
Abstract
Objective
To assess the rural–urban disparity in caesarean section rates using electronic health records from hospitals located in the Province of Inner Mongolia, which is a minority area in Northeastern China.
Methods
The study examined the electronic health records of women that gave birth in three major public hospitals between January 2012 and December 2016. Multinomial regression analyses were used to estimate rural–urban disparities in caesarean section rates.
Results
Data from 61 903 women were examined. Caesarean section rates increased slightly over the study period and the rate was significantly higher in rural compared with urban hospitals (48% versus 38%). This disparity consistently increased over time. Multinomial regression analyses showed that maternal age, ethnicity, health insurance type, employment status, reproductive history and the newborn’s sex were significant risk factors associated with caesarean section rate. Furthermore, stratified analysis of first-time pregnancies, minorities and different age groups showed that the odds of undergoing an emergency caesarean section was lower in the rural hospital, but the odds of undergoing a planned caesarean section was higher in the rural hospital.
Conclusions
Caesarean section rates have increased in rural areas and the disparity in rural–urban areas has increased substantially over the years.
Introduction
A caesarean section refers to the surgical procedure for delivering one or more babies from the mother’s uterus. Various rates of caesarean delivery have been recorded worldwide, and as of 2015, these rates ranged from 26% in New Zealand to 56% in the Dominican Republic. 1 These rates are far higher than the 10%–15% recommended by the World Health Organization in 1985. 2 Caesarean section should only be performed when a vaginal delivery places the newborn or mother at risk because of medical reasons (e.g. labour dystocia or non-reassuring fetal heart tracing). 3 However, some women, particularly in under-developed countries and areas, opt for a caesarean section without a medical reason due to the mother’s age, fear of childbirth, child’s health considerations, provider’s fears of malpractice and higher reimbursement for caesarean birth.3–5 Non-medically related caesarean section has a significant effect on maternal and fetal health, leading to a higher risk of stillbirth and subsequent ectopic pregnancy, and higher obesity and immune disease risks for children at later stages.6–8 Hence, reducing non-medical caesarean births has been a focus in under-developed and developing countries.
Caesarean section use has prevailed in China over the past several decades, and the caesarean section rates rose sharply from 29.4% in 1993 to 54.6% in 2011. 9 The Chinese central government has launched multiple efforts to reduce these rates through public health education and penalties for hospitals with high caesarean section rates. 10 These efforts resulted in considerable progress. In 2014, the rate of caesarean sections in China declined to 34.9%, which was the lowest level in two decades. 11 Despite this decrease in the overall caesarean section rate in China, there are large geographic variations in caesarean section rates, with a mean of 57% in mega-urban cities such as Beijing and Shanghai, and less than 20% in rural areas in Western China. 11 The Province of Inner Mongolia is a large geographical area with a low population density and a large minority population distributed in rural areas. At the end of 2016, rural residents accounted for one-third of the total population in Inner Mongolia. In China, the healthcare systems in rural areas have progressed since 2010. The government of Inner Mongolia launched a series of programmes to improve the skills of rural health professionals, such as providing medical treatment counterpart support from mega-urban top-ranked hospitals. As a result, prenatal visits and maternal healthcare utilization increased in rural Inner Mongolia. In this context, caesarean section rates need to be investigated in rural minority regions, such as Inner Mongolia, and the differences between rural and urban hospitals need to be compared. To the best of our knowledge, there have not been any studies that have examined rural–urban disparities in caesarean section rates, particularly in the context of a drastic reduction in the overall caesarean section rates in minority areas.
This study aimed to assess the rural–urban disparity in caesarean section rates using electronic health records from three major hospitals in both rural and urban areas in the Province of Inner Mongolia, one of the biggest provinces in China with a large minority population. These electronic health records were analysed by multinomial regression to examine rural–urban disparities in caesarean section rates in minority areas in China.
Patients and methods
Study design
This retrospective study extracted data from the electronic health records of pregnant women that were admitted and gave birth between January 2012 and December 2016 in three major public hospitals (two urban hospitals and one rural hospital) in Inner Mongolia. In China, major healthcare facilities are mostly government owned, and therefore, public hospitals dominate the market and admit the largest patient population in each administrative region. 12 Hence, pregnant women that gave birth in these three hospitals represent the largest pregnancy population in the Province of Inner Mongolia. In this study, the three hospitals are referred to as Hospital A, Hospital B and Hospital C. Hospital A (Maternal and Children Health Hospital of Inner Mongolia), located in the capital city Hohhot of Inner Mongolia, is a first-class hospital with 121 beds and 900 obstetric staff, specializing in maternal care and child health. Hospital B (General Hospital of Xilin Gol City), with 36 beds and 40 obstetric staff, is a general hospital located in a city in the middle of Inner Mongolia with a large minority population. Hospital C (General Hospital of Ningcheng Country) is also a general hospital, with 35 obstetric health providers and 65 beds. It is located in a rural area in the eastern part of Inner Mongolia and primarily provides health services to rural residents.
This study was approved by the Institutional Review Boards from the Maternal and Children Health Hospital of Inner Mongolia, General Hospital of Xilin Gol City and General Hospital of Ningcheng Country (there were no Ethics Committee reference numbers). This study did not use any non-routine procedures. Data use was approved by the Institute of Public Health Policy of Inner Mongolia Autonomous Region. Written informed consent was provided by the study participants.
Data collection
Patient-level information included mode of delivery, maternal baseline characteristics at hospital admission and information on newborns. Women who were unable to provide data regarding their ethnicity, their age and mode of delivery, and those with multiple pregnancies were excluded from this study.
The primary outcome variable of the study was the delivery mode, which was represented by two indicators for planned and emergency caesarean sections. Here, planned caesarean and emergency caesarean sections were distinguished and studied simultaneously. Planned caesarean section is usually decided and planned before labour begins, either based on medical reasons for maternal requirements or based on maternal requirements without a clear medical indication. Emergency caesarean section occurs during labour when urgent medical complications take place, such as obstructed labour or problems with the placenta or umbilical cord. 13
The primary covariate of interest was the indicator of rural–urban residency of the pregnant women. This variable was determined by the status of the subject in the China Household Registration System, which indicates whether the place of residence was officially identified as a rural or an urban area. 14 Other covariates included maternal demographic characteristics (age and ethnicity), type of health insurance coverage, employment status and reproductive history. All these pieces of information were obtained from the hospital electronic health records.
Demographic characteristics comprised of maternal age (classified into four groups; ≤24, 25–29, 30–34 and ≥35 years) and ethnicity (Han or Minority). Types of health insurance coverage included three categories: (i) self-pay; (ii) new rural cooperative medical scheme (NCMS) coverage: (iii) urban health insurance scheme coverage. Under China’s healthcare policy, only rural residents are eligible to enrol in and subsequently be covered by the NCMS, while urban residents are eligible for enrolment into one of the urban health insurance schemes, depending on their employment status. The maternal reproductive history referred to the number of pregnancies prior to the current birth. The mother’s employment status was a categorical variable indicating that the woman was either a rural farmer or self-employed, an urban employee or unemployed.
Statistical analyses
All statistical analyses were performed in the R statistical environment (R Version 3.5.1, 2018; The R Foundation for Statistical Computing Platform). A descriptive analysis was conducted to represent the baseline characteristics of the study population and the results were also stratified by rural or urban residence. Rural versus urban group comparisons were conducted using the two-proportion z-test. Multinomial logistic regression analysis, stratified by mode of delivery (vaginal delivery, emergency caesarean and planned caesarean), was used to determine factors associated with emergency and planned caesarean section procedures. Taking vaginal delivery as the baseline, the model reported the odds ratio (OR) of rural residency in emergency and planned caesarean sections. The sample population was stratified into multiple categories according to first-time pregnancy, minority group and different age groups (≤24, 25–29, 30–34 and ≥35 years). Separate multinomial logistic regression analyses were performed to examine the rural–urban caesarean section disparities in these study subgroups. A P-value < 0.05 was considered statistically significant.
Results
The electronic health records were extracted for 62 269 pregnant women that were admitted into three hospitals between 2012 and 2016. Women who were unable to provide data regarding their own age (n = 77) and mode of delivery (n = 144) and those with multiple pregnancies (n = 145) were excluded from this study. The final study sample included 61 903 pregnant women that had a live birth (Figure 1). The mean ± SD age of the included women was 29.03 ± 4.66 years.

Flow chart of the study population.
With regard to the rural–urban disparities in caesarean section rates from 2012 to 2016, Table 1 presents summary statistics from the study sample in terms of percentages of the study subjects. From 2012 to 2016, among the 61 903 women that delivered newborns in one of three major public hospitals, approximately 40% (n = 24 715) had caesarean section births and of these, 11% (2795 of 24 715) received an emergency caesarean section procedure due to unanticipated medical conditions during labour. The remaining were planned caesarean section births. The caesarean section rate varied from urban to rural hospitals. Women in the rural hospital had a significantly higher rate of overall caesarean section than women in the urban hospitals (P < 0.001), but had a significantly lower rate of emergency caesarean section (P < 0.001). There were also substantial differences in most demographic characteristics of women in rural and urban areas. The prevalence of caesarean sections in ethnic minorities was significantly lower in rural mothers compared with urban mothers (P < 0.001). In addition, approximately 25% (3449 of 13 970) and 42% (20 001 of 47 933) of rural and urban women, respectively, were pregnant for the first time (P < 0.001). The newborn’s sex was significantly different between rural and urban areas (P < 0.001). Among the newborns, approximately 55% (7669 of 13 970) were male in rural areas, while only 43% (20 760 of 47 933) were male in urban areas. Due to the healthcare settings, rural women were predominantly insured by NCMS (65%; 9099 of 13 970) or were self-paid (34%; 4708 of 13 970), while urban women either received insurance coverage through their employers (68%; 32 708 of 47 933) or were self-paid (29%; 13 906 of 47 933) (P < 0.001 for all between-group comparisons).
Summary statistics presented as the percentage of women in each category in the final sample (n = 61 903).
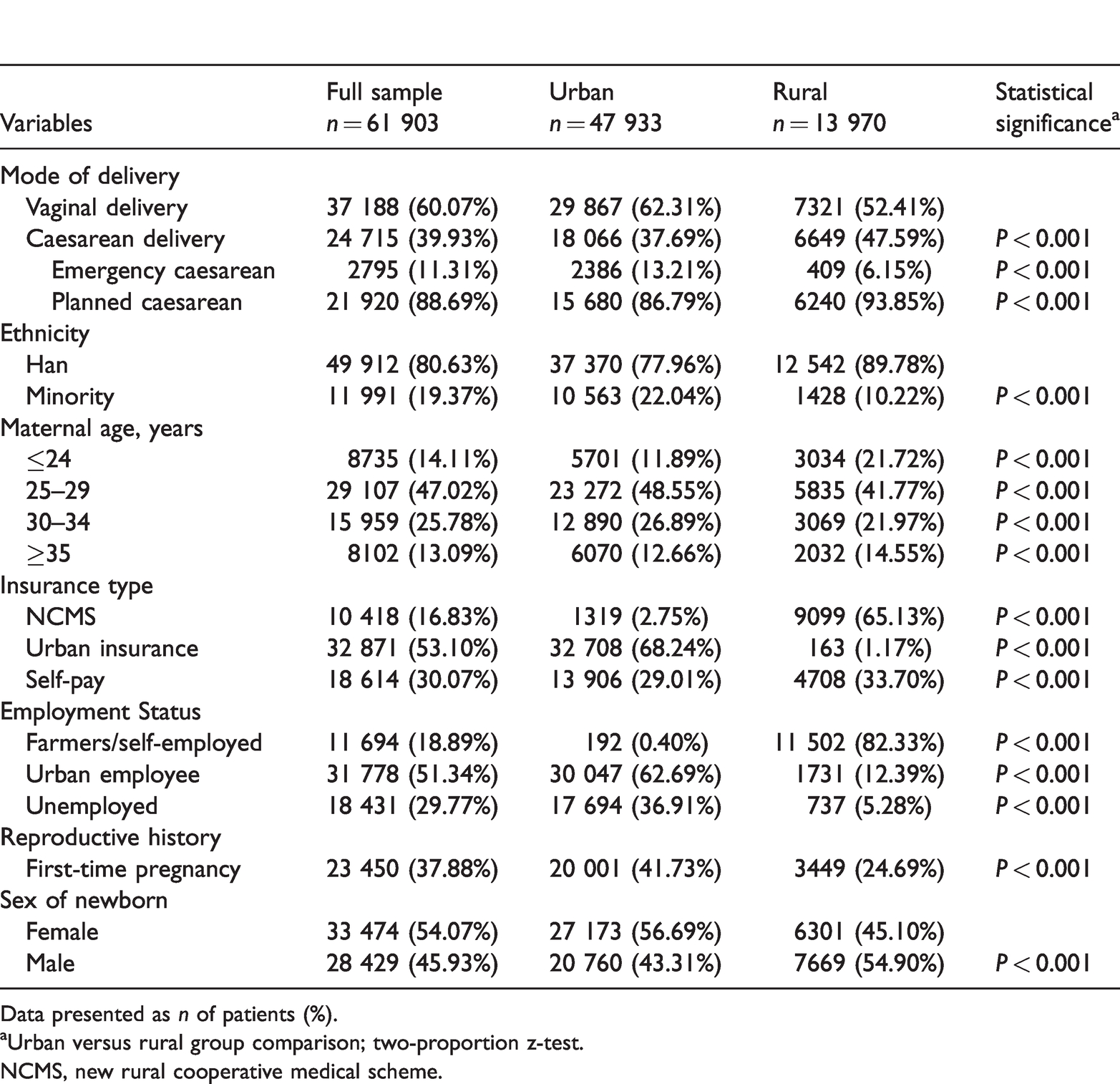
Data presented as n of patients (%).
aUrban versus rural group comparison; two-proportion z-test.
NCMS, new rural cooperative medical scheme.
The longitudinal trajectory of caesarean section rates in rural and urban hospitals was analysed. Figure 2 presents the quarterly trend of births between 2012 and 2016. From a total of 2675 births in the first quarter of 2012, the total number of babies born increased to 4329 at the end of 2014, decreased to 2654 in the first quarter of 2015, and increased again to 3496 in the first quarter of 2016. The number of delivered babies in rural areas remained relatively stable, with only a slight increase from 678 in the first quarter of 2012 to 839 in the last quarter of 2016, peaking in the fourth quarter of 2014. The number of pregnant women and babies in urban areas fluctuated greatly over the study period; increasing from 1997 in the first quarter of 2012 to 3304 in the fourth quarter of 2014, decreasing to 1604 in the second quarter of 2015, and increasing again to 3179 in the final quarter of 2016. Figure 3 presents the quarterly trend of caesarean birth rates between 2012 and 2016. Overall, the rate of caesarean births increased from 34% (898 of 2675) in the first quarter of 2012 to 40% (1618 of 4018) in the final quarter of 2016, with considerable variation between urban and rural hospitals. In the rural hospital, the caesarean birth rate was 33% (222 of 678) in the first quarter of 2012. This increased to 49% (303 of 622) in the third quarter of 2013, peaked at 63% (298 of 474) in the second quarter of 2015, decreased slightly in early 2016, and continued to increase to a rate of 62% (523 of 839) by the end of 2016. In contrast, the rate of caesarean births in urban hospitals was 34% (676 of 1997) in the first quarter of 2012, slightly increased in later quarters, and peaked at 42% (1080 of 2595) in the middle of 2014. The rate remained relatively stable between 2014 and 2015, while it fluctuated during 2015 and 2016. The rate of caesarean births was 34% (1095 of 3179) at the end of 2016. Figure 4 presents the direct measure of rural–urban disparity in caesarean section rates during the study period. The disparity was negative in 2012, which indicated that the caesarean section rate was lower in the rural hospital compared with the urban hospitals. As the caesarean section rate in rural areas had increased substantially since 2013, the rural–urban disparity became positive and the difference in rural and urban caesarean section rates peaked at 28% at the end of 2016.
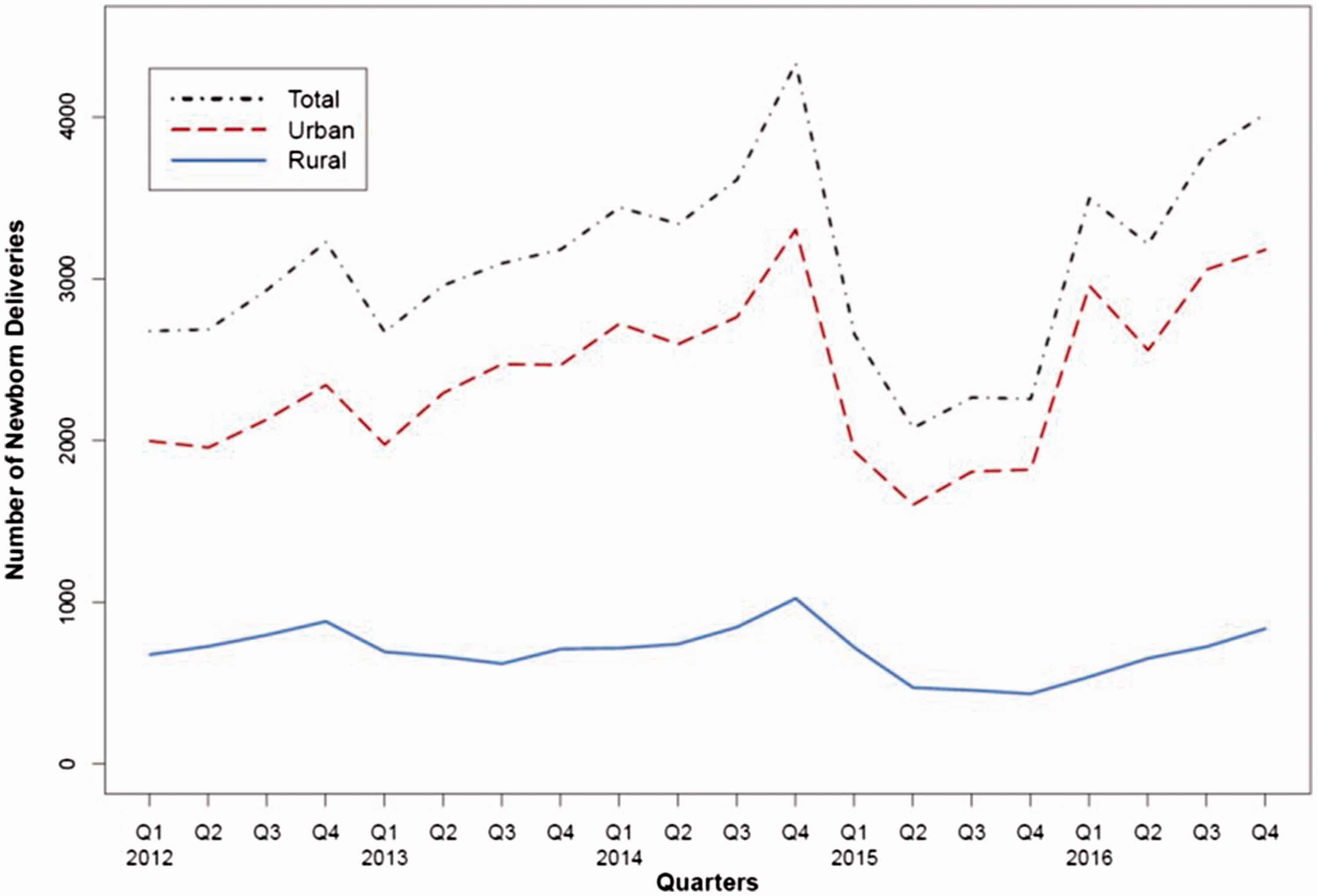
Number of newborns delivered in Inner Mongolian hospitals from January 2012 to December 2016 (5 years; 20 quarters). The colour version of this figure is available at: http://imr.sagepub.com.

Trend of caesarean section rates in Inner Mongolian hospitals from January 2012 to December 2016 (5 years; 20 quarters). The colour version of this figure is available at: http://imr.sagepub.com.

Disparity (difference) of caesarean section rates between rural and urban hospitals in Inner Mongolia, as assessed for each quarter from January 2012 to December 2016.
Results from multinomial logistic regression analyses are summarized in Tables 2 and 3. Using vaginal delivery as the baseline, the ORs of emergency and planned caesarean sections for different risk factors were calculated (Table 2). The odds of emergency caesarean sections were not significantly different between rural and urban women (OR 0.93; 95% confidence interval [CI] 0.75, 1.15), but the odds for planned caesarean births was higher for rural women than for urban women (OR 1.77; 95% CI 1.62, 1.93; P < 0.001). Age appeared to be an important risk factor for caesarean sections. Significant age effects were observed for both emergency and planned caesarean births (P < 0.001 for all comparisons). Compared with Han residents, minority women had an increased odds of undergoing both emergency caesarean section (OR 1.18; 95% CI 1.07, 1.30; P < 0.001) and planned caesarean section (OR 1.25; 95% CI 1.20, 1.31; P < 0.001). NCMS was associated with an increased risk of emergency caesarean (P < 0.01) and planned caesarean (P < 0.001), but urban insurance was only associated with an increased risk of planned caesarean (P < 0.001). Employment status (farmers/self-employed) was associated with a lower odds of emergency caesarean section (OR 0.63; 95% CI 0.50, 0.80; P < 0.001). Compared with unemployed women, urban employed women were significantly associated with a planned caesarean section during labour (OR 1.20; 95% CI 1.15, 1.25; P < 0.001), but they were not associated with emergency caesarean births. Women who were pregnant for the first time were significantly less likely to have a planned caesarean section during labour (OR 0.91; 95% CI 0.87, 0.94; P < 0.001), but they were not associated with emergency caesarean births. Delivering a male newborn was associated with higher odds for emergency caesarean birth (OR 1.22; 95% CI 1.13, 1.32; P < 0.001) and planned caesarean birth (OR 1.06; 95% CI 1.03, 1.10; P < 0.01).
Odds ratios of rural/urban residency and other factors on planned and emergency caesarean sections.
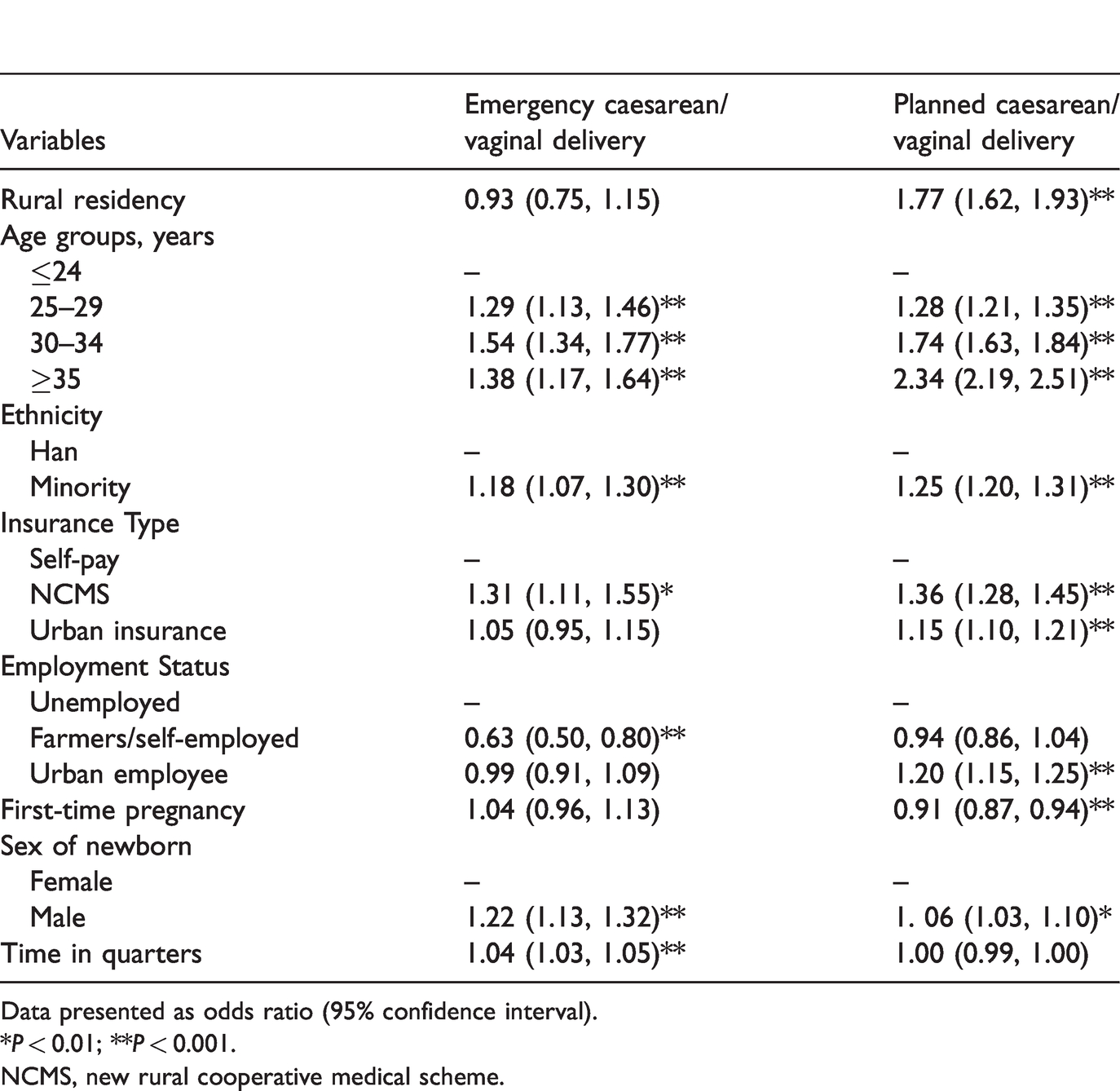
Data presented as odds ratio (95% confidence interval).
*P < 0.01; **P < 0.001.
NCMS, new rural cooperative medical scheme.
Odds ratios of rural versus urban residency for planned and emergency caesarean deliveries according to stratified samples of first-time pregnancy, minority group and age groups.

Data presented as odds ratio (95% confidence interval).
*P < 0.01; **P < 0.001.
Table 3 presents the ORs of rural residency on the caesarean delivery mode in the stratified samples. Among the women in their first pregnancy, rural women had a lower odd of receiving an emergency caesarean section when giving birth (OR 0.55; 95% CI 0.43, 0.69; P < 0.001), but had a higher odd of receiving a planned caesarean birth (OR 2.08; 95% CI 1.93, 2.24; P < 0.001). Similar significant patterns persisted for the minority group and the four age groups.
Discussion
Inner Mongolia is an Autonomous Region in China. Inner Mongolia comprises a large geographical area and ethnic diversity, making it the third largest subdivision of China. This current study examined the rural–urban disparities in caesarean sections during labour in Inner Mongolia, which has a large minority population. This current study found that the caesarean section rate in rural areas were 48%, which was 10% higher than those in urban areas. Between 2012 and 2016, such disparities ranged from −1% to 28%. There were significant rural–urban disparities in the planned caesarean section rate, but not in the emergency caesarean section rate in the Province of Inner Mongolia. The percentage of women older than 35 years and the percentage of male newborns were higher in the rural hospital than in the urban hospitals during the study period. The reasons for these findings may be associated with the ease of certain restrictions in rural and minority areas, so that families in rural and minority areas can have more than one child. 15 A previous study showed that delivered male newborns and women aged 30 years or older were associated with both emergency and planned caesarean sections. 16 Possible reasons for the finding in this current study that there was a high planned caesarean section rate in rural areas, which affected rural–urban disparities, may include the following.
First, hospitals in rural areas previously had a lower rate of caesarean births than hospitals in urban cities. 17 The reason for this finding is mainly due to the lack of good care for pregnant women caused by outdated equipment and a shortage in well-trained physicians and nurses. 18 In such an environment, pregnant women with complicating factors would go to urban hospitals to deliver their children, rather than rural hospitals. In addition, rural hospitals may have transferred or referred their patients to urban hospitals if a caesarean birth procedure was needed or requested. This situation has changed since 2010 during a period of healthcare system reform in China. At this time, central and local governments substantially invested in rural hospitals, helping them purchase advanced equipment and train clinical staff. 19 Rural hospitals had opportunities to partner with at least one urban hospital to provide training and mentoring programmes for their physicians, with a goal of providing better quality of care to their patients. 20 This developmental trajectory for rural hospitals may have resulted in a large increase in their patient population, including women seeking obstetric care. Hence, there may have been increased requests and needs for caesarean section procedures in rural hospitals, which reduced the rate of caesarean births in their urban counterparts. 21
Secondly, although maintaining low caesarean birth rates is a regulatory and clinical requirement in hospitals in China, only urban hospitals faced strict penalties, while rural hospitals receive more lenient treatment. As a result, physicians in rural hospitals do not have the same pressure as their peers in urban hospitals to strictly follow clinical rules. These current results support this situation. Women in rural areas had a significantly higher rate of planned caesarean sections than women in urban areas, but no significant difference was found in the emergency caesarean section rate between these two groups. The rationale for planned caesarean births included both maternal requirements for such procedures and medical necessities. Because emergency caesarean births are often based on medical reasons, these current findings suggest that the planned caesarean section rate was higher in rural areas compared with urban areas, partly due to the lack of regulation enforcement in rural areas.
Finally, caesarean section births may result be from physician-induced procedures. Researchers have found that, in China, physicians may play a self-interest role in the process of recommending caesarean section because they can make more profit from the higher insurance reimbursement and receive ‘tips’ from families. This phenomenon is more serious in rural hospitals compared to urban hospitals.5,22
This current study had several limitations. First, the patient-level records did not include a clinical indication regarding pre-labour caesarean section decisions. Therefore, it was not possible to distinguish between planned caesarean sections due to medical reasons and non-medically elective caesarean births. For example, a woman that had a diagnosis of fetal distress could still have a vaginal birth, while another woman with the same diagnosis could receive a caesarean section procedure. This current study used an alternative approach to identify emergency caesarean and planned caesarean births, which only partially solved this problem. Future research will study the decision of a planned caesarean. Secondly, the percentage of rural women who delivered their newborns at urban hospitals cannot be identified between 2012 and 2016. Thirdly, this study assessed the rural–urban disparities in caesarean births in minority areas in Inner Mongolia in China. Whether these conclusions can be generalized to other minority areas remains unclear because there may be variations in resource availability, policy requirements and care patterns.
In conclusion, this current study showed that recent caesarean section rates were generally reduced in the Province of Inner Mongolia between 2012 and 2016 but were still higher than the World Health Organization recommendations. The caesarean birth rate tended to increase in rural areas, and the rural–urban disparity in caesarean section rates increased each year. Further studies are required to identify which characteristics of patients and physicians, as well as regulatory policies, may affect such a disparity.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
Dr Lili Kang’s research was partially supported by the Construction Project of Health Policy Institute of Inner Mongolia and Social Medicine Programme and Scientific Research Starting Foundation for Doctoral Scholars in Inner Mongolia Medical University. Dr Bo Zhang’s research was partially supported by a National Institutes of Health grant (no. U24 AA026968) and by grants from the University of Massachusetts Center for Clinical and Translational Science (no. UL1TR001453, no. TL1TR01454 and no. KL2TR01455).