
Abstract
Objective
S100A12 is an emerging inflammatory disease biomarker. Interstitial lung disease (ILD) is a common, severe complication of dermatomyositis (DM). This study was performed to investigate the association between S100A12 and disease activity and prognosis in patients with DM-associated ILD (i.e., DM-ILD).
Methods
Serum S100A12 levels were measured using enzyme-linked immunosorbent assays in patients with stable DM-ILD, patients with acute exacerbation of DM-ILD (AE DM-ILD), and healthy controls (HCs). The relationships of serum S100A12 levels with C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), ferritin, high-resolution computed tomography (HRCT) scores, and pulmonary functions were evaluated by multiple unpaired t-tests and Pearson correlation.
Results
Serum S100A12 levels were higher in patients with stable DM-ILD and those with AE DM-ILD than in HCs. Serum S100A12 levels in patients with stable DM-ILD and those with AE DM-ILD were positively correlated with CRP, ESR, and ferritin. S100A12 levels were positively correlated with HRCT scores in patients with stable DM-ILD and those with AE DM-ILD, while they were negatively correlated with predicted percentages of forced vital capacity and predicted percentages of carbon monoxide diffusing capacity in those patients.
Conclusion
Our findings demonstrate the usefulness of serum S100A12 levels for assessing clinical severity and prognosis of DM-ILD.
Keywords
Introduction
Dermatomyositis (DM) is characterized by skeletal muscle inflammation, which often extends to the skin and lungs. Interstitial lung disease (ILD) is common and presents earlier than myositis in 18% to 20% of patients. 1 Most patients with ILD exhibit chronic disease, but subacute worsening may occur. 2 S100A12 is a member of the S100 family of EF-hand calcium-binding proteins; it is related to the innate immune response and certain autoimmune reactions. Notably, it is involved in a variety of processes (e.g., chemotaxis and intracellular signaling cascade activation) that lead to the production of inflammatory cytokines and induction of oxidative stress. 3 Recent clinical evidence has demonstrated that S100A12 can be overexpressed in inflammatory compartments;4,5 accordingly, elevated serum levels of S100A12 are regarded as an emerging biomarker for acute and chronic lung disorders.6,7 Serum S100A12 levels are reportedly higher in patients with idiopathic pulmonary fibrosis, and are correlated with poor outcomes. 8 However, to the best of our knowledge, S100A12 levels in patients with DM-associated ILD (i.e., DM-ILD) and their prognostic significance in this disease have not been reported. Such data regarding S100A12 may contribute to the establishment of new therapeutic targets. The objective of this study was to investigate the relationships of S100A12 levels with disease activity and prognosis in patients with DM-ILD.
Methods
Ethical approval
The study protocol was approved by the Institutional Review Board of Renji Hospital (Approval No. 2016075). Informed consent was obtained from all participants.
Patients
The current study included patients who were newly diagnosed with definite DM-ILD in Ren Ji Hospital South Campus from September 2017 to October 2018. Our study population consisted of patients who met the traditional criteria of Bohan and Peter;9,10 they were diagnosed with ILD based on high-resolution computed tomography (HRCT) findings: reticulonodular appearance; ground-glass attenuation or opacities; consolidations; irregular lines; and honeycombing or traction bronchiectasis. Pulmonary function test parameters were recorded, including predicted percentage of forced vital capacity (FVC%) and predicted percentage of carbon monoxide diffusing capacity (DLCO%). Healthy controls (HCs; n = 20) were recruited at Ren Ji Hospital South Campus; they were healthy people without any disease, especially without any autoimmune disease.
For the diagnosis of acute ILD, the following criteria for acute exacerbation of idiopathic pulmonary fibrosis were used: 11 (1) subjective worsening of dyspnea within the past 1 month; (2) appearance of new ground-glass opacities or consolidation on chest radiograph or HRCT; (3) evidence of hypoxemia, as defined by worsened or severely impaired gas exchange; (4) no evidence of infection, as indicated by negative respiratory culture and serologic test results for respiratory pathogens; and (5) no clinical evidence of pulmonary embolism, congestive heart failure, or pneumothorax as a cause of acute worsening.
Disease assessments
HRCT examinations of all patients were performed on the day of hospitalization and within 5 days (median, 3 days; range, 0–5 days) after the onset of symptoms. HRCT was performed to assess the progression of ILD before initiation of treatment. The overall HRCT score was calculated based on the classification system described by Ichikado et al. 12 Pulmonary function tests (i.e., assessments of predicted FVC% and predicted DLCO%) were performed on a JAEGER platform (CareFusion; BD Biosciences, San Jose, CA, USA) before treatment. Routine laboratory tests were performed within 24 hours after admission, and the following data were recorded for this study: C-reactive protein (CRP) level, erythrocyte sedimentation rate (ESR), and ferritin level. Serum S100A12 levels were measured using an enzyme-linked immunosorbent assay (Cusabio Technology LLC, Wuhan, China).
Statistical analysis
Descriptive data are expressed as mean ± SD. Differences between patients and controls were compared using multiple unpaired t-tests. Relationships between two continuous variables were analyzed by Pearson correlation. All statistical analyses were performed using SPSS 23.0 for Windows (IBM Corp., Armonk, NY, USA) and GraphPad Prism 6.0 (GraphPad Software Inc., La Jolla, CA, USA). P < 0.05 was considered statistically significant in all comparisons.
Results
Baseline characteristics of patients and HCs
Thirty-eight patients were included in this study. Table 1 summarizes the characteristics of the three cohorts: patients with stable DM-ILD, patients with acute exacerbation of DM-ILD (AE DM-ILD), and HCs. Notably, HCs did not significantly differ from the two patient cohorts in terms of age or sex.
Clinical characteristics of patients with dermatomyositis associated with interstitial lung disease and healthy controls.
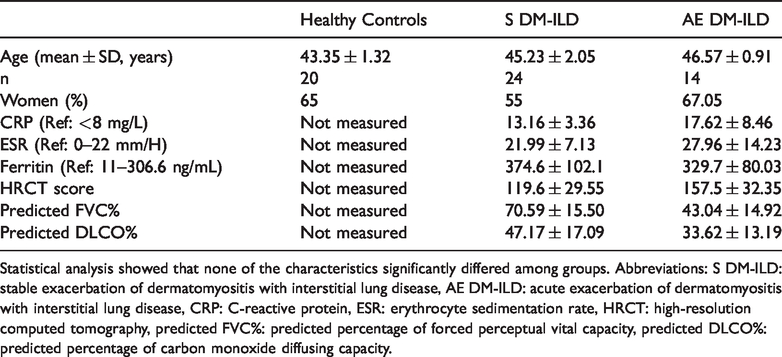
Statistical analysis showed that none of the characteristics significantly differed among groups. Abbreviations: S DM-ILD: stable exacerbation of dermatomyositis with interstitial lung disease, AE DM-ILD: acute exacerbation of dermatomyositis with interstitial lung disease, CRP: C-reactive protein, ESR: erythrocyte sedimentation rate, HRCT: high-resolution computed tomography, predicted FVC%: predicted percentage of forced perceptual vital capacity, predicted DLCO%: predicted percentage of carbon monoxide diffusing capacity.
Serum S100A12 levels were increased in patients with DM-ILD
S100A12 levels were higher in patients with stable DM-ILD and those with AE DM-ILD than in HCs (18.33 ± 1.01 ng/mL vs 25.52 ± 1.17 ng/mL, P < 0.01 and 18.33 ±1.01 ng/mL vs 32.25 ± 1.40 ng/mL, P < 0.001, respectively). Moreover, S100A12 levels were higher in patients with AE DM-ILD than in patients with stable DM-ILD (25.52 ± 1.17 ng/mL vs 32.25 ± 1.40 ng/mL, P < 0.001) (Figure 1a). Consistent with these findings, receiver operating characteristic analyses revealed that serum S100A12 levels exhibited good predictive performance for severity of DM-ILD (Figure 1b).

(a) Comparison of S100A12 among patients with S DM-ILD, patients with AE DM-ILD, and healthy controls. ***P<0.001. (b) Receiver operating characteristic curve for prediction of dermatomyositis associated with interstitial lung disease, with corresponding area under the curve values. Abbreviations: S DM-ILD: stable exacerbation of dermatomyositis with interstitial lung disease, AE DM-ILD: acute exacerbation of dermatomyositis with interstitial lung disease.
Serum S100A12 levels were associated with disease activity in patients with DM-ILD
As shown in Figure 2a–c, serum S100A12 levels were positively correlated with CRP, ESR, and ferritin in patients with stable DM-ILD and in those with AE DM-ILD.

Serum S100A12 levels were associated with clinical characteristics in patients with dermatomyositis associated with interstitial lung disease. Serum S100A12 levels were measured in patients with S DM-ILD and patients with AE DM-ILD; these levels were correlated with (a) CRP, (b) ESR, and (c) ferritin. Abbreviations: S DM-ILD: stable exacerbation of dermatomyositis with interstitial lung disease, AE DM-ILD: acute exacerbation of dermatomyositis with interstitial lung disease, CRP: C-reactive protein; ESR: erythrocyte sedimentation rate.
Relationships of serum S100A12 levels with lung structural changes and pulmonary function impairments in patients with DM-ILD
Serum S100A12 levels were positively correlated with lung structural changes in patients with ILD, as determined by HRCT scores in patients with stable DM-ILD and those with AE DM-ILD (Figure 3a). Furthermore, in patients with stable DM-ILD and those with AE DM-ILD, serum S100A12 levels were negatively correlated with pulmonary function impairment, as indicated by predicted FVC% and predicted DLCO% (Figure 3b, c).

Serum S100A12 levels were associated with lung structural changes and pulmonary function impairments in patients with dermatomyositis associated with interstitial lung disease. Serum S100A12 levels were measured in patients with S DM-ILD and patients with AE DM-ILD; these levels were correlated with (a) pulmonary HRCT score, (b) predicted FVC%, and (c) predicted DLCO%. Abbreviations: S DM-ILD: stable exacerbation of dermatomyositis with interstitial lung disease, AE DM-ILD: acute exacerbation of dermatomyositis with interstitial lung disease, HRCT: high-resolution computed tomography, predicted FVC%: predicted percentage of forced perceptual vital capacity, predicted DLCO% predicted percentage of carbon monoxide diffusing capacity.
Discussion
In this study, we investigated the clinical utility of serum S100A12 levels in patients with DM-ILD. We found that serum S100A12 levels were elevated in patients with DM-ILD; moreover, these levels were associated with the clinical characteristics of disease and may be correlated with the prognosis of DM-ILD.
The S100 family represents the largest subgroup within the Ca2+-binding EF-hand protein superfamily. Serum S100 protein levels are related to disease activity in inflammatory processes. S100 proteins may participate in the pathogenesis of some autoinflammatory diseases, such as familial Mediterranean fever or systemic juvenile idiopathic arthritis. 13 S100A12 is a member of the S100 family of calcium-binding proteins; notably, its levels increase with inflammation. 14 DM is an idiopathic inflammatory myopathy that often involves inflammation of the skeletal muscles and skin. 15 In patients with DM,ILD is an important prognostic factor, which causes higher morbidity and mortality.16,17 On the basis of this association, we presumed that S100A12 levels might be elevated in patients with DM-ILD and may be related to disease activity and prognosis. Accordingly, we measured serum CRP, ESR, and ferritin levels. We found that serum S100A12 levels were higher in patients with DM-ILD than in HCs; the good predictive capacity and specificity of S100A12 suggests it can be used as a biomarker for DM-ILD and may act as a pathogenic driver in patients with DM-ILD. We also found that elevated S100A12 levels were positively correlated with levels of CRP, ESR, and ferritin. Therefore, we speculate that S100A12 might contribute to inflammation in patients with DM-ILD.
HRCT findings are crucial in the diagnosis of ILD, in that they play important roles in judgment of prognosis and treatment strategies. 18 The HRCT score system provides a quantitative approach for assessment of HRCT findings. In patients with idiopathic pulmonary fibrosis, predicted FVC% and predicted DLCO% are the most sensitive parameters for assessment of the clinical course of disease. 19 In this study, we found that serum S100A12 levels were positively correlated with ILD structural damage (HRCT score) and negatively correlated with pulmonary function impairment (predicted FVC% and predicted DLCO%). Thus far, many studies have shown correlations between serum S100A12 and the prognoses of some inflammatory diseases, as well as between serum S100A12 and the activity of these diseases.20,21 The findings of the present study suggest that S100A12 levels are correlated with the prognosis and severity of DM-ILD.
In brief, we found that serum S100A12 levels were elevated in patients with DM-ILD; moreover, these levels were correlated with clinical severity, HRCT scores, and pulmonary function impairment (predicted FVC% and predicted DLCO%) in affected patients. Hence, serum S100A12 levels may be used to assess disease characteristics and prognosis in patients with DM-ILD, improving disease management.