
Abstract
Objective
To investigate maternal and neonatal outcomes after different intrapartum interventions for vaginal birth after cesarean section (VBAC) in mainland China.
Methods
A retrospective study was performed on 143 VBAC cases from Beijing Obstetrics and Gynecology Hospital between January 2015 and November 2016. These cases were divided into two groups on the basis of different intrapartum interventions. Maternal and neonatal outcomes were compared.
Results
The durations of the first stage and total labor after oxytocin were significantly longer than those before oxytocin use. The proportion of operative vaginal delivery with oxytocin was significantly higher than that without oxytocin (43.9% vs. 11.8%). The times of the first stage, second stage, and total labor with analgesia were significantly longer than those without analgesia (548.4±198.1 vs. 341.8±233.0 minutes, 52.0±38.9 vs. 36.0± 29.1 minutes, and 606.3±212.1 vs. 387.3±233.0 minutes, respectively). Postpartum hemorrhage and operative vaginal delivery occurred significantly more frequently in women with epidural analgesia than in those without epidural analgesia (29.7% vs. 12.3 and 35.1% vs. 16.0%, respectively).
Conclusions
Induction can increase the rate of operative vaginal delivery in VBAC. Oxytocin and epidural analgesia may increase the risk of operative vaginal delivery, and may be associated with a prolonged duration of labor.
Keywords
Background
As China modifies its family planning policy to a “universal two-child policy,” many women of childbearing age are having their second child. To date, the rate of cesarean birth for this group ranges from 32.7% to 50.0%.1–4 After a cesarean procedure, the subsequent delivery mode includes repeated cesarean delivery and vaginal birth after caesarean section (VBAC). Because repeated cesarean section may increase postpartum hemorrhage (PPH) and pelvic adhesion, a trial of labor after cesarean (TOLAC) has been found to be the most effective method of delivery. 5 The recent American College of Obstetricians and Gynecologists practice bulletin has revisited VBAC and emphasized the importance of discussing VBAC with all patients who meet the criteria. 6
TOLAC is in its infancy because of the special medical environment in mainland China. However, a growing number of medical institutions are using TOLAC. Exploring labor patterns among these women may be clinically useful for counselling, as well as in guiding clinical management, during the course of labor among women attempting VBAC. With conscientious intrapartum management, there is a high probability of a safe and successful outcome with VBAC. This means that caution is required with induction and augmentation of labor to avoid overstimulation of contractions. Additionally, surveillance regarding signs of uterine rupture is necessary. 7 , 8 Therefore, intrapartum interventions on maternal and neonatal outcomes have attracted the attention of obstetricians. To date, few studies have investigated the outcome of these interventions. 9 , 10
Therefore, we retrospectively assessed VBAC cases in the Department of Perinatal Medicine of Beijing Obstetrics and Gynecology Hospital, Capital Medical University. This study aimed to investigate the effect of different intrapartum interventions on maternal and neonatal outcomes of VBAC in women who had one prior cesarean section in a tertiary hospital in mainland China.
Methods
Ethics statement
This study was approved by the Ethics Committee of Beijing Obstetrics and Gynecology Hospital. All patients were approved for receiving TOLAC by providing written informed consent.
Study design
Inclusion criteria for TOLAC were as follows: healthy pregnant women without contraindications of vaginal delivery, a history of Pfannenstiel incision cesarean, >1 year since the previous cesarean section, no history of uterine rupture, immediate access to emergency surgery, and written informed consent was provided by the patient.
All cases were assessed by a deputy chief physician and the risks for TOLAC were explained to the patients. Induction approaches were selected by determining the cervical Bishop score. If this score was ≥6 points, low-dose oxytocin was used. If the score was <6, mechanical agents (transcervical Foley catheter or double-balloon cervical ripening catheter) were used. All patients with TOLAC were observed in the delivery room and all patients had intravenous access. An initial laboratory evaluation was performed, which included a complete blood count, as well as blood type and screening, to facilitate the rapid availability of blood products, if required.
All patients who underwent TOLAC had continuous electronic fetal monitoring throughout labor. Once arrested labor occurred, fetal distress, abnormal fetal heart rate, suspected uterine rupture, or pregnant women who refused TOLAC were the indications used for immediate emergency cesarean section. Oxytocin was used to strengthen the contractions if necessary. Regional anesthesia was encouraged for patients who underwent TOLAC to provide pain control. Forceps were used for operative vaginal delivery for maternal and fetal indications.
The data of successful VBAC cases were collected from the database, including the interval after the first cesarean section and oxytocin use. The method of delivery, duration of labor, and maternal and neonatal complications, including PPH (defined as total blood loss >500 mL) and fetal distress (umbilical cord blood pH <7.2), were also noted.
Statistical analyses
Comparisons of vaginal delivery, PPH, and fetal distress between different intrapartum interventions were performed using Pearson’s χ2 test and Fisher’s exact test for categorical data, and the Student’s t-test for continuous measures. Adjusted odds ratios with 95% confidence intervals were calculated by modeling the data to control for possible confounding variables. Statistical analysis was performed using SPSS Statistics for Windows, Version 19.0 (IBM Corp., Armonk, NY, USA). A P value <0.05 was considered statistically significant.
Results
A total of 203 women intended TOLAC, among whom 143 (70.4%) had successful VBAC and 60 underwent repeated cesarean section. No maternal or fetal deaths occurred. The reasons for repeated cesarean section were suspected uterine rupture (eight cases, 13.3%), abnormal fetal heart rate pattern (seven cases, 11.7%), stopping TOLAC (30 cases, 50%), and abnormal progression of labor (15 cases, 25%). Furthermore, five (2.46%) patients had uterine rupture during repeated cesarean section.
The baseline characteristics of VBAC cases are shown in Table 1. No deaths occurred. Maternal and neonatal outcomes and intrapartum interventions are summarized in Table 2. For induction of labor, five patients were inducted by mechanical agents, 12 were provided low-dose oxytocin, and three were provided a combination of these two. Oxytocin was used in approximately one third of women to strengthen contractions. The total and mean time of oxytocin use was 0.2 to 11.0 hours and 2.6±2.4 hours, respectively. The rate of oxytocin infusion was 2.70 to 21.12 mU/minute.
Baseline characteristics of patients who had vaginal birth after cesarean section.

Data are mean ± standard deviation or median (range).
Maternal and neonatal outcomes and intrapartum inventions.
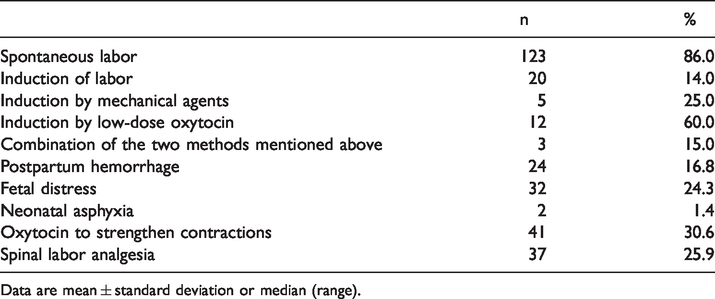
Data are mean ± standard deviation or median (range).
Maternal and neonatal outcomes and initiation of labor.

Data are mean ± standard deviation or number (%). PPH: postpartum hemorrhage; CI: confidence interval.
The patients were divided on the basis of different intrapartum interventions, and maternal and neonatal outcomes were compared between these two groups. The rate of operative vaginal delivery with induction was significantly higher than that with spontaneous labor (P=0.014). The rates of PPH and fetal distress, and the durations of the first stage, second stage, and total labor were similar between the induction group and spontaneous labor group (Table 3). The rate of operative vaginal delivery in induced patients who were treated with oxytocin was significantly higher than that in those without oxytocin (P<0.001) (Table 4). The durations of the first stage, second stage, and total labor with intrapartum oxytocin and analgesia were longer than those without oxytocin and analgesia (all P<0.05 except for the duration of the second stage with intrapartum oxytocin (Tables 4, 5). The incidence of PPH and vaginal delivery in patients who received analgesia was greater than that those who that did not receive analgesia (both P=0.014) (Table 5).
Maternal and neonatal outcome and intrapartum oxytocin.

Data are mean ± standard deviation or number (%). PPH: postpartum hemorrhage; CI: confidence interval.
Analgesia and maternal and neonatal outcomes.

Data are mean ± standard deviation or number (%). PPH: postpartum hemorrhage; CI: confidence interval.
Discussion
Among our patients with VBAC, no deaths occurred. Balachandran et al. 11 described 96 cases of VBAC. Among these cases, four had PPH, five needed operative vaginal delivery, and 33 had fetal distress. In our study, the rates of operative vaginal delivery and PPH were significantly higher than those reported in the literature. 11 However, the rate of fetal distress in our study was significantly less than that previously reported. 11 Furthermore, studies have indicated that the rate of operative vaginal delivery with VBAC was 18.5%, and this is consistent with our data. 12 Abnormal fetal heart rate is the most common clinical manifestation of uterine rupture.13–15 The high rates of operative vaginal delivery and PPH with VBAC may be attributed to emergency delivery situations and an abnormal fetal heart rate. Additionally, there might be more blood loss with VBAC. 16
Induction with low-dose oxytocin and a transcervical Foley catheter or double-balloon cervical ripening catheter was used in this study. In the present study, induction did not increase PPH and fetal distress or prolong labor, but the rate of operative vaginal delivery was higher than that with spontaneous labor. Previous studies have suggested that induction can be used with TOLAC with appropriate communication. 17 Ashwal et al. 18 retrospectively studied 259 cases of induction with TOLAC and found that induction did not increase the risk of uterine rupture or adverse neonatal outcomes compared with the spontaneous labor group. Furthermore, operative vaginal delivery between each group was similar. As mentioned above, the rate of operative vaginal delivery with induction was higher than that with spontaneous labor group in our study. This finding was the result of more awareness of uterine rupture, and because forceps or a vacuum extractor were frequently used to shorten labor during the second stage of labor. Some studies have indicated that induction of labor increases the incidence of uterine rupture, especially with the use of a prostaglandin. 19 However, the relationship of induction and uterine rupture was not studied. Therefore, pregnant women who attempt TOLAC should be advised to wait for spontaneous onset of labor, and whether induction of labor is necessary should be determined. Low-dose oxytocin or physical methods, such as the use of a transcervical Foley catheter or double-balloon cervical ripening catheter, can be applied with informed consent.20–21
In the present study, 2.70 to 21.12 mU/minute of oxytocin was used to strengthen uterine contractions. This procedure increased the duration compared with those who were not provided oxytocin. Additionally, surgical interventions were required to prevent uterine rupture when the cervix was fully dilated. Oxytocin can also be used for TOLAC in pregnant women, but this may increase the risk of uterine rupture, and is dose-dependent. 22 Previous studies have indicated that oxytocin exceeding 20 mU/minute increases the risk of uterine rupture by four fold or greater (21–30 mU/minute: hazard ratio 3.92, 95% confidence interval 1.06–14.52; 31–40 mU/minute: hazard ratio 4.57, 95% confidence interval 1.00–20.82). These findings support the maximal oxytocin dose of 20 mU/minute in VBAC trials, avoiding the unacceptable high risk of uterine rupture. 23 Therefore, low-dose oxytocin was selected for the present study, and contractions were closely monitored.
In our study, analgesia significantly prolonged labor and increased the risk of PPH, but this did not modify the delivery approach or the incidence of fetal distress. Whether analgesia affects the duration of the first stage of labor remains to be determined, and data in the literature are presently inconsistent.24–26 Many factors may influence uterine activity during the first stage of labor, including pain and analgesia, because catecholamines affect uterine contractility. Labor pain causes sympathetic hyperactivity, and increases plasma epinephrine and norepinephrine levels. 27 Epinephrine decreases uterine contractility, while norepinephrine increases uterine contractility. Severe pain, such as that with induced labor, may cause a surge in epinephrine that cannot be offset by an equal increase in norepinephrine, and may precipitate uncoordinated uterine contractions and dystocia. Subsequently, the risk of PPH increases with prolonged labor, and epidural analgesia may be used for TOLAC. Because no data suggest that epidural analgesia causes unsuccessful TOLAC, adequate pain relief may encourage more women to choose TOLAC. Additionally, effective regional analgesia is not expected to mask the signs and symptoms of uterine rupture, particularly because the most common signs of rupture are fetal heart tracing abnormalities. 6 , 8 , 28
Our study is limited because of its single-center design, and randomization was not possible. Additionally, the sample used for the study was small and the study was retrospective in nature. Multicenter, large-sample, randomized trials are required to validate the effect of intrapartum interventions and VBAC. We conclude that pregnant women with one previous cesarean section can undergo VBAC with appropriate care. With the lack of spontaneous onset of labor, low-dose oxytocin and mechanical agents may be useful for induction because oxytocin can be used to strengthen contractions, and epidural analgesia can be used to relieve pain.
Conclusions
Induction increases the rate of operative vaginal delivery in VBAC. Oxytocin and epidural analgesia may increase the risk of operative vaginal delivery, and may be associated with a prolonged duration of labor.
List of abbreviations
VBAC: vaginal birth after cesarean section; TOLAC: trial of labor after cesarean section, PPH: postpartum hemorrhage
Footnotes
Acknowledgements
The authors thank LetPub Company for editing the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This project was supported by the Natural Science Foundation of China (81402689) and Beijing Municipal Science & Technology Commission (Z151100004015182).