
Abstract
Objective
To evaluate the clinical efficacy of Baihe Gujin decoction combined with anti-tuberculosis therapy in mitigating the symptoms of pulmonary tuberculosis and to measure the effect on the CD4+ CD25+ regulatory T cell (Treg) ratio.
Methods
This randomized study enrolled patients with pulmonary tuberculosis and randomly assigned them to one of two treatment groups: an anti-tuberculosis treatment group and a combined treatment group. Bronchoalveolar lavage was performed before and 2 weeks after treatment. The ratio of CD4+ CD25+ Treg cells and the levels of tumour necrosis factor (TNF)-α, interleukin (IL)-4, IL-6 and IL-12 in peripheral blood and bronchoalveolar lavage fluid were measured. Symptoms were recorded before and after treatment.
Results
A total of 100 patients were enrolled and assigned to the anti-tuberculosis (n = 58) and combined treatment groups (n = 42). In the combined treatment group, Leicester Cough Questionnaire score, erythrocyte sedimentation rate, CD4+ CD25+ Treg cell ratio in bronchoalveolar lavage fluid, cytokine levels, chest pain score and sleep disorder score were significantly decreased compared with the anti-tuberculosis treatment group after treatment. The leukocyte count, haemoglobin level, platelet and alanine aminotransferase levels did not differ significantly between the two groups after treatment. The creatinine level in the combined treatment group was significantly lower than that in the anti-tuberculosis treatment group.
Conclusion
Baihe Gujin decoction combined with anti-tuberculosis treatment can effectively alleviate the symptoms of pulmonary tuberculosis, enhance the host immune function and protect renal function.
Keywords
Introduction
Pulmonary tuberculosis is a prevalent disease in China, which severely affects the quality of life of the patients. 1 Chronic cough is the most common symptom of pulmonary tuberculosis. The main immune protective mechanism against pulmonary tuberculosis is cellular immunity. Regulatory T (Treg) cells are a special subset of T cells that play a pivotal role in preventing the incidence of autoimmune diseases by inhibiting the harmful activities of immune cells. 2 According to the dialectical treatment of traditional Chinese medicine, traditional Chinese medicine adjuvant treatment based upon the patient’s different signs and symptoms can adjust the Yin and Yang balance, enhance host immunity and disease resistance, accelerate the elimination of sputum bacteria and reduce the adverse reactions induced by use of Western medicine. It can not only cure the symptoms, but also treat the cause of disease, which significantly improves the healing rate. 3
Pulmonary tuberculosis is considered to be induced by a Yin deficiency of the lung and kidney, which is the basic pathogenesis of pulmonary tuberculosis. If the disease progresses further, it can also cause both Qi and Yin symptoms; and Yin signs affect the Yang and eventually disrupt the Yin–Yang balance. Baihe Gujin decoction is a classic prescription in traditional Chinese medicine, which is widely applied in the treatment of pulmonary tuberculosis by practitioners of traditional Chinese medicine.
Despite its widespread use, the clinical efficacy, relevant data and the underlying mechanisms of action, especially its effect on cytokines and immune mechanisms, of Baihe Gujin decoction in the management of pulmonary tuberculosis have been rarely reported. This present study investigated the clinical efficacy of Baihe Gujin decoction combined with anti-tuberculosis therapy in mitigating the symptoms of pulmonary tuberculosis with Yin-deficiency and Fire-hyperactivity syndrome. The study measured the effect of treatment on the CD4+ CD25+ Treg ratio in peripheral blood samples and bronchoalveolar lavage fluid (BALF) and cough symptoms, with the aim of providing clinical evidence for the application of Baihe Gujin decoction in the management of pulmonary tuberculosis in clinical practice.
Patients and methods
Patient population and study design
This randomized study enrolled patients diagnosed with pulmonary tuberculosis with Yin-deficiency and Fire-hyperactivity syndrome in Nanjing Chest Hospital, Nanjing, Jiangsu Province, China from April 2016 to January 2018. The inclusion criteria were as follows: (i) patients with positive pulmonary tuberculosis based on smear testing for the first time; (ii) those presenting with the symptoms of Yin-deficiency and Fire-hyperactivity syndrome, such as cough, shortness of breath, sticky sputum, hot flushes, cheek redness, night sweats, sleep disorder, chest pain, haemoptysis, spermatorrhoea, irregular menstruation, weight loss, fatigue, dark red tongue, relatively low levels of haemoglobin and red blood cells; (iii) adults diagnosed with secondary pulmonary tuberculosis except those with non-tuberculous mycobacterial infection; (iv) those with active pulmonary tuberculosis confirmed by X-ray chest imaging; (v) those aged > 18 years old; (vi) those taking care of themselves independently; (vii) those with normal liver and kidney function; (viii) those with fasting blood glucose level < 7.0 mmol/l. The exclusion criteria were as follows: (i) those diagnosed with severe primary diseases affecting anti-tuberculosis treatment, such as various types of advanced-stage malignant tumours, haematological diseases, persistent state of bronchial asthma, severe hepatorenal insufficiency, severe pneumonia, acute exacerbation of severe chronic obstructive pulmonary disease and respiratory failure; (ii) those failing to tolerate bronchoscopy or those unwilling to undergo bronchoscopy; (iii) those with mental retardation, cognitive impairment or mental disorders; (iv) those failing to clearly describe the symptoms and unable to cooperate with the doctors; (v) those participating in clinical trials for other drugs; (vi) those with adverse events in the past 3 months. In addition, those receiving other medications that might affect the therapeutic efficacy of the test medications, those with incomplete data, those with poor compliance, patients lost to follow-up and those that voluntarily withdrew from the study were excluded. The patients were randomly divided into an anti-tuberculosis treatment group and a combined treatment group using a computer-generated randomization schedule. In the anti-tuberculosis treatment group, patients received conventional anti-tuberculosis treatment as described below. In the combined treatment group, patients received traditional anti-tuberculosis treatment in combination with Baihe Gujin decoction as described below.
The study procedures were approved by the Ethics Committee of the Third Affiliated Hospital of Nanjing University of Chinese Medicine (no. 2016-KL018-D1). Written informed consent was obtained from all study participants.
Therapeutic process
After the diagnosis of tuberculosis was confirmed, anti-tuberculosis and hepatoprotective agents were administered in the anti-tuberculosis treatment group. The drugs included: isoniazid (Jiangsu Zhengdafenghai Pharmaceutical, Nanjing, China; 0.3 g, orally, once daily); rifampicin (North China Pharmaceutical Group, Shijiazhuang, China; 0.45 g, orally, once daily); ethambutol (Shanghai Xinyi Pharmaceutical, Shanghai, China; 0.75 g, orally, once daily); pyrazinamide (Shanghai Xinyi Pharmaceutical; 0.5 g, orally, three times a day); bicyclol (Beijing Union Pharm, Beijing, China; 25–50 mg, orally, three times a day); diammonium glycyrrhizinate enteric coated capsule (Zhengda Tianqing Pharmaceutical Group, Lianyungang, China; 150 mg, orally, three times a day. The anti-tuberculosis treatment group was treated using the conventional anti-tuberculosis 2HERZ/4HR regime (H, isoniazid; R, rifampicin; Z, pyrazinamide; E, ethambutol. 2, 2 months; 4, 4 months; 2HERZ/4HR represented intensive treatment with HERZ for 2 months, followed by consolidation treatment with HR for 4 months) for 6 months.
The Baihe Gujin decoction included the following substances: steamed Rehmannia glutinosa 9 g; dried Rehmannia glutinosa 9 g; Angelica sinensis 9 g; Paeonia latiflora 3 g; Glycyrrhiza uralensis Fisch 3 g; Campanulaceae campanuloideae 3 g; Digitalis purpurea 3 g; Fritillaria cirrhosa 12 g; Ophiopogon japonicus 12 g; Lilium brownii 12 g. A bag (200 ml) of the preparation was obtained by decocting with water using an automatic traditional Chinese medicine decocting machine (Tianshui Huayuan Medical Equipment, Tianshui, China) and packaged by the Department of Traditional Chinese Medicine, Nanjing Chest Hospital. In the combined treatment group, patients received Baihe Gujin decoction (200 ml, orally, once daily) combined with the conventional anti-tuberculosis 2HERZ/4HR regime for 6 months.
The Leicester Cough Questionnaire (LCQ) 4 and Cough Symptom Score were utilized to assess the initial symptoms before and at 4 weeks after the treatment interventions. Routine blood tests, biochemical examinations, erythrocyte sedimentation rate and the levels of tumour necrosis factor (TNF)-α (Shenzhen Kerunda Bioengineering, Shenzhen, China), interleukin (IL)-4 (Beijing BLKW Biotechnology, Beijing, China), IL-6 (Beijing BLKW Biotechnology) and IL-12 (Beijing BLKW Biotechnology) were quantitatively measured using commercial kits according to the manufacturer's instructions before and at 2 weeks after the treatment interventions. Bronchoalveolar lavage was performed under bronchoscopy and the BALF was immediately collected for detection of CD4+ CD25+ Treg cells using flow cytometry (Bio-Rad, Hercules, CA, USA) before and at 2 weeks after the treatment interventions. Patients were permitted to receive other drugs throughout the study.
Clinical efficacy and adverse events
The LCQ and Cough Symptom Score were used to evaluate the severity of cough symptoms. A visual analogue scale was used to evaluate the scores of clinical symptoms that included shortness of breath, hot flashes, night sweats, sleep status and the severity of chest pain. At 2 weeks after the treatment interventions, the percentage of patients who were negative for sputum bacteria among all participants was calculated. The difference in the erythrocyte sedimentation rates before and at 2 weeks after the treatment interventions were observed and statistically compared between the two groups. The quantity and percentage of severe adverse events, such as severe hepatic insufficiency, renal insufficiency and myelosuppression, were counted and recorded.
Gating strategy used in flow cytometry
As shown in Figure 1, flow cytometric analysis was performed to identify the lymphocyte populations in the peripheral blood and BALF samples using the forward scatter as the x-axis and the sagittal scatter as the y-axis. Then, the proportion of CD4+ T cells in the lymphocyte population was analysed. Subsequently, the proportion of CD4+ CD25+ Foxp3+ Treg cells was investigated.

Representative images showing the flow cytometry gating strategy used in this study. The colour version of this figure is available at: http://imr.sagepub.com.
Statistical analyses
All statistical analyses were undertaken using IBM SPSS® Statistics for Windows®, Version 19.0 (IBM Corp., Armonk, NY, U.S.A). The statistical differences in the age and sex were quantitatively measured. Continuous data were first tested for normal distribution. If normally distributed, the data were expressed as mean ± SD. Independent sample t-test was used to compare the continuous data between two groups before and after the treatment interventions. A P-value ≤ 0.05 was considered statistically significant.
Results
This randomized study enrolled 100 patients (55 males and 45 females) diagnosed with pulmonary tuberculosis with Yin-deficiency and Fire-hyperactivity syndrome and randomly divided them into an anti-tuberculosis treatment group (n = 58) and a combined treatment groups (n = 42) (Table 1). The mean age and sex ratio did not differ significantly between the two groups.
Baseline demographic data of the patients (n = 100) enrolled in a study to investigate the efficacy of the traditional Chinese medicine Baihe Gujin decoction in the management of pulmonary tuberculosis in clinical practice.
Data presented as mean ± SD or n of patients.
No significant between-group differences (P > 0.05); independent sample t-test.
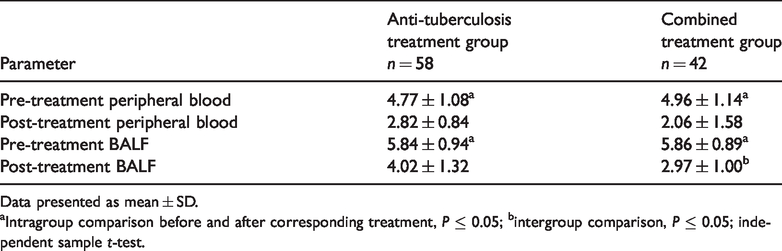
The relevant parameters evaluating the clinical efficacy are presented in Table 2. The erythrocyte sedimentation rate, LCQ score, cough symptom score, CD4+ CD25+ Treg cell ratio in the BALF and peripheral blood, shortness of breath, night sweats, hot flashes, chest pain and sleep disorder at baseline did not differ significantly between the two groups. Similar changes were observed in the two groups after the treatment interventions. The erythrocyte sedimentation rate, LCQ score, cough symptom score, CD4+ CD25+ Treg cell ratio in the BALF and peripheral blood were significantly reduced after both treatment interventions (P ≤ 0.05 for all intragroup comparisons). In the combined treatment group, the erythrocyte sedimentation rate, LCQ score, CD4+CD25+ Treg cell ratio in the BALF (Figure 2) and the scores of chest pain and sleep disorder were significantly improved compared with those in the anti-tuberculosis treatment group (P ≤ 0.05 for all intergroup comparisons).
Comparison of clinical efficacy between the two groups of patients (n = 100) enrolled in a study to investigate the efficacy of the traditional Chinese medicine Baihe Gujin decoction in the management of pulmonary tuberculosis in clinical practice.

Data presented as mean ± SD.
aIntragroup comparison before and after corresponding treatment, P ≤ 0.05; bintergroup comparison, P ≤ 0.05; independent sample t-test.
ESR, erythrocyte sedimentation rate; LCQ, Leicester Cough Questionnaire; CSS, cough symptom score; Treg, regulatory T cells.

Representative flow cytometric analysis of the CD4+ CD25+ regulatory T cell ratio in bronchoalveolar lavage fluid from patients enrolled in a study to investigate the efficacy of the traditional Chinese medicine Baihe Gujin decoction in the management of pulmonary tuberculosis in clinical practice: before treatment (a) and after treatment in the anti-tuberculosis treatment group (b) and the combined treatment group (c). The colour version of this figure is available at: http://imr.sagepub.com.
The levels of cytokines in the peripheral blood and BALF after treatment are presented in Table 3. The levels of TNF-α, IL-4, IL-6 and IL-12 in the peripheral blood and BALF did not significantly differ between the two groups before treatment. Similar changes were noted between the two groups after treatment in terms of the levels of TNF-α, IL-4, IL-6 and IL-12 in the peripheral blood and BALF, which were significantly down-regulated after treatment in both groups (P ≤ 0.05 for all intragroup comparisons) and were significantly down-regulated in the combined treatment group compared with the anti-tuberculosis treatment group (P ≤ 0.05 for all intergroup comparisons).
Comparison of cytokine levels in the peripheral blood and bronchoalveolar lavage fluid between the two groups of patients (n = 100) enrolled in a study to investigate the efficacy of the traditional Chinese medicine Baihe Gujin decoction in the management of pulmonary tuberculosis in clinical practice.

Data presented as mean ± SD.
aIntragroup comparison before and after corresponding treatment, P ≤ 0.05; bintergroup comparison, P ≤ 0.05; independent sample t-test.
TNF, tumour necrosis factor; IL, interleukin.
The CD4+ CD25+ Foxp3+ Treg cell ratio in CD4+ T cells in the peripheral blood and BALF of patients in the anti-tuberculosis treatment group and combined treatment group are shown in Table 4. The CD4+ CD25+ Foxp3+ Treg cell ratios in CD4+T cells in the peripheral blood and BALF before treatment were not significantly different between the two groups. After treatment, the ratios of CD4+ CD25+ Foxp3+ Treg cells in the peripheral blood and BALF were significantly decreased in both treatment groups (P ≤ 0.05 for all intragroup comparisons) and the decrease in BALF was significantly lower in the combined treatment group compared with the anti-tuberculosis treatment group (P ≤ 0.05).
Comparison of the proportion of CD4+ CD25+ Foxp3+ regulatory T cells before and after treatment in the peripheral blood and bronchoalveolar lavage fluid (BALF) between the two groups of patients (n = 100) enrolled in a study to investigate the efficacy of the traditional Chinese medicine Baihe Gujin decoction in the management of pulmonary tuberculosis in clinical practice.
Data presented as mean ± SD.
aIntragroup comparison before and after corresponding treatment, P ≤ 0.05; bintergroup comparison, P ≤ 0.05; independent sample t-test.
There were no significant differences in terms of the peripheral blood leukocyte count, haemoglobin level, platelet count, alanine aminotransferase and serum creatinine levels between the two groups prior to treatment (Table 5). After the treatment intervention, the peripheral blood leukocyte counts and alanine aminotransferase levels in the peripheral blood were significantly changed in both groups (P ≤ 0.05 for all intragroup comparisons). In the combined treatment group, the serum level of creatinine was significantly downregulated after treatment compared with before treatment (P ≤ 0.05) and significantly lower after treatment compared with the anti-tuberculosis treatment group (P ≤ 0.05). As illustrated in Figures 3a and 3b, pulmonary lesions were clearly alleviated after receiving the combined treatment. However, residual lung lesions could be observed in the anti-tuberculosis treatment group (Figures 3c and 3d).
Comparison of adverse events between the two groups of patients (n = 100) enrolled in a study to investigate the efficacy of the traditional Chinese medicine Baihe Gujin decoction in the management of pulmonary tuberculosis in clinical practice.

Data presented as mean ± SD.
aIntragroup comparison before and after corresponding treatment, P ≤ 0.05; bintergroup comparison, P ≤ 0.05; independent sample t-test.
ALT, alanine aminotransferase.

Chest computed tomography scan images of representative patients from the combined treatment group (a and b) showing that pulmonary lesions were clearly alleviated and from the anti-tuberculosis treatment group (c and d) after treatment showing the presence of residual lung lesions.
Discussion
The LCQ score, cough symptom score, shortness of breath, night sweats, hot flashes, chest pain, sleep disturbances and other symptoms can reflect the severity of the symptoms from the patient's subjective perspective. In this current study, the chest pain and sleep disorder scores of patients receiving combined treatment were significantly lower compared with those in the anti-tuberculosis treatment group. The rate of sputum smear negativity in the combined treatment group was slightly higher than that in the anti-tuberculosis treatment group, but the difference was not significant, probably due to the small sample size. The decrease in erythrocyte sedimentation rate may reflect the degree of tuberculosis activity; and the post-treatment erythrocyte sedimentation rate in the combined treatment group was significantly decreased compared with that in the anti-tuberculosis treatment group.
In terms of adverse reactions in the current study, the peripheral blood leukocyte count, haemoglobin level, platelet count, alanine aminotransferase and serum creatinine levels did not significantly differ between two groups before treatment. After the two corresponding treatment interventions, the peripheral blood leukocyte count was significantly reduced in both groups, whereas the alanine aminotransferase level was significantly elevated in both groups. There were no significant differences in the peripheral blood leukocyte count and aminotransferase levels between the two groups post-treatment, indicating that the Baihe Gujin decoction does not increase the risk of bone marrow suppression and liver function damage of anti-tuberculosis drugs. According to the theory of traditional Chinese Medicine, combined use of steamed and dried Rehmannia glutinosa can nourish the kidney, which refers to the purpose of changing renal function through diet, medicine, acupuncture, massage and other methods. There was a significant difference in the serum level of creatinine before and after treatment in the combined treatment group, suggesting that Baihe Gujin decoction exerts a protective effect upon the kidney. The significant improvement of the symptom scores in the combined treatment group indicated that the Baihe Gujin decoction was an efficacious anti-tuberculosis treatment. It functions to nourish Yin, protect the lungs and dissolve the phlegm. It can also treat internal heat, Yin deficiency, cough and shortness of breath, hot flashes and dark red tongue. Baihe Gujin decoction can be applied to treat multiple diseases induced by Yin-deficiency syndrome in the lung and kidney, such as chronic bronchitis, tuberculosis and bronchiectasis. The total saponin extract might effectively eliminate hydroxyl radicals. 5 The iridoid glycosides, sterols and verbascoside can inhibit oxidative stress by reducing the secretion of transforming growth factor-β and IL-1β, regulate endothelial cell secretion, inhibit inflammatory factors and prevent cell adhesion, thereby protecting vascular endothelial cells from the inflammatory reaction. 6 The effective components of steamed Rehmannia glutinosa include sterols, saccharides, lutein, amino acids and rehmainonoside A, B and D, which play a vital role in suppressing the progression of malignant tumours, provide anti-oxidation effects, promote haematopoiesis and have anti-aging effects. 7 Ophiopogon japonicus homoisoflavones exert effects upon anti-oxidation and anti-proliferation in human lung cancer cells (A-549). 8 The phenylpropanoid glycosides in Radix Scrophulariae have significant anti-inflammatory, hepatoprotective, anti-oxidative and anti-platelet aggregation effects.9,10 Ophiopogon japonicus can moisten the lungs with nourishing Yin and Scrophularia can alleviate the pain.11,12 As the main active ingredient of Chinese angelica, ferulic sodium can significantly down-regulate the serum levels of alanine aminotransferase, aspartate aminotransferase, IL-1β, IL-6 and TNF-α, and reduce the expression levels of liver TNF-α and nuclear factor-κB protein. 13 The anti-oxidation activity of the crude extract of pentaphylla and its active ingredient pentagalactose is significantly higher than that of vitamin C. 14 The crude extract of liquorice and its active ingredients exert bi-directional regulatory effects on the immune system, including immune enhancement and immunosuppression. 15 In addition, it also has a significant impact on the maturation status and activity of immune cells. 15 Previous research has demonstrated that the combination of Campanulaceae and liquorice increases the content of anti-inflammatory substances of glycyrrhizic acid and glycyrrhetinic acid, which significantly enhances the clinical efficacy of prescriptions. 16 Angelica sinensis is a Chinese herb, which can cure a cough. 17 White peony nourishes the blood. 18 Fritillaria can remove the heat and nourish the lungs, dissolve the phlegm and treat the cough. 19 Campanulaceae functions to mitigate the inflammation and dissolve the phlegm, and protects the liver. 20 Raw liquorice propels the heat and fire and can be used in combination with other drugs as an adjuvant therapy. 21 Modern pharmacology research validates that this prescription has anti-tuberculosis, anti-bacterial and anti-virus effects, eliminates free radicals and enhances the host immunity and regulate endocrine balance. 22 A previous study that treated 53 patients that had pulmonary tuberculosis with Baihe Gujin decoction demonstrated that the total efficacy rate was 94.3%, which was significantly higher than that in the control group. 23 In another study, 24 Baihe Gujin decoction not only treated the primary disease, but also mitigated the adverse events of anti-tuberculosis drugs on the liver. The findings above were further validated by the evidence obtained in present study with regard to the cytological findings. The above studies are consistent with the results of this current study.23,24
A previous study compared patients with diabetes mellitus and pulmonary tuberculosis treated with anti-tuberculosis therapy alone and Baihe Gujin decoction combined with anti-tuberculosis treatment. 25 After 2 months of treatment, the sputum negative conversion rates of the two groups were 56.3% and 81.9%, respectively; and the lesion improvement rates were 75.8% and 46.9%, respectively; and the differences were significant. 25 A study found that Baihe Gujin decoction combined with Shengmai powder can reduce the level of IFN-α in the serum of pulmonary tuberculosis patients and improve clinical symptoms. 26 Baihe Gujin decoction not only treats primary disease, but it also reduces the liver damage associated with anti-tuberculosis drugs. 24
In this current study, Baihe Gujin decoction was hypothesized to improve the symptoms of pulmonary tuberculosis and enhance the immune function by regulating the activity of Treg cells. A previous study found that patients with positive pulmonary tuberculosis by a sputum smear test had elevated levels of CD4+ CD25+ Treg cells compared with their counterparts with negative outcomes. 27 The increase in the proportion of Treg cells was associated with the deleterious consequences of active tuberculosis and may be related to Mycobacterium tuberculosis strains, animal models, local environment and infection stage. 28 In this current investigation, the CD4+ CD25+ Treg cell ratio in the peripheral blood and BALF in the combined treatment group was lower than that in the anti-tuberculosis treatment group after 2 weeks of treatment and the relevant symptoms were improved, indicating that Baihe Gujin decoction can down-regulate the activity of CD4+ CD25+ Treg cells.
The balance of type 1 helper T (Th1) cell/Th2/Treg is essential for controlling the progression of active tuberculosis disease.29,30 Th1 cells and IL-12 can promote inflammation and activate the infected macrophages and Mycobacterium tuberculosis. 31 Specific cytotoxic T lymphocytes from local sites of tuberculosis infection can be enhanced by IL-2, which plays a vital role in local immune reactions against tuberculosis infection. 31 Increased activity of Th2 cells, IL-4 and Treg cells effectively inhibit protective cellular immunity, which may lead to poor tuberculosis control. 32 Th2 cells and IL-6 are positively correlated with the severity of pulmonary tuberculosis and can be used as a potential biomarker for anti-tuberculosis treatment. 33 When Treg activity increases, the Th1 immune response is inhibited, eventually impairing the host immune function against Mycobacterium tuberculosis and accelerating disease progression. 34 In the present study, it was hypothesized that prior to treatment, the Treg ratio, Th1, TNF-α, IL-12, Th2, IL-4 and IL-6 levels would be elevated, reflecting the Th1/Th2/Treg imbalance. When the immune response of Th2 towards immunity is weakened, it may aggravate the severity of pulmonary disease. 35 After treatment in the current study, the levels of these cytokines were reduced, suggesting that the Th1/Th2/Treg balance had been restored.
In conclusion, Baihe Gujin decoction combined with anti-tuberculosis therapy resulted in higher clinical efficacy in mitigating the symptoms of pulmonary tuberculosis with Yin-deficiency and Fire-hyperactivity syndrome compared with anti-tuberculosis treatment alone. The combined intervention can enhance the host immunity, reduce the risk of adverse events induced by anti-tuberculosis drugs and protect the kidney probably by regulating the activity of Treg cells. These current findings provide theoretical and clinical evidence for Baihe Gujin decoction in treating pulmonary tuberculosis as a supplemental therapy along with anti-tuberculosis treatment in patients with Yin-deficiency and fire-hyperactivity syndrome.