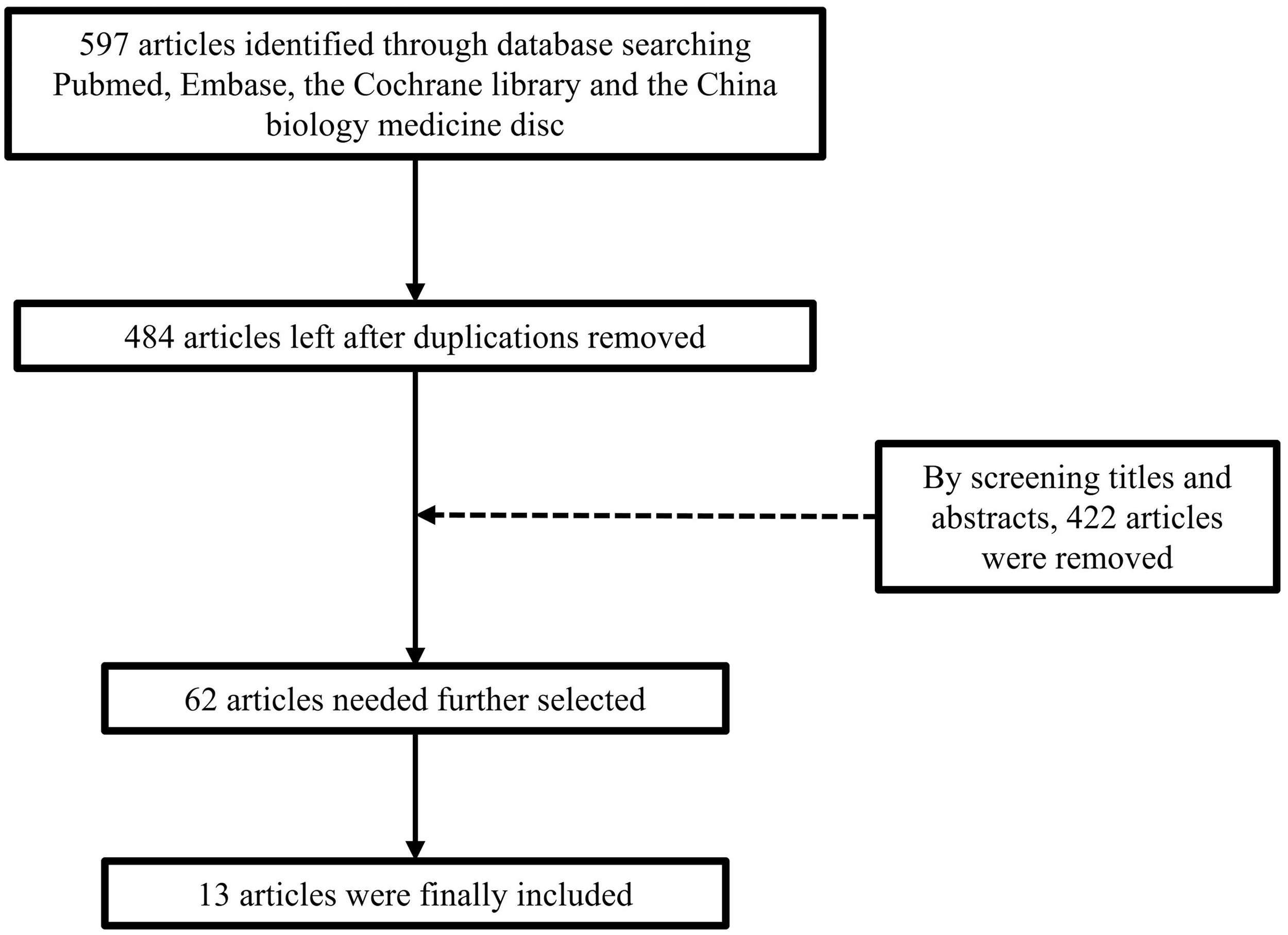
Flow diagram of selection process in the meta-analysis.
Data extraction
To reduce bias, two reviewers (B.L. and D.Z.) independently extracted the following information from the included studies (Table 1): first author’s name, year of publication, journal, region, total number of patients, number of U2AF1 mutations, age and sex distribution of patients, criteria for classification of MDS and karyotypes, and IPSS-R classification. HRs and 95% CIs for OS and LFS were also extracted from the included studies together with the number of patients which survived every year after diagnosis. If the article provided a survival curve, Engauge Digitizer software (Github) 22 was used to extract the number of surviving patients every year after diagnosis. Efforts were made to contact corresponding authors for missing data.
Summary of the data extracted from the 13 included studies.

Abbreviations: WHO, World Health Organization; FAB, French–American–British; U2AF1, U2 small nuclear RNA auxiliary factor 1; NR, Not Reported; IPSS-R, International Prognostic Scoring System.
Quality assessment
The quality of the included literature was evaluated by Newcastle–Ottawa quality assessment (NOS). This included 10 items categorized into three major categories: four items for selection, four items for outcome, and two items for comparability, with a total score of 10 (Table 2). We considered a final score of 6 or more as representing a high quality study, and the quality of each included study was high enough for meta-analysis.
Total NOS score of each study.

Note: studies scored a maximum of one star (*) for meeting each criterion, except comparability (design or analysis) scored a maximum of two stars (**).
NOS, Newcastle–Ottawa quality assessment.
Statistical analysis
All statistical analyses were performed using Reviewer Manager Ver5.3 software (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). For studies that provided a survival curve, ORs and 95% CIs of OS and LFS were used to assess the prognostic effect of U2AF1 mutations in MDS patients compared with wild-type. For the studies that provided HRs and 95% CIs for OS, we used the O-E and Variance model to perform the meta-analysis. We also performed an OS comparison between U2AF1S34F and U2AF1Q157. The statistical heterogeneity of the effect was assessed by I2 and Q statistics. Data were calculated using fixed effects models when the P-value of Q statistics was more than 0.05. Otherwise, the random effects model was used. A two-tailed P-value of less than 0.05 was defined as statistically significant. All statistical analyses were performed by B.L. and D.Z. Bubble diagrams were made by R studio, using ggplot2 package.
Results
Characteristics of the selected studies
As shown in Figure 1, 13 studies covering a total of 3038 patients were included in the present meta-analysis. Characteristics of these studies are shown in Table 1. One study included patients from Germany, three studies included patients from America, four were from China, and five were from Korea. Among the 3038 patients, 355 carried U2AF1 mutations. Patient ages ranged from 52 to 74 years. Nine studies reported the karyotype of patients, and nine reported the IPSS-R score which was defined as five grades (very low, low, intermediate, high, and very high). The NOS score is shown in Table 2.
Outcome of the meta-analysis
Significantly more males carried U2AF1 mutations than had the wild-type gene (79.6% vs 60.8%, P < 0.001). Moreover, of those patients with U2AF1 mutations, there were significantly more males than females (15.8% vs. 7.0%, P < 0.001). Abnormal karyotypes were encountered significantly more often in patients with than without U2AF1 mutations (49.6% vs. 37.8%, P < 0.05); similarly, patients with abnormal karyotypes were significantly more likely to have U2AF1 mutations (19.3% vs 12.1%, P < 0.05) (Figure 2).
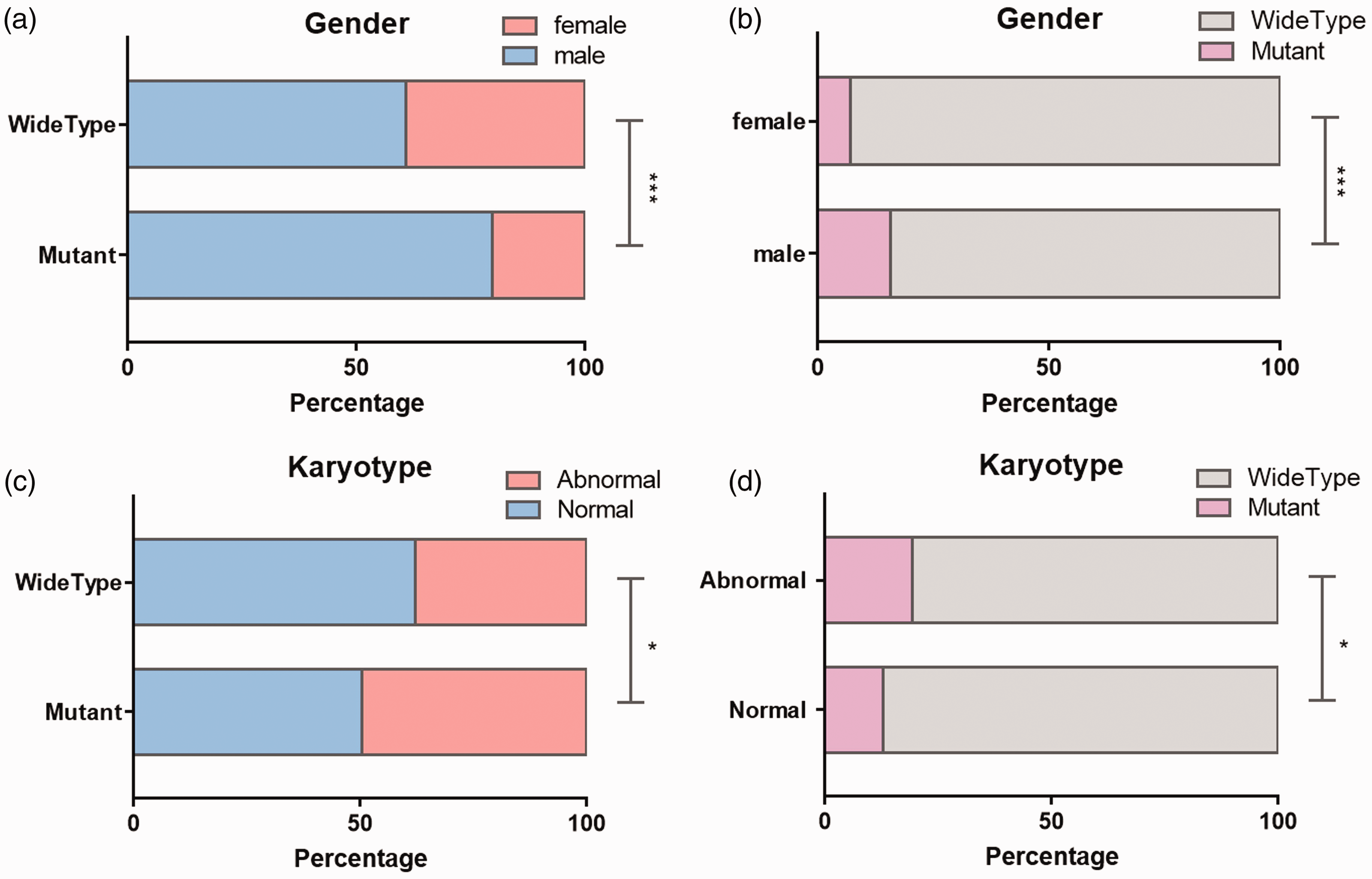
(a) Ratio of males and females for mutant and wild-type U2AF1. (b) Ratio of U2AF1 mutation/wild-type in male and female patients. (c) Ratio of normal and abnormal karyotypes in mutant and wild-type U2AF1. (d) Ratio of U2AF1 mutations in patients with normal and abnormal karyotypes. *: P< 0.05, ***: P < 0.001.
As shown in Figure 3a–d, we analyzed the ORs of OS in MDS patients with U2AF1 mutations in eight studies;13,15–21 summary ORs for OS of 1, 2, 3, and 5 years were 0.76 (95% CI: 0.54–1.09), 0.47 (95% CI: 0.35–0.62, P < 0.001), 0.43 (95% CI: 0.24–0.78, P = 0.006), and 0.37 (95% CI: 0.26–0.51, P < 0.001), respectively. In the case of 3-year OS, high heterogeneity was observed with an I2 of 64% (P = 0.006). As shown in Figure 3e, the summary HR of OS in MDS patients with U2AF1 mutations from 10 studies13,15,16,18,20,23–27 was 1.60 (95% CI:1.33–1.92, P <0.001); this demonstrated that U2AF1 mutations were a poor factor for longer-term survival in MDS patients. The tendency for OS in patients with and without U2AF1 mutations is shown in Figure 3f for each study. Because of a lack of information, LFS data were only collected from three studies 13,17,18. No differences in LFS were identified between patients with and without U2AF1 mutations (Figure 4).

Summary odds ratios (ORs) for overall survival (OS) at 1, 2, 3, and 5 years in MDS patients with and without U2AF1 mutations. (a) 1 year OS. (b) 2 year OS. (c) 3 year OS. (d) 5 year OS. (e) Summary hazard ratios (HRs) for OS. (f) OS tendency in patients with and without U2AF1 mutations; green plots represent those without U2AF1 mutations. The size of each point represents the weight of each study in the meta-analysis.
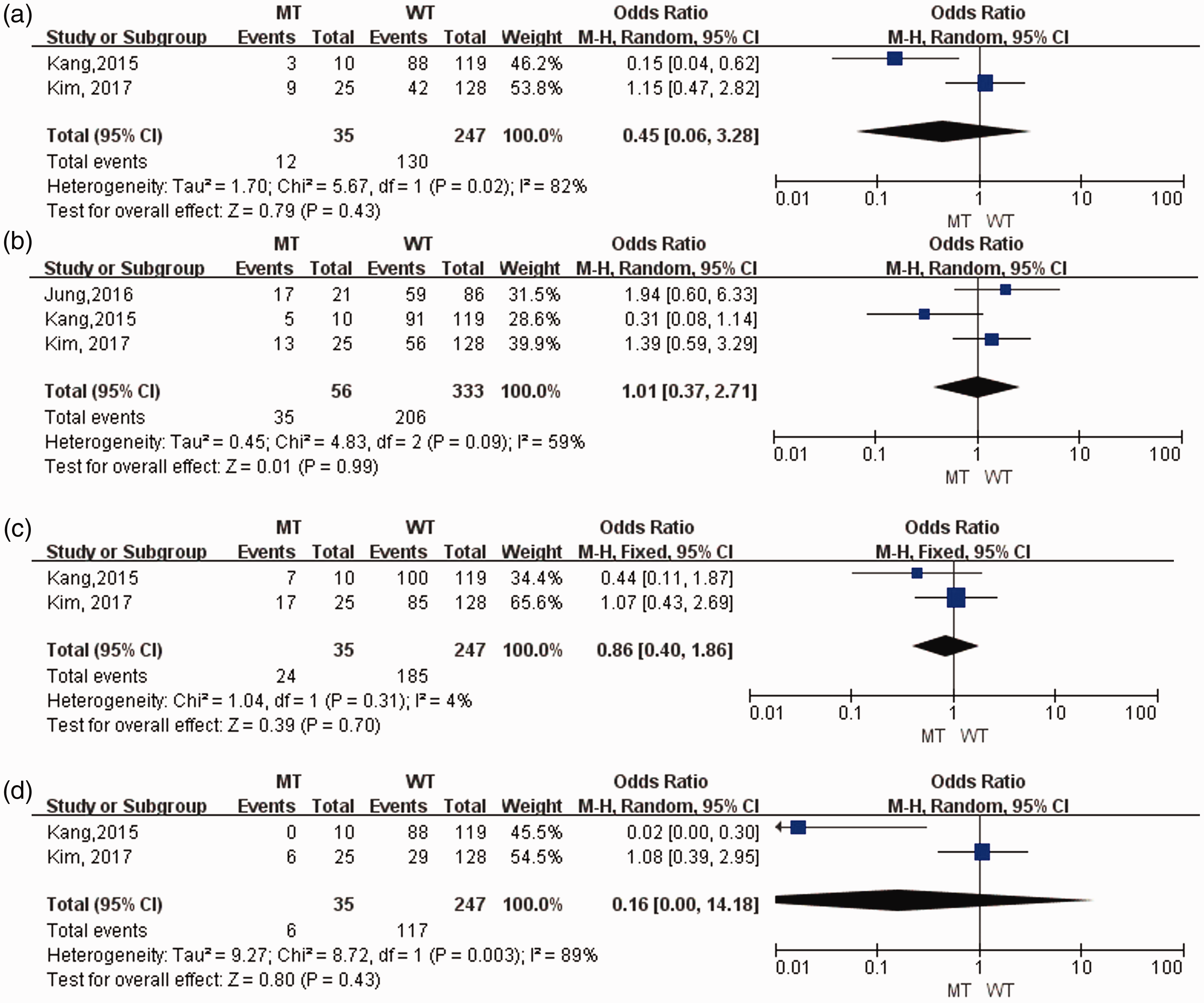
Summary ORs for leukemia-free survival (LFS) at 1, 2, 3, and 5 years in MDS patients with and without U2AF1 mutations. (a) 1 year LFS. (b) 2 year LFS. (c) 3 year LFS. (d) 5 year LFS.
In MDS, U2AF1 mutations predominantly affect S34 and Q157 codons, so these were further analyzed in the meta-analysis. Figure 5a–d shows that summary ORs for OS in patients with U2AF1S34 and U2AF1Q157 of 1, 2, 3, and 5 years were 0.92 (95% CI: 0.30–7.52), 1.53 (95% CI: 0.68–3.48), 1.56 (95% CI: 0.65–3.76), and 3.68 (95% CI: 1.32–10.25, P = 0.01), respectively, indicating that patients with U2AF1Q157 had a worse prognosis than those with U2AF1S34 for long-term survival. This tendency is also shown in Figure 5e. Our findings also revealed an OR for HTR between patients with and without U2AF1 mutations of 0.76 (95% CI: 0.24–2.44), demonstrating that the U2AF1 mutation status does not affect HTR (Figure 6).

Summary OR of OS in MDS patients with U2AF1S34 and U2AF1Q157. (a) 1 year OS. (b) 2 year OS. (c) 3 year OS. (d) 5 year OS. (e) OS tendency in patients with U2AF1S34 and U2AF1Q157.

Summary OR for hypomethylating therapy response (HTR) in MDS patients with and without U2AF1 mutations.
Discussion
Recently, with the development of next-generation sequencing, many more mutations have been identified as being associated with hematological disorders, which may affect disease progression. 28 Patients with U2AF1 mutations were previously shown to have distinct clinical features, including a younger age, isolated +8 or 20q-, and ASXL1 mutations13,14,19. However, the association between U2AF1 mutations and MDS outcomes was controversial.
In our analysis, summary ORs for OS of 2, 3, and 5 years as well as the summary HR in all patients demonstrated significant differences in patients with and without U2AF1 mutations, suggesting that the mutations could have an adverse survival impact. This is despite the association of U2AF1 mutations with improved prognostic factors such as younger age.13,14,19 We also found that patients carrying U2AF1 mutations had a higher risk of abnormal karyotypes, which are indicative of a worse prognosis. Because U2AF1 is a splicing factor, its mutations can cause abnormal splicing and aberrant expression of different genes. Additionally, a previous in vitro experiment showed that U2AF1 mutations affect cell cycle and apoptosis in HeLa cells, 11 indicating that they play an important role in cell proliferation. However, in our meta-analysis, there was no significant difference in LFS between patients with and without U2AF1 mutations although this may reflect the limited number of cases.
U2AF1S34 and U2AF1Q157 have been reported as two major mutation types of U2AF1. 21 The U2AF1S34 mutation tends to splice CAG rather than UAG 3′ splice site sequences, 29 while U2AF1Q157 reinforces the preferential recognition of G instead of A at the +1 position. 30 In our meta-analysis, we compared the prognostic values of the two mutation variants, but only three of the included studies had performed an OS comparison of U2AF1S34 and U2AF1Q157. Nevertheless, we showed that patients with U2AF1Q157 had a worse OS than those with U2AF1S34 after 5 years, suggesting that mechanistic differences occur between U2AF1S34 and U2AF1Q157 that should be further studied.
Hypomethylating therapy such as azacitidine and decitabine is a major breakthrough in the treatment of MDS patients which could improve transfusion requirements and change the natural history of the disease. 31 Therefore, we analyzed the impact of U2AF1 mutations on MDS outcomes under hypomethylating therapy in our meta-analysis. Although there were only two studies reporting the proportion of HTR, we found that the HTR of MDS was independent of the U2AF1 mutation status, indicating that HTR could still improve the prognosis of MDS patients with U2AF1 mutations. Further studies are needed to confirm this conclusion.
In our meta-analysis, the analysis of 3-year OS in all patients presented with a high heterogeneity because of a limited number of cases in the original study. 18 If we removed this study, the P-value of the Q test became 0.06 and I2 became 53%, which we can regard as low heterogeneity. This enabled the analysis to be performed using fixed effects models, which gave an OR of 0.38 (95% CI: 0.22–0.66, P< 0.001). Similarly, the limited information about HTR also may have caused heterogeneity in the corresponding results.
Although this meta-analysis has a number of limitations, it nevertheless demonstrates that U2AF1 mutations have a poor impact on survival in MDS, which to the best of our knowledge has not previously been reported. It is conceivable that a new prognostic scoring system for MDS will be developed to include U2AF1 and other splicing factor gene mutations to replace the traditional risk ones such as IPSS, IPSS-R, and WPSS. However, in the meantime, more research is required to determine the prognostic values of mutations.
Footnotes
Acknowledgement
This research was supported by the Zhejiang Provincial Natural Science Foundation of China under Grant No. LY17H160005, the National Natural Science Foundation of China under Grant No. 81401321, the Traditional Chinese Medicine Administration of Zhejiang Province under Grant No. 2015ZZ018, and the Natural Science Foundation of Ningbo under Grant No. 2014A610217.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.