
Abstract
Objective
To identify factors associated with outcome of septic shock patients receiving high dose noradrenaline according to three primary infection sites.
Methods
This retrospective study was based on data from a publicly available ICU database (Medical Information Mart for Intensive Care [MIMIC] III. Septic shock patients receiving high dose (≥1 μg/kg per min) noradrenaline and ≥18 years were identified and their characteristics and outcomes were compared according to three primary infection sites (abdominal, respiratory and urinary tract).
Results
154 septic shock patients who received high doses of noradrenaline were identified; (89 [58%] had a respiratory infection, 41 [27%] an abdominal infection and 24 [16%] a urinary infection). There were no differences among the three infection groups in duration/maximum dosage of noradrenaline, length of stay in the ICU/hospital, do not resuscitate (DNR) rates, hypertension and adequate antimicrobial therapy. Patients with urinary infections had a lower risk of death at 28-days compared with those with abdominal or respiratory infections.
Conclusions
The prognosis for septic shock patients receiving high dose noradrenaline is poor. Patients with abdominal or respiratory infections are at higher risk of death compared with those with urinary infections.
Introduction
Refractory shock develops in approximately 6–7% of critically ill patients and is associated with extremely high mortality. 1 For these patients, high dose vasopressor therapy is sometimes necessitated to maintain normal organ perfusion. According to the International Guidelines for Management of Sepsis and Septic Shock, noradrenaline is recommended as the first-choice vasopressor for septic shock. 2 However, high doses of noradrenaline have been associated with a poor prognosis. Mortality rates of 65–100% have been recorded in septic shock patients receiving high doses of noradrenaline (i.e., >1 μg/kg per min).3,4 These values are much higher than the average 40% mortality rate which has been reported for septic patients. 5
Abdominal, respiratory and urinary infections are the three most common causes of sepsis. 6 However, limited data are available on the characteristics and outcomes of septic shock from infections of different origin. One study that compared different outcomes of ICU patients with respiratory or abdominal infections found that septic shock was more common in patients with abdominal infections but the mortality rates in the two patient groups were similar. 7 Data are also limited on the outcomes of septic shock patients who received high doses of noradrenaline. For these patients, evaluating the risk of death is of paramount importance for both clinicians and family members when deciding whether or not to continue with intensive therapy. Therefore, the aim of this retrospective study was to identify factors associated with outcome in a cohort of septic shock patients receiving high dose noradrenaline according to three different primary infection sites (i.e., abdominal, respiratory and urinary tract).
Methods
This study was based on data from a publicly available ICU database (Medical Information Mart for Intensive Care [MIMIC] III [version 1.4]).8,9 The database contains information from 46,520 critically ill patients admitted to a single centre in the USA (Beth Israel Deaconess Medical Centre, Boston, MA) from 2001 to 2012. 9 Access to the database was approved by the Institutional Review Boards of the Massachusetts Institute of Technology (Cambridge, MA, USA) and the Beth Israel Deaconess Medical Centre after completion of a NIH web-based course named “Protecting Human Research Participants”. Patient data were anonymised and so informed consent was not required. Data were extracted from the database using structure query language (SQL) with pgAdmin4 PostgreSQL 9.6. software.
Patients, ≥18 years, with a diagnosis of septic shock and receiving high dose noradrenaline (≥1 μg/kg per min) 10,11during their first ICU admission on each hospitalization were eligible for the study. According to Sepsis-3 definition, septic shock was defined as infection or suspected infection, plus an increase in Sequential Organ Failure Assessment (SOFA) score of ≥2 points and a vasopressor requirement to maintain a proper mean arterial pressure. 5 In addition, the origin of the patients’ infection was from abdominal, respiratory or urinary tract sources. Infection or suspected infection was defined as either (a) International Classification of Diseases (ICD)-9 contained any of the following term “infection”, “pneumonia”, “meningitis”, “pyelonephritis”, “peritonitis”, “bacteraemia”, “sepsis” or “septic”, or, (b) positive microbiological culture. 12 Patients without a confirmed infection or who had more than one infection were excluded from the study. Organ failure was defined as SOFA score ≥2 for one organ 13 and inadequate antimicrobial treatment was defined as the antimicrobial agents used had no activity against the cultured pathogens. 14
Patients’ characteristics including sex, age, diagnosis on admission, comorbidities, Simplified Acute Physiology (SAP) score; SOFA score on Day 1, 3, 5 and 7, length of stay (LOS) in ICU and hospital, causative agents, do-not-resuscitate (DNR) rates and mortality were extracted from the database. DNR orders were recorded when they happened after septic shock.
Statistical analyses
The primary endpoint was 28-day mortality. Normally distributed quantitative variables were presented as mean ± standard deviation (SD) and skewed variables were summarized as median and interquartile range (IQR). Continuous data were compared using the Kruskal-Wallis U test and categorical data were compared using χ-square or Fisher’s exact test as appropriate. Significant risk factors for 28-day mortality were identified using the Wald χ-squared test (Figure 1). These factors were entered into a Cox proportional hazard model to assess their association with mortality at 28 and 90-days. Kaplan-Meier plots were used to compare differences in 28-day survival between the three primary infection sites. All analyses were performed using R version 3.3.3 for Windows (http: //www.r-project.org/) and a P-value <0.05 was considered to indicate statistical significance.

The importance of each factor as assessed by the Wald χ2 test. The significant variables were: SOFA scores on Day 1, infection sites, age >60 years, noradrenaline (norepinephrine) duration, presence of hypertension and adequate antimicrobial therapy.
Results
In total, 154 septic shock patients who received high doses of noradrenaline were identified from the database. From this cohort, 89 (58%) had an infection of respiratory origin, 41 (27%) of an abdominal origin and 24 (16%) of a urinary tract origin (Table 1). There were no significant differences between groups in age at admission, admission type, comorbidities and resuscitation endpoints. However, fluid balance status was significantly different between groups (P=0.006) (Table 1). The variations in intake and output of fluid were probably due to different requirements of fluid resuscitation volumes for the septic shock patients.
Demographic baseline characteristics of the 154 septic shock patients receiving high dose noradrenaline according to three primary infection sites.
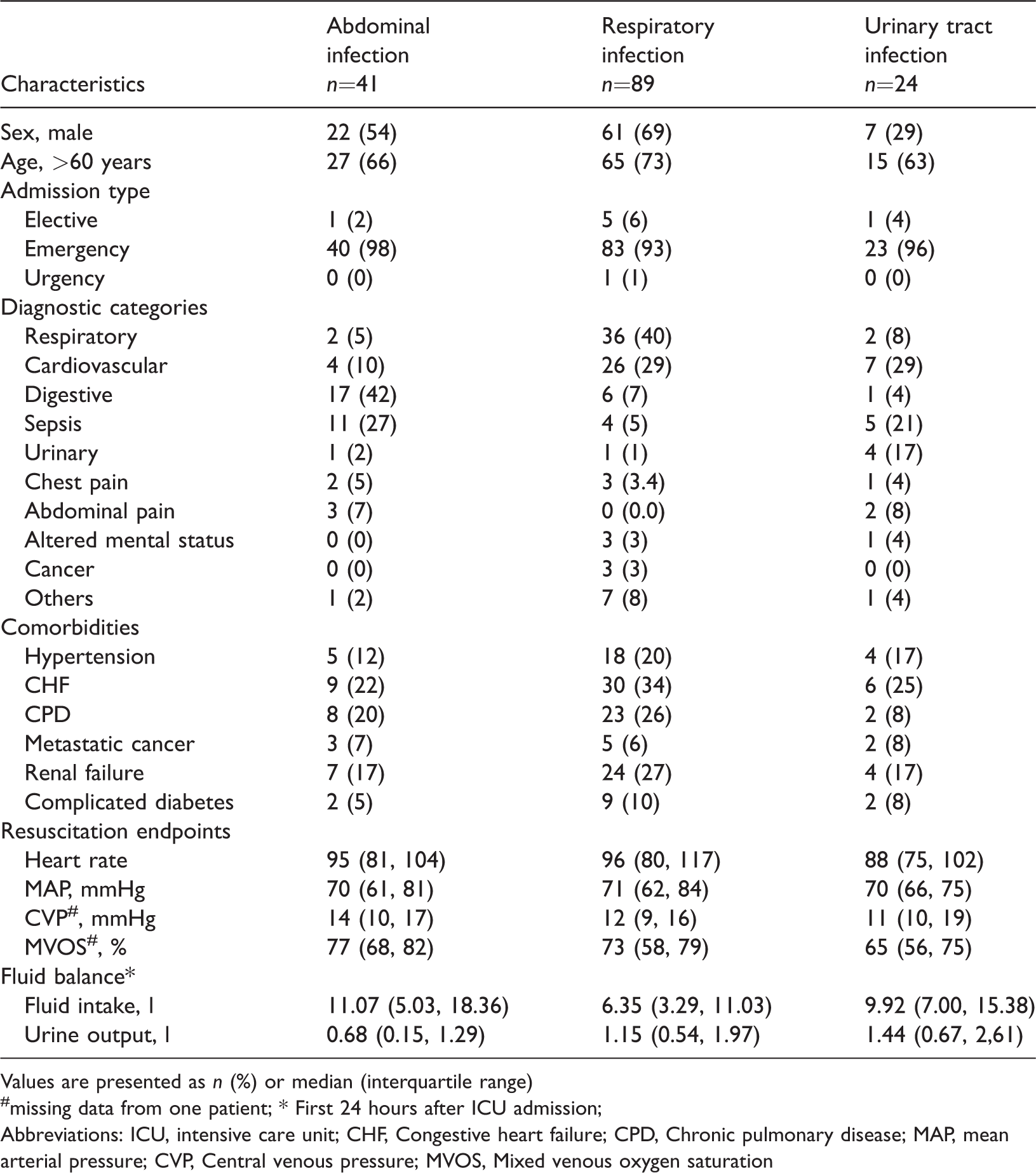
Values are presented as n (%) or median (interquartile range)
missing data from one patient; * First 24 hours after ICU admission;
Abbreviations: ICU, intensive care unit; CHF, Congestive heart failure; CPD, Chronic pulmonary disease; MAP, mean arterial pressure; CVP, Central venous pressure; MVOS, Mixed venous oxygen saturation
Although SAPS II scores and SOFA scores on day 1, 3 and 5 were comparable, SOFA scores on day 7 for the respiratory infection group were statistically significantly different (P =0.036) from the other two groups (Table 2). Unsurprisingly, patients with a respiratory infection had the highest incidence of respiratory failure (61, 69%, P =0.043) and patients with an abdominal infection tended to have more liver failure (5, 12%, P =0.040). Of note, the incidence of secondary bacteraemia in the abdominal infection group was twice that of the other infection groups (51% vs 25% and 25%).
Severity of the 154 septic shock patients receiving high dose noradrenaline according to three primary infection sites.

Values are presented as mean ± standard deviation (SD) or n (%) or median (interquartile range)
Abbreviations: SAPS II, Simplified Acute Physiology Score; SOFA, Sequential Organ Failure Assessment; CNS, central nervous system
For patients with abdominal infections, Escherichia coli (5, 12%), Pseudomonas aeruginosa (3, 7%) and Klebsiella pneumonia (4, 10%) were the most common gram-negative organisms while coagulase negative (11, 27%) and positive (9, 22%) Staphylococci were the most common gram-positive bacteria (Table 3). In addition, 9 (22%) patients with an abdominal infection had Candida. Most of the patients in the respiratory infection group (38, 43%) had positive cultures for Staphylococci. The three leading gram-negative organisms for this group of patients were, E. coli (7, 8%), P aeruginosa (9, 10%) and K. pneumonia (7, 8%). As expected, half of the patients with a urinary infection were positive for E. coli. However, most patients (85%) received adequate antibiotic treatment (Table 4).
Distribution of micro-organisms isolated from culture-positive-infected septic shock patients receiving high dose noradrenaline according to three primary infection sites (n=154).
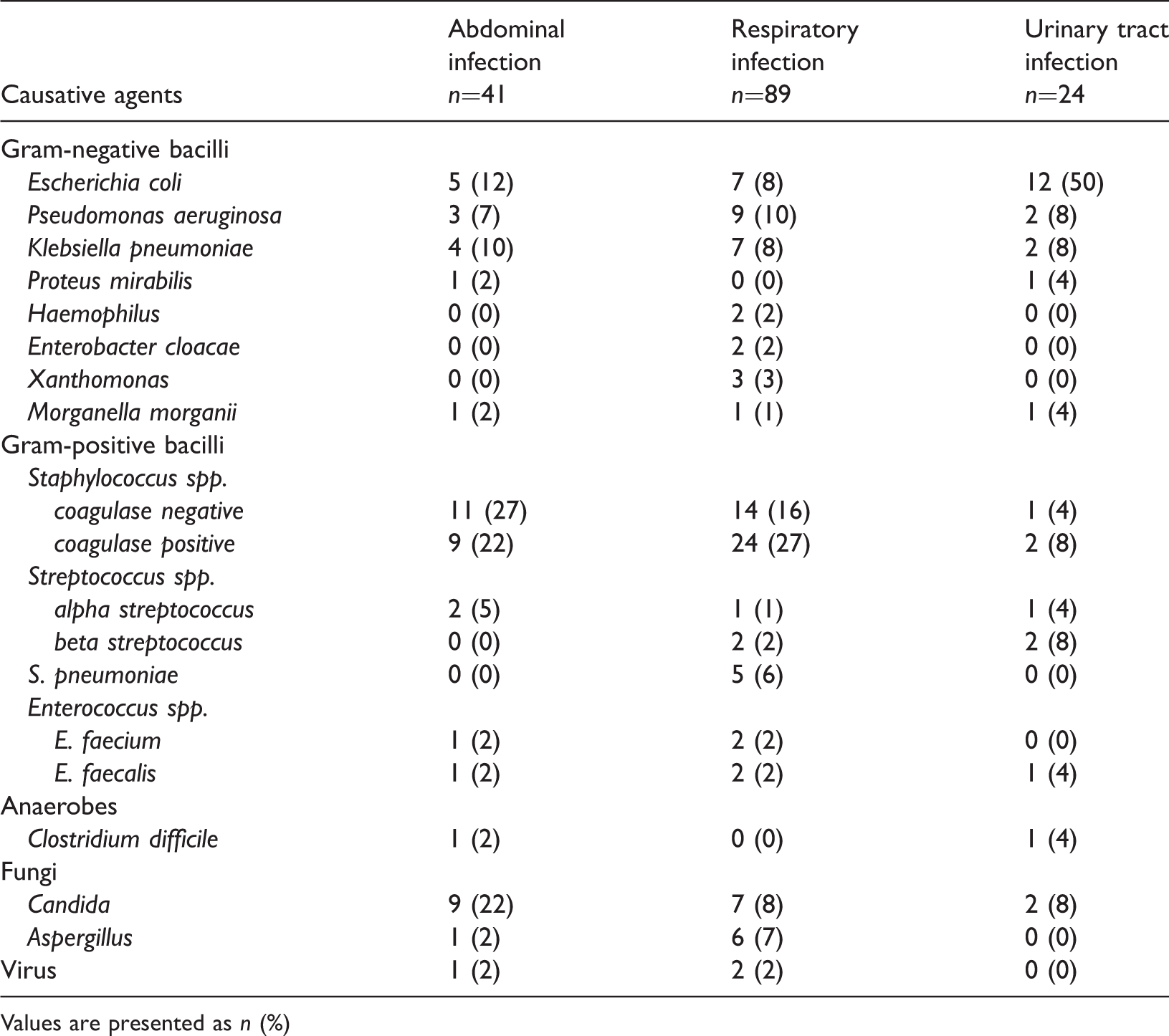
Values are presented as n (%)
Supportive therapy and outcomes of the 154 septic shock patients receiving high dose noradrenaline according to three primary infection sites.

Values are presented as n (%) or median (interquartile range)
ICU, intensive care unit; DNR, do not resuscitate; ns, not significant
The maximum dosage/duration of noradrenaline therapy, adequate antimicrobial therapy, length of stay in ICU/hospital and DNR rates were comparable among the three infection groups (Table 4). However, the 28- and 90-day mortalities were statistically significantly different among the groups (P=0.009) (Table 4). The 28-day mortality rates were 59%, 52% and 21% for the abdominal, respiratory and urinary tract infection groups, respectively. The 90-day mortality rates were 68%, 56% and 29% for the abdominal, respiratory and urinary tract infection groups, respectively.
A Cox proportional hazard model was used to assess the influence of significant risk factors identified using by the Wald χ2 test, on 28-day mortality. The factors were: age >60 years; SOFA score (Day 1); noradrenaline duration; adequate antimicrobial therapy; hypertension. As shown in Table 5, only SOFA scores on Day 1 were statistically significantly associated with increased 28-day mortality (P <0.001). Compared with the urinary infection group, the respiratory and abdominal infection groups were associated with higher risk of death (P =0.023 and P =0.015, respectively). Kaplan-Meier curve analyses were used to compare differences in 28-day survival between the three infection sites (Figure 2). There was no statistically significant difference between the abdominal and respiratory infection groups (Log Rank=0.9) but compared with the urinary infection group, the abdominal infection group (Log Rank=7.7, P =0.006) and the respiratory infection group (Log Rank=5.9, P =0.015) were significantly associated with 28-day mortality.
Risk factors for 28- day mortality based on multivariable Cox regression analysis.

SOFA, Sequential Organ Failure Assessment; ns, not significant
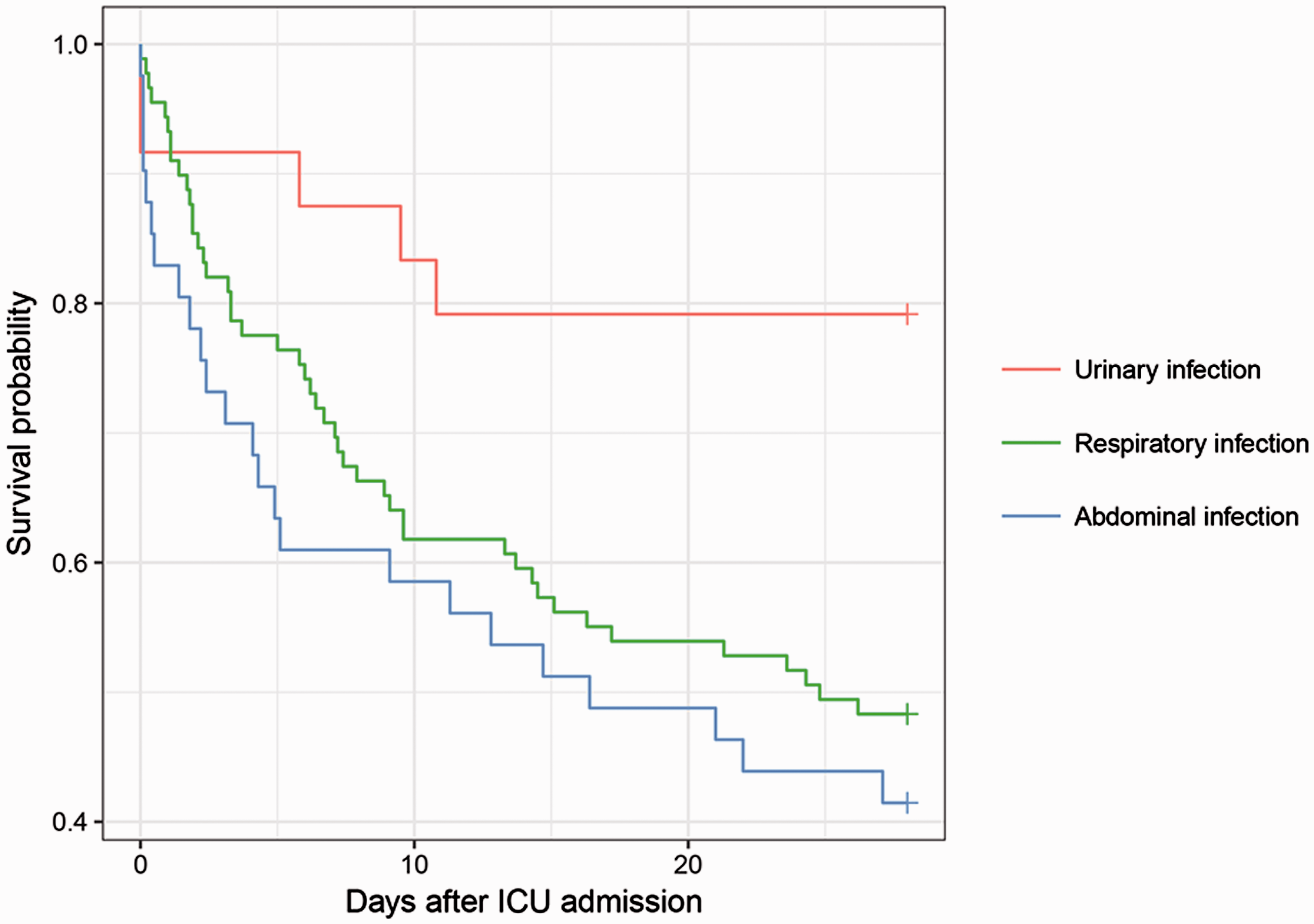
Kaplan-Meier survival curve analysis of septic shock patients receiving high doses of noradrenaline according to three primary infection sites. The 28-day survival was comparable between abdominal and respiratory infection population (Log Rank = 0.9). However, compared with the urinary infection group, the abdominal infection group (Log Rank=7.7, P = 0.006) and the respiratory infection group (Log Rank=5.9, P = 0.015) were significantly associated with 28-day mortality.
Discussion
Refractory shock can occur even after aggressive fluid resuscitation and so high dose vasopressors maybe required in patients with septic shock to maintain organ perfusion. However, high dose vasopressor therapy has been associated with unfavourable outcomes. For example, one study found that the likelihood of survival in ICU was minimal when patients received more than 0.5μg/kg per min of noradrenaline or adrenaline. 4 In another study in critically ill patients, noradrenaline ≥ 0.9 μg/kg per min was associated with a 28-day mortality rate of 65%. 3 In patients with sepsis who received ≥ 1 μg/kg per min of noradrenaline, a retrospective analysis of data from 433 patients found a mortality rate of 83%. 11 In addition, it is unclear if the source of the infection has an impact on the outcome of septic shock patients receiving high dose norepinephrine.
This retrospective study of data from a publicly available ICU database (MIMIC-III) which contained information from 46,520 critically ill patients admitted to a single centre in the USA,9 included 154 patients with septic shock who had received high dose (≥1 ug/kg per min) noradrenaline. In this cohort of patients, infections of the respiratory tract were the most common source of infection (58%), followed by abdominal (27%) and urinary (16%) infections. These findings are in agreement with those from a large international study where respiratory infections in the ICU were the most common (64%) while infections originating in the abdomen or renal/urinary tract accounted for 20% and 14%, respectively. 15
We found that the abdominal and respiratory infection groups recorded the largest number of deaths, almost twice as many as the urinary infection group. Analysis showed that by comparison with infections originating from the urinary tract, infections of an abdominal or respiratory origin were significantly associated with 28-day mortality in this cohort of patients. These findings are consistent with results from previous studies that have shown urinary infections were less severe and associated with better outcomes in patients with septic shock compared with respiratory, and abdominal infections.15,16 In our opinion, the lower risk of mortality may reflect the relative straightforward approach to source control for many patients with urinary infection compared with other infections.
In this present study, patients in the abdominal infection group had the highest SAPS II scores and 28- and 90-day mortality rates compared with the other patient groups. In addition, we observed that the incidence of secondary bacteraemia in the abdominal infection group was twice that of the other infection groups. These findings are consistent with previous studies.16,17 One possible explanation for these observations is that abdominal infections are typically polymicrobial. 18 We are of the opinion that bloodstream infections secondary to abdominal infections tend to result in multidrug resistance and pose a challenge for antibiotic therapy. For example, although mortality rates of 6–11% have been recorded following abdominal infection,19,20 after the infection has progressed to septic shock, the risk of death increases dramatically. 21 One study found that the 7-day mortality of patients with pyelonephritis and septic shock was 26% while those without septic shock was zero. 22
Our study showed that high SOFA scores on Day 1 were associated with increased risk of death. A strong correlation between vasopressor dose and SOFA scores has been observed previously. 10 These investigators also found that the interaction between SOFA score >10 and dose of noradrenaline >0.75 μg/kg per min was associated with an increasing 28-day mortality. Nevertheless, we found no differences between the three infection groups in the duration/maximum dosage of noradrenaline, length of stay in the ICU/hospital, DNR rates, hypertension and adequate antimicrobial therapy. Interestingly, a large proportion of patients were receiving adequate antimicrobial treatment which appeared to have little impact on their survival. It has been suggested that prolonged infections may be more a reflection of host immune activity rather than an indication of the presence of viable microorganisms. 23 However, further studies are required to determine if influencing factors, such as adequate/inadequate antimicrobial therapy are associated with outcomes in septic shock patients since in this study only approximately 15% of patients were receiving inadequate antibiotic treatment.
The study had several limitations. For example, it was a retrospective analysis of data from a single centre in the USA and so the evaluation may have been influenced by numerous biases. In addition, because the sample size was small and the positive culture rate was low, the association between microbiologic characteristics of the source infections and patients’ outcome could not be established. Finally, the exact causes of death for this cohort of patients were not evaluated.
In summary, we found that septic shock patients receiving noradrenaline ≥1 ug/kg per min had a poor prognosis. Duration/maximum dosage of noradrenaline, length of stay in the ICU/hospital, DNR rates, hypertension and adequate antimicrobial therapy were similar among the three different primary infection groups. However, patients with urinary infections had a lower risk of death at 28-days compared with those who had abdominal or respiratory infections. Given this heterogeneity, future studies should subgroup septic shock patients according to primary infection sites rather than group them as a whole. 7
Footnotes
Declaration of conflicting interests
The authors declare that there were no conflicts of interest.
Funding
The study was supported by Medical Scientific Research Foundation of Zhejiang province, China (No. 2016KYB155) and Zhejiang Provincial Natural Science Foundation of China (No. LY16H150004).