
Abstract
Splenosis refers to the seeding of splenic cells associated with surgery or trauma. Splenosis mimicking other diseases has been reported in the literature. To the best of our knowledge, this is the first case of follicular lymphoma in a patient with splenosis whose diagnosis of lymphoma was delayed because of a known history of splenosis. We report a 48-year-old male patient who underwent splenectomy because of injury from a high fall 20 years previously. He had no symptoms other than mild abdominal pain until 2 years previously, which was thought to be associated with splenosis. When his symptoms began to increase, he had explorative laparotomy for diagnosis, which was later confirmed as follicular lymphoma. Splenosis may delay the diagnosis of other conditions that can be underestimated. Clinicians should be aware of unusual symptoms in patients with splenosis.
Introduction
Splenosis is defined as transplantation of splenic tissue that usually follows splenic trauma or surgery and often occurs many years previously. These splenic ruptures are generally numerous and vary between millimeters to a few centimeters in size. 1 Although splenosis can be located in the thoracic cavity, it is commonly located anywhere within the abdomen or pelvis. Splenosis is regarded as a benign condition that is usually asymptomatic and requires no treatment unless it causes symptoms. Diagnosis of this condition can be made by tissue biopsy or radiological techniques, such as scintigraphy with Tc-99m or magnetic resonance imaging.1,2 We report the first case of follicular lymphoma in a patient with splenosis.
Case presentation
A 48-year-old male patient with no significant medical history other than radiologically diagnosed splenosis presented with the complaint of slowly increasing abdominal pain. The patient had a history of splenectomy after falling from a tree 20 years ago. His follow-up images showed hypointense, round lesions up to 3 cm in diameter in the left upper quadrant of the abdomen, some of which were localized to the abdominal wall and some were adjacent to the upper pole of the left kidney. This finding was consistent with splenosis when evaluated together with the patient’s anamnesis. After this history of trauma, he only had mild abdominal pain during effort up until the last 2 years. He began to experience occasional abdominal pain, unrelated to food and exertion, in the year before admission. After visiting a doctor, abdominal ultrasonography (USG) was performed and his complaints were thought to be associated with splenosis. In the last 3 months, the complaint of abdominal pain gradually increased and he consulted a doctor again at a hospital. An abdominal USG showed a dense, vascular, 150-mm mass lesion with lobulated contours at the mesenteric root at the level inferior to the pancreas. A computed tomography (CT) scan of the abdomen showed a lobulated contoured mass lesion of 129 × 64 mm in its widest length in part of the left abdomen. Another 23 × 58-mm lobulated contoured lesion was observed at the upper pole of the left kidney (Figure 1). The radiological diagnosis was suggestive of sarcoma. Oncological markers were normal. An upper system gastrointestinal system endoscopy and colonoscopy were performed and showed no pathology. Endoscopic ultrasound of the stomach was performed to obtain a diagnosis, but a lesion was not observed. A Tru-Cut biopsy was not performed from the main lesion because of its close proximity to vascular structures and the patient was offered an exploratory laparotomy. The patient visited our university hospital for a second opinion.
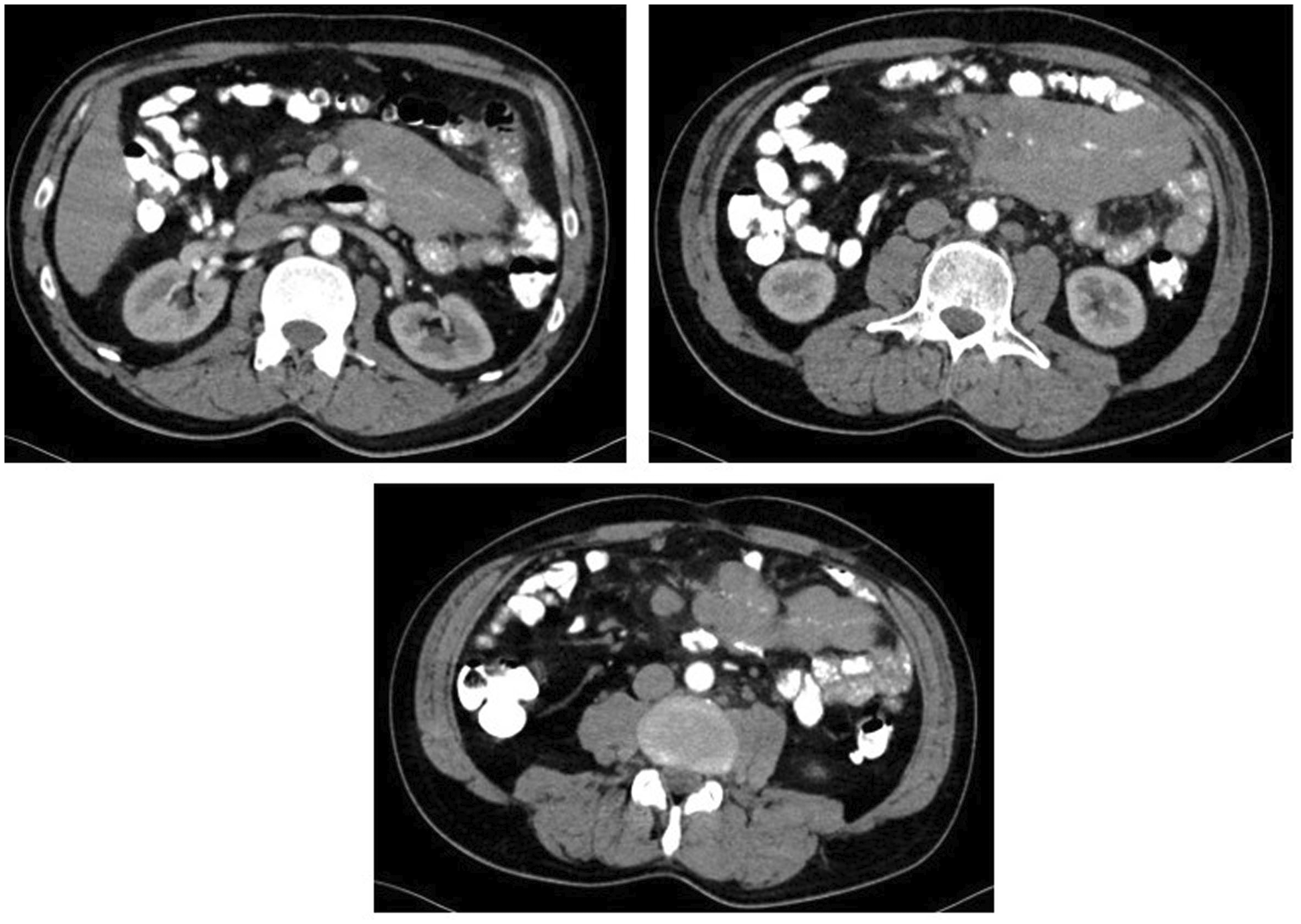
Abdominal and pelvic computed tomography (CT) scans of the patient show a lobulated contoured mass lesion of 129 × 64 mm in its widest length in part of the left abdomen. Another 23 × 58-mm lobulated contoured lesion can be seen at the upper pole of the left kidney.
A mesenteric midline Tru-Cut biopsy was performed and it led to the diagnosis of splenosis and reactive lymph nodes. We decided to perform a positron emission tomography and computed tomography (PET/CT) scan to establish whether there was malignancy and to rule out splenosis. A mass lesion of 55 × 114 mm with intense increased fluorodeoxyglucose (FDG) involvement (maximum standardized uptake value [SUVmax]: 13.8) that was located between the bowel loops in the mesenteric area of the middle left quadrant was observed. Near the mass, nodular lesions were observed in the mesenteric and aortocaval areas with increased FDG uptake (SUVmax: 9.5) (Figure 2). The patient was referred to interventional radiology and multiple Tru-Cut biopsies were obtained from the lesion because of the suspicion of malignancy in PET/CT. In immunohistochemistry, CD3 and CD5 were negative and CD10, CD20, BCL2, and BCL6 were positive in tumor cells. The patient was diagnosed with a low-grade follicular lymphoma. He received six cycles of bendamustine (90 mg/m2/day on days 1 and 2 every 28 days) and rituximab (375 mg/m2 on day 1 every 28 days) chemotherapy, which resulted in a complete response to treatment.

Positron emission tomography and computed tomography scan showing a mass lesion of 55 × 114 mm with intense increased fluorodeoxyglucose involvement (maximum standardized uptake value: 13.8) located between the bowel loops in the mesenteric area of the middle left quadrant. Near the mass, nodular lesions can be seen in the mesenteric and aortocaval areas with increased fluorodeoxyglucose uptake (maximum standardized uptake value: 9.5).
The patient provided written consent for publication. Ethics committee approval was not required for this case report.
Discussion
Buchbinder and Lipkoff first introduced the term splenosis in 1939. 1 Splenic remnants implant on the serosal surface, derive their blood supply from surrounding tissue, and grow into mature splenic tissue that is histologically indistinguishable from the normal spleen. Spleen implants, as in our case, can be multiple with different sizes. 3 Splenosis is found in 26% to 65% of cases following trauma.4,5 Most patients are asymptomatic and splenosis is usually found incidentally in radiological imaging, as in our case.1,3 The diagnosis of splenosis is often made using CT, conventional magnetic resonance imaging, and USG. If a diagnostic dilemma persists after traditional imaging, non-invasive nuclear scintigraphic studies become the imaging modalities of choice. 6
Splenosis should be considered in the differential diagnosis of benign and malignant abdominal conditions.1,6 Splenosis may be confused with primary renal, gastric, or hepatic tumors, metastatic disease, carcinomatosis, peritoneal mesothelioma, endometriosis, or simple adenopathy. 7 Therefore, considering splenosis is important in the differential diagnosis of abdominal masses in splenectomized patients, as well as establishing the correct diagnosis by non-invasive procedures. In our case, the differential diagnosis was sarcoma and lymphoma, which required a tissue biopsy to avoid unnecessary aggressive surgery.
Multiple cases of splenosis mimicking lymphomas have been reported.8,9 However, there have been no reports of follicular lymphoma located only in the abdominal region in a patient with a known history of splenosis. The diagnosis of splenosis in our patient was complicated by the evaluation processes and caused a late diagnosis of follicular lymphoma.
Conclusions
On imaging, splenosis can be confused with multiple entities in differential diagnosis of benign and malignant conditions.1–3 Unless splenosis is symptomatic, it does not require follow-up. However, splenosis should be kept in mind for diagnosis, especially in the presence of atypical symptoms and courses, when other causes need to be searched for with further work-up.
Supplemental Material
IMR890200 Supplemental Material - Supplemental material for Follicular lymphoma in a patient with splenosis: a case report
Supplemental material, IMR890200 Supplemental Material for Follicular lymphoma in a patient with splenosis: a case report by Umut Kefeli, Ozgur Mehtap, Ozgur Cakir, Ahmet Tugrul Eruyar, Serkan İsgoren and Aysegul Ucuncu Kefeli in Journal of International Medical Research
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.