
Abstract
Objective
Endothelin-1 (ET-1) promotes the progression and induction of sclerotic renal changes in end-stage kidney disease. Membrane-bound endothelin-converting enzyme 1 (ECE-1) is involved in the production of ET-1. The aim of this study was to assess the effects of ECE-1b rs213045 and rs2038089 polymorphisms, which have been shown to be involved in the development of atherosclerosis, hypertension, and nephropathy, on the development of contrast-induced acute kidney injury (CI-AKI) in patients with acute coronary syndrome.
Methods
Our study included 38 patients with CI-AKI (CI-AKI[+]) and 55 patients without CI-AKI (CI-AKI[−]) who had coronary syndrome. The ECE-1b polymorphisms rs213045 and rs2038089 were assessed using real-time PCR. Serum ET-1 levels were measured by ELISA.
Results
The distributions of ECE-1b rs213045 and rs2038089 polymorphisms were similar between the two groups. Additionally, the serum ET-1 level did not different between the groups and was not associated with the ECE-1b polymorphisms. Peri-procedural low systolic blood pressure (SBP) was identified as a risk factor for CI-AKI development.
Conclusion
Our findings indicate that ECE-1b rs213045 and rs2038089 polymorphisms are not associated with CI-AKI development and that peri-procedural low SBP is a risk factor for CI-AKI. However, variations in ECE-1b rs2038089 may contribute to the development of CI-AKI.
Keywords
Introduction
The incidence of contrast-induced acute kidney injury (CI-AKI) has been reported to be three times greater in patients with acute coronary syndrome than in patients with stable angina pectoris undergoing coronary angiography. 1 The development of CI-AKI may differ because of potential differences in genetic and physiological susceptibilities between these patient groups.
Recent studies have reported that endothelin-1 (ET-1) is upregulated in cardiovascular and renal diseases and that it plays an important role in renal damage in the course of cardiovascular disease.2,3 However, the cellular and molecular mechanisms by which ET-1 plays a role in renal injury are not fully understood. One proposed mechanism is that ET-1 promotes the progression and induction of sclerotic renal changes in end-stage kidney disease.
Polymorphisms in the endothelin gene family have been shown to be associated with the development of atherosclerosis, hypertension, and nephropathy.4–7 Membrane-bound endothelin converting enzyme-1 (ECE-1) is involved in the proteolytic process, leading to the formation of active ET-1 from precursor ET-1. Increased ECE-1 expression appears to result in an increase in ET-1 biosynthesis. 8 Numerous polymorphisms of the ECE-1 gene have been identified and their association with cardiovascular disease risk have been investigated. Among these polymorphisms, the most frequently investigated is the C-338A (rs213045) polymorphism, which has been found to be associated with hypertension, coronary artery disease, carotid atherosclerosis, and ischaemic stroke.4,6,9
Polymorphisms of the ECE-1 gene (rs213045 and rs2038089) in the endothelin system have previously been shown to be involved in the development of atherosclerosis, hypertension, and nephropathy; however, the effects of these polymorphisms on the aetiopathogenesis of AKI associated with contrast administration in patients with acute coronary artery syndrome remain unclear.4–7 Therefore, the present study aimed to determine the effects of rs213045 and rs2038089 polymorphisms on CI-AKI development in patients with acute coronary syndrome, who have a three-fold increased incidence of CI-AKI and increased mortality and morbidity.
Material & methods
Patients
Our hospital database was screened for patients with acute coronary syndrome without ST-segment elevation treated between February 2011 and December 2016. Patients were retrospectively identified and invited to a hospital visit for blood sampling for genotype analysis and endothelin level measurement. Patients with CI-AKI within this patient population were identified by creatinine level, and CI-AKI was defined as an increase in creatinine level of ≥0.5 mg/dL and/or ≥25% at 48–72 h after exposure to contrast medium compared with the baseline level. The MEHRAN risk scores of CI-AKI patients were calculated. 1 Blood samples were taken from eligible patients after screening. The first blood sample was taken upon admission to emergency services and further blood samples for measurement of creatinine level were collected daily during hospitalization. All patients were treated with 300 mg clopidogrel, 300 mg aspirin, and 1 mg/kg enoxaparin at admission. Atorvastatin 40 or 80 mg was given after blood sample collection, and angiotensin converting enzyme inhibitors and beta blockers were given where haemodynamically appropriate. Low-osmolar contrast media (iohexol) was used in all patients during coronary angiography. Intravenous hydration therapy (1 mL/kg/h 0.9% NaCl solution) was administered 3–12 h before and 6–24 h after the procedure to prevent CI-AKI in patients with a glomerular filtration rate of 30–60 mL/min/1.73 m2. We used the minimum creatinine value between hospital admission and angiography to define the baseline creatinine level.
Patients with ST-elevation myocardial infarction (STEMI) or high-risk non-STEMI requiring urgent coronary angiography within 2 h, left ventricular dysfunction (ejection fraction [EF] < 45%), acute renal failure or end-stage renal failure requiring dialysis, contrast agent exposure within the previous 2 weeks, and advanced comorbidities were excluded from the study. The study was approved by the local ethics committee of Istanbul University Medical Faculty (protocol no. 83045809/604.01) and written informed consent was obtained from each participant prior to blood sample collection. The biochemical parameters, echocardiography results, reference blood pressure values, and demographic characteristics of patients were analysed using data from our hospital database.
Genotyping
Total DNA was extracted from peripheral blood samples using a commercial DNA isolation kit (Roche Diagnostics, GmbH, Mannheim, Germany). The concentration and purity of DNA samples were assessed using a NanoDrop 2000 spectrophotometer (Thermo Scientific, Wilmington, DE, USA). The rs2038089 and rs213045 polymorphisms of the ECE-1 gene were analysed using a TaqMan® SNP genotyping assay (40×) (Thermo Scientific) and real-time PCR Master Mix (Jena Bioscience, Hamburg, Germany) with a CFX Connect™ real-time PCR instrument (BioRad, Hercules, CA, USA) under the following cycling conditions: 2 min at 50°C (pre-incubation), 2 min at 95°C (activation), 15 seconds at 95°C (denaturation), and 1 min at 60°C (binding/extension/reading) (40 cycles). Genotypes were determined automatically by the device according to the FAM or VIC fluorescence signal, which is associated with allele amplification (GG/GT/TT).
Endothelin-1 measurement
A commercial ELISA kit (Shanghai Yehua Biological Technology, Shanghai, China) was used to determine ET-1 levels in serum samples. Absorbance (OD) measurements were obtained using an ELISA plate reader (Multiskan™ GO Microplate Spectrophotometer; Thermo Scientific) at 450 nm. The levels of standards (ng/L) were calculated automatically, and a linear regression equation was obtained according to the OD values. The serum ET-1 levels (ng/L) were determined according to the OD values of the samples.
Statistical analysis
Statistical analyses were performed using SPSS 21 software ((IBM Corp., Armonk, NY, USA)). Data were tested for normality of distribution using the Kolmogorov–Smirnov test. Categorical data were compared between the study groups using the chi-square test, whereas continuous data were compared using Student’s t-test and the Mann–Whitney U test, depending on the normality distribution of the data. Multivariate regression analysis was performed to identify the predictors/risk factors for CI-AKI. The model included CI-AKI as the dependent variable. Age, peri-procedural systolic blood pressure (SBP), EF, and ECE-1b rs2038089 rare G allele were used as categorical independent variables.
The null hypothesis was that there was no association between rs2038089 and rs213045 SNPs of the ECE-1 gene and CI-AKI. We performed sample size calculation using the “PS Power and Sample Size Calculation” package program, with inputs of p0 (probability of exposure in controls) and p1 (probability of exposure in cases) from the Ensembl genome browser (Human (GRCh38.p13); https://www.ensembl.org/Homo_sapiens/Variation/Population?db=core;r=1:21224464-21225464;v=rs2038089;vdb=variation;vf=20747334). The type I error probability (α) was set to 0.05. We planned to include 100 participants in the study. The statistical significance limit was set at p < 0.05. Odds ratios (ORs) and confidence intervals (CIs) were calculated to estimate the relative risk.
Results
After screening, 38 patients with CI-AKI (CI-AKI[+]) and 55 controls without CI-AKI (CI-AKI[−]) were identified. Our sample size analysis showed that these group sizes were sufficient for the power of the study to reach 0.8 (for rs2038089). The characteristics of patients in the CI-AKI(+) and CI-AKI(−) groups are presented in Table 1. In total, 93 patients (27 [29%] female and 66 [71%] male) were included in the study. All patients received anti-aggregants, anti-coagulants, anti-ischaemic agents, and high-dose statin therapy in accordance with their indications. The mean age and MEHRAN score of the total patient group were 60.16 ± 1.14 years and 4.54 ± 0.32 points, respectively. Among patients with acute coronary syndrome, 61.3% had hypertension and 45.2% had diabetes mellitus (DM).
Clinical, demographic and biochemical parameters of patients and distribution according to CI-AKI group.

Values were derived using an independent-sample t-test. Results are shown as mean ± SD or % (in parentheses). Values of P < 0.05 in bold font indicate statistical significance. CI-AKI, contrast induced acute kidney injury; DM, diabetes mellitus; HT, hypertension; MI, myocardial infarction; CABG, coronary artery bypass grafting; PCI, percutaneous coronary intervention; SBP, systolic blood pressure; DBP, diastolic blood pressure; EF, ejection fraction; Total-C, total cholesterol; LDL-C, LDL cholesterol; HDL-C, HDL cholesterol; TG, triglycerides; Hgb, haemoglobin; WBC, white blood cells.
Although age was significantly higher in the CI-AKI(+) group than in the CI-AKI(−) group (62.97 ± 1.70 vs. 58.22 ± 1.51 years, p = 0.041), blood pressure (systolic: 123.73 ± 8.85 vs. 143.06 ± 4.11 mmHg, p = 0.033; diastolic: 70.33 ± 4.96 vs. 82.20 ±1.91 mmHg, p = 0.014) and EF (53.87 ±1.16% vs. 56.56 ± 0.78%, p = 0.048) were significantly lower in the CI-AKI(+) group than in the CI-AKI(−) group (Table 1). The serum ET-1 level did not differ between the study groups and was not associated with the assessed ECE-1 polymorphisms.
Table 2 shows the genotypes, allele distributions, and Hardy–Weinberg equilibriums (HWEs) of the assessed polymorphisms (rs213045 and rs2038089) in the patient groups. The distributions of the genetic polymorphisms between the CI-AKI(+) and CI-AKI(−) groups were similar. The frequencies of all alleles and genotypes in the study groups were compatible with HWE. The frequencies of ECE-1b rs213045 GG, TT, and GT genotypes were 0.50, 0.105, and 0.395, respectively, in the CI-AKI(+) group and 0.436, 0.091, and 0.473, respectively, in the CI-AKI(−) group. The frequencies of ECE-1b rs2038089 AA, GG, and AG genotypes were 0.289, 0.263, and 0.447, respectively, in the CI-AKI(+) group and 0.455, 0.145, and 0.40, respectively, in the CI-AKI(−) group. Among the allele frequencies, the rs2038089 rare G allele frequency was higher in the CI-AKI(+) group than in the CI-AKI(−) group (71.1% vs. 54.5%); however, the difference was not statistically significant.
Genotype and allele distributions of rs213045 and rs2038089 polymorphisms in CI-AKI(+) and CI-AKI(−) patients.
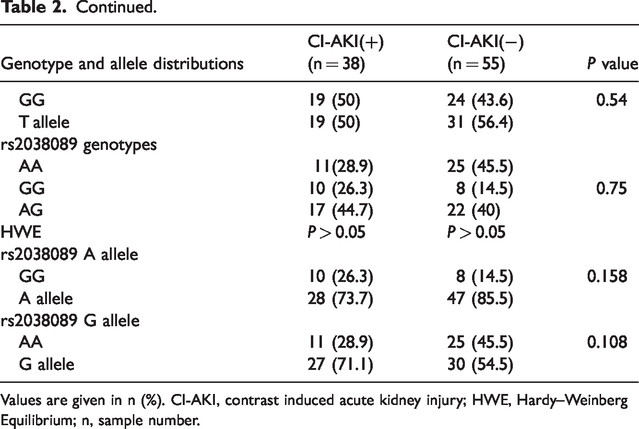
Values are given in n (%). CI-AKI, contrast induced acute kidney injury; HWE, Hardy–Weinberg Equilibrium; n, sample number.
In the multivariate logistic regression analysis, peri-procedural low SBP was identified as a risk factor for CI-AKI development (p = 0.029) (Table 3).
Evaluation of risk factors associated with CI-AKI in multivariate logistic regression analysis.
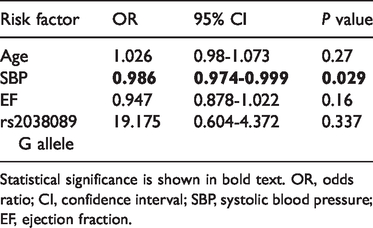
Statistical significance is shown in bold text. OR, odds ratio; CI, confidence interval; SBP, systolic blood pressure; EF, ejection fraction.
Discussion
The risk of CI-AKI is three times greater in patients with acute coronary syndrome than in patients with stable angina pectoris undergoing coronary angiography and/or percutaneous intervention. 10 CI-AKI is the third most common cause of hospital admission for acute renal failure. 11 Therefore, the prevention of CI-AKI in patients at high risk has prognostic significance.
After exposure to contrast medium, deterioration of renal haemodynamics, increase in angiotensin, adenosine, and endothelin secretion, decrease in NO synthesis, oxidative stress, and secretion of proinflammatory cytokines appear to play important roles in interstitial inflammation and tubular necrosis in the kidneys.12,13
Several factors have been identified as determining the risk of CI-AKI prior to coronary angiography/percutaneous procedures. Chronic renal failure, low EF, DM, older age, hypotension, advanced chronic heart failure, and amount of contrast agent used during angiography have been identified as important predisposing factors. Different risk scoring approaches (e.g., MEHRAN score) have been developed based on these factors.1,14 Despite the high sensitivity of risk scoring, CI-AKI can also develop in patients with low risk scores, indicating that some patients might have a genetic predisposition to this condition. Therefore, it is important to identify the genetic biomarkers associated with susceptibility to CI-AKI. Pre-procedural and post-procedural treatment options should therefore be evaluated in individuals with a potential genetic predisposition for developing CI-AKI.
Although multiple studies have examined genetic susceptibility associated with AKI development in recent years, the results are contradictory. Variations in genes that encode proteins associated with inflammation and vasoconstriction have an important relationship to AKI. Some studies found that target gene variations were responsible for an increased risk of AKI,15–19 whereas others found that the variations were not related to the risk of AKI.20–22 ACE I/D and APO-E gene polymorphisms were found to be associated with inflammation and vasoconstriction as well as increased creatinine clearance in a study of genetic polymorphisms affecting AKI development after coronary artery bypass grafting. 16 Additionally, Chew et al. 15 found that APO-E polymorphism was associated with elevated creatinine after cardiac surgery. In contrast, Boehm et al. 21 did not find any significant association between APO-E and TNFα polymorphisms in patients with AKI after cardiac surgery.
Experimental animal studies on receptor responses showed that after the administration of contrast medium in normal rats, a positive effect was observed through mitigation of the ET-A selective blockade of the hypoxic response in the external medulla. Based on these results, it is suggested that oxygen requirements decrease with ET-A antagonism. 22 Other studies have indicated that endothelin might be a contributory factor in CI-AKI development, based on the increase in endothelin levels in plasma and urine observed after contrast medium administration.24–26 Consistent with this hypothesis, individuals with impaired renal function had increased endothelin release after contrast medium administration. It has been reported that the production and release of endothelin from endothelial cells are enhanced after contrast medium administration. 27
Ulaş et al. 28 reported a significant increase in ET-1 levels before and 48 h after contrast administration in 78 patients. In another study investigating the relationship of ET-1 levels with the amount of contrast medium (above or below 150 mL), ET-1 levels were elevated in patients who received more than 150 mL of contrast medium. 29 In addition, polymorphisms in the endothelin gene family have been shown to be associated with chronic renal failure in patients with autosomal dominant polycystic kidney disease and IgA nephropathy.7,29 Although ET-1 is among the candidate genes associated with susceptibility to vascular diseases, an association of ET-1 gene polymorphisms with CI-AKI predisposition has not yet been reported.
Although the ECE-1 gene is important for ET-1 maturation, the relationship between ECE-1 gene polymorphisms and ET-1 levels has not been clarified. Additionally, the effects of ECE-1 gene polymorphisms on contrast nephropathy risk have not been investigated. To our knowledge, our study is the first to investigate a possible relationship between ECE-1 gene polymorphisms and the risk of developing CI-AKI. Moreover, we investigated the relationship between high ET-1 levels suggested in previous studies and CI-AKI development and examined the possible contributions of ECE-1 gene polymorphisms to high ET-1 levels.
In the multivariate logistic regression analysis, peri-procedural low SBP was identified as a predictive factor for CI-AKI. In the scoring system used by Mehran et al., hypotension was identified as a risk factor for CI-AKI development, which supports the finding in our study. Although renal hypoperfusion has been established as having an important role in CI-AKI development, few studies have examined haemodynamic changes such as peri-procedural SBP. In the study by Li et al., 30 which included 349 post-menopausal patients, SBP was lower in patients with CI-AKI, and this decrease was proposed as an independent risk factor for CI-AKI development when it was greater than 10 mmHg.
Multiple studies have shown that hyperglycaemia is associated with the development of CI-AKI. In our study, there was no difference in glucose levels between the CI-AKI groups. This may have been attributable to the fact that the glucose levels were measured after 12 h of fasting and not at the time of admission.
The MEHRAN score was similar between the two groups, and this may be explained by the fact that MEHRAN scoring was developed primarily for stable patients or by the inclusion of a small number of patients in our study.
Our study had several limitations, primarily related to the study design. We screened our hospital database for eligible patients and scheduled blood sample collection among this group; however, not all patients identified in our screening process could be contacted, and this may have led to selection bias. ET-1 levels were measured long after contrast exposure. Therefore, the short-term effect of contrast agent on ET-1 levels could not be demonstrated in our study. Furthermore, we did not enrol patients with STEMI or high-risk acute coronary syndrome so our results cannot be extrapolated to these populations. Finally, data on patient height were unavailable, meaning that we could not determine indexed values or body mass index for our study population.
Conclusion
Our findings indicate that ET-1 levels and ECE-1b rs213045 and rs2038089 polymorphisms are not associated with the development of CI-AKI. A large-scale study is required to clarify the relationship between CI-AKI and the rs2038089 (G allele) polymorphism, and the results of such a study may lead to the prevention of CI-AKI in patients harbouring this genetic variant. Additional studies are needed owing to the lack of a genetic polymorphism related to CI-AKI and the limited number of patients in the present study.