
Abstract
Objective
In this retrospective study, a modified measurement method was used to analyze cage migration during follow-up after unilateral instrumented transforaminal lumbar interbody fusion (TLIF) and identify associated factors.
Methods
We retrospectively evaluated 75 patients who had been treated with unilateral instrumented TLIF. Cage migration was quantitatively defined as anterior–posterior or lateral displacement of the cage.
Results
Five patients had significant cage migration (6.7%), but none developed severe neural symptoms during follow-up or underwent reoperation. The cages tended to migrate posteriorly or toward the side of surgery. The initial cage position and patient age were strongly associated with migration. Migration was less frequent when the cages were initially placed closer to the side of surgery. Patients of advanced age were more likely to develop anterior–posterior migration than were young patients.
Conclusion
Cage migration is related to the initial position of the cage. Particular attention is required when performing unilateral instrumented TLIF in patients of advanced age because they are most likely to develop cage migration. Quantification of cage migration is an effective method of exploring the associated factors.
Keywords
Introduction
With the increasing prevalence of a sedentary lifestyle among the aging population, it is unsurprising that growing numbers of people are developing degenerative lumbar diseases. Lumbar interbody fusion is a standard procedure with which to relieve these patients’ symptoms and improve their quality of life. Initially developed by Harms and Jeszenszky 1 in the 1990s, transforaminal lumbar interbody fusion (TLIF) has become a popular procedure for patients with degenerative lumbar diseases because it is safe, effective, and less invasive than other treatments. 2 Although unilateral instrumented TLIF is less invasive than traditional TLIF, upon which it is based, it has similar clinical outcomes and complication rates.3–6 Thus, it is a well-accepted surgical technique for the treatment of degenerative lumbar diseases.
However, some controversies remain regarding the use of unilateral instrumented TLIF. One is the increased cage migration rate. Cage migration is usually diagnosed as movement of the cage that exceeds 3 mm or extends beyond the wall of the vertebral body.7,8 Cage migration can be further classified as posterior, anterior, or lateral according to the direction in which the cage migrates. The cage can also slide either forward into the retroperitoneum or backward into the vertebral canal, causing failure of fusion or compression of the nerve roots and dura mater. Aoki et al. 9 and Duncan and Bailey 10 noted that cage migration occurs more commonly in patients treated with unilateral than bilateral fixation. However, several meta-analyses have shown that this difference is not statistically significant.5,6 Our previous study of 139 patients treated with unilateral instrumented TLIF showed a cage migration rate of 5.9%, 2 which is almost identical to the migration rates reported in other studies of bilateral instrumented TLIF. Thus, the available data on cage migration after unilateral instrumented TLIF are still insufficient to either finalize an accurate migration rate or identify the risk factors involved. Moreover, because a large degree of cage movement is rare, sizable samples are required for prospective or retrospective studies to ensure statistically significant results. Therefore, the present study is unique in that we used a modified measurement method to convert the variables tested into continuous variables and to measure cage migration during follow-up to analyze cage migration and identify the related factors.
Materials and methods
Patient selection
All patients included in this study had single-level (L4/5 or L5/S1) lumbar degenerative disc disease or spondylolisthesis and were treated by single-level unilateral instrumented TLIF with kidney-shaped polyetheretherketone (PEEK) cages by a single doctor from 2009 to 2014. All patients provided written informed consent, and ethical approval for the study was granted by the institutional review board. Before undergoing surgery, all patients were treated conservatively for at least 6 months. Patients were excluded if they had previously undergone spinal instrumentation and/or fusion. Only patients who underwent three complete follow-up examinations at 2 to 3 days, 2 to 3 months, and ≥6 months postoperatively were included in the study. The baseline analysis showed no significant differences between the patients in the final sample and the total initial sample (Table 1), indicating that the smaller sample was representative of the whole initial population.
Baseline level analysis.

A p value of <0.05 was accepted as significant.
All of the included patients were examined preoperatively and followed up with anterior–posterior (AP) and neutral lateral X-rays taken in a standing position.
Two types of variables were analyzed: demographic variables (age, sex, preoperative diagnosis, level of fusion, cage type, and cage size) and radiographic variables (disc height and cage position).
Surgical technique
All operations were performed by one senior doctor. The patients were placed in the prone position on a radiolucent operating table. Under fluoroscopic guidance with a C-arm X-ray system, the appropriate surgical level was marked and a lateral incision was made on the symptomatic side, 2 to 3 cm from the midline. The sacrospinalis muscle was split to expose the facet, transverse processes, and vertebral lamina, and two pedicle screws were then inserted through the vertebral pedicles. Consistent with standard TLIF, the facet joint and part of the vertebral lamina were removed with a high-speed drill, osteotome, and Kerrison rongeur; the disc was then exposed as for standard TLIF. The bone graft material was a mixture of autologous bone from the lamina and facet joint and contained 3- to 5-mm sections stripped of all the soft tissue attachments and decorticated. The disc and endplate cartilage were completely and carefully removed to ensure that the subchondral bone was not violated. If the patient developed symptoms of bilateral nerve root compression, the contralateral side was decompressed by resecting the contralateral ligamentum flavum and osteophyte through the same incision. A kidney-shaped cage was inserted into the intervertebral space and filled with autologous bone. Finally, a pre-bent rod was placed and locked. A drain was inserted and the incision was closed. All patients were required to start ambulation early, at 2 to 3 days after surgery, and to wear a brace during ambulation for 8 weeks after surgery.
Radiographic assessment
Plain radiographs of the lumbar spine were obtained four times: preoperatively and at 2 to 3 days, 2 to 3 months, and ≥6 months postoperatively.
The anterior disc height was defined as the vertical distance between the anterior edge of the inferior endplate of the superior surgery body and the anterior edge of the superior endplate of the inferior surgery body. The posterior disc height was defined as the vertical distance between the posterior edge of the inferior endplate of the superior surgery body and the posterior edge of the superior endplate of the inferior surgery body. The mean disc height (MDH) was the mean of the anterior disc height and posterior disc height. The value obtained by subtracting the preoperative MDH from the cage size was defined as “cage size − preMDH.” The value obtained by subtracting the postoperative MDH from the cage size was defined as “cage size − postMDH.”
The cage position was identified in terms of its AP position and lateral position, as shown in Figure 1. The AP position was defined as the ratio of the distance between the anterior margin of the inferior endplate of the superior surgery body and the center of the cage to the whole AP length of this endplate (i.e., the distance between the anterior margin of the inferior endplate of the superior surgery body and the center of the cage/the whole AP length of this endplate). The lateral position was defined as the ratio of the distance between the contralateral margin of the endplate of the instrumented side and the center of the cage to the least lateral length of the superior fusion body. A smaller AP ratio indicated a more anterior position on the sagittal plane, and a smaller lateral ratio indicated a greater distance from the instrumented side on the coronal plane. The initial position of the cage was measured at the first follow-up and modified by the difference between the measured center and the original center according to the inclination angle of the cage. Cage migration was defined as a change in the position of the cage during follow-up on the AP or lateral X-ray. If the cage shifted in the anterior direction or toward the noninstrumented side, the migration was given a negative number. Likewise, if the cage shifted in the posterior direction or toward the instrumented side, the migration was given a positive number. Therefore, movements could differ in direction although their absolute distances were the same. All measurements were made by one of the authors.
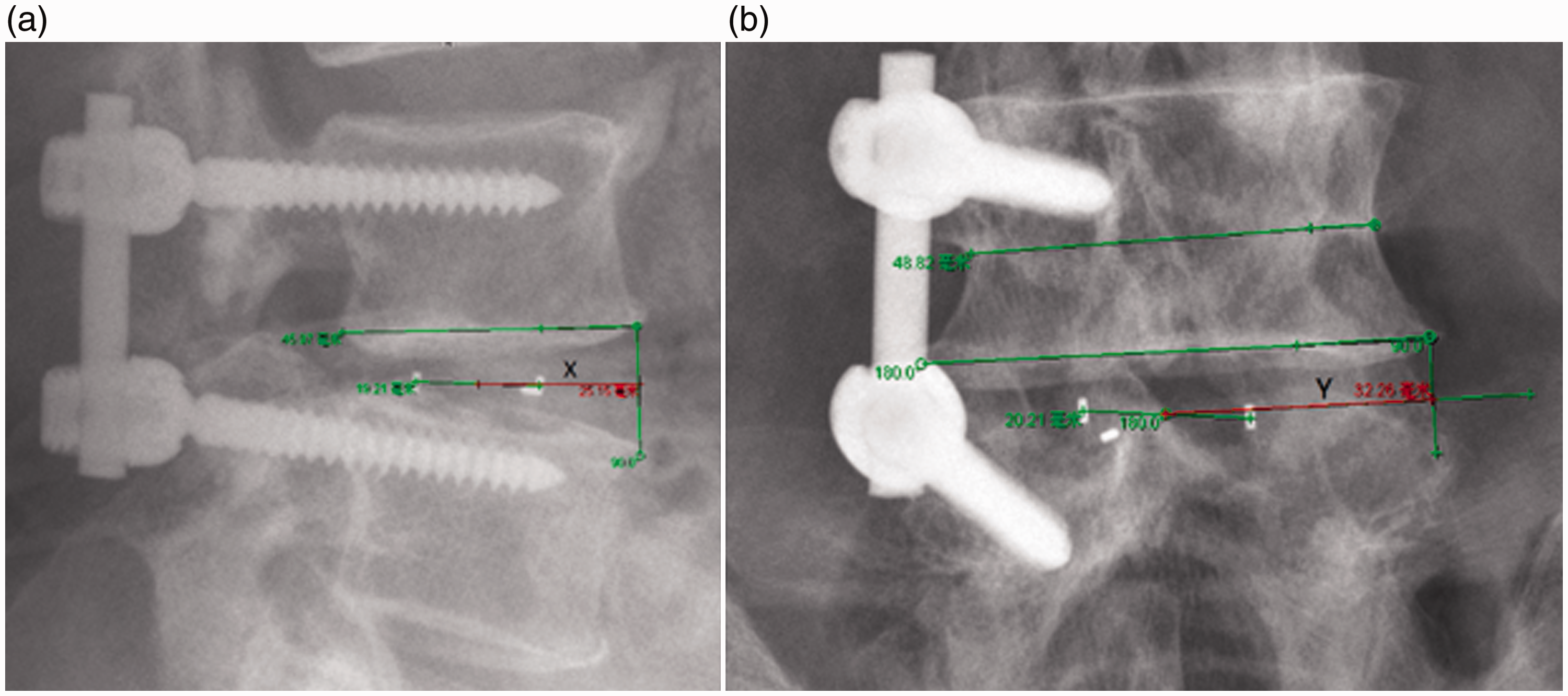
Cage position measurement in anterior–posterior (AP) position and lateral position. (a) The AP position was defined as the ratio of the distance between the anterior margin of the inferior endplate of the superior surgery body and the center of the cage to the whole AP length of this endplate. (b) The lateral position was defined as the ratio of the distance between the contralateral margin of the endplate of the instrumented side and the center of the cage to the least lateral length of the superior fusion body.
To determine the intraobserver consistency, 30 patients were randomly selected and their data were collected again by the same researcher 1 month after the first data collection. To determine the interobserver consistency, the data for these patients were also collected by another two pretrained researchers using the same process.
Statistical analysis
Data were analyzed with the SPSS 20.0 software package (IBM Corp., Armonk, NY, USA). Descriptive statistics are summarized as frequency and percentage for categorical variables and as mean ± standard deviation for continuous variables. The preoperative and postoperative indices were compared with a paired t test, Pillai’s trace, and repeated-measures analysis of variance. The initial position of the cage, disc height, age, sex, and other parameters were analyzed with a general estimating equation to identify the possible risk factors for cage migration. A p value of <0.05 was considered statistically significant.
Results
Demographic variables
Of 249 patients who met the inclusion criteria, only 75 patients underwent three complete follow-up examinations (at 2–3 days, 2–3 months, and ≥6 months postoperatively) and were therefore included in the study. These 75 patients comprised 30 men and 45 women with a mean age of 57.4 years (range, 34–79 years); 55 patients had a diagnosis of spinal stenosis and 20 had a diagnosis of spondylolisthesis. Fifty-three cages were inserted at the L4.5 level and 22 at the L5.S1 level. All were kidney-shaped PEEK cages made by three manufacturers (Johnson & Johnson, Le Locle, Switzerland; LDR, Sainte-Savine, France; and Stryker, Cestas, France) and varied in size from 7 to 15 mm. The median periods to the three follow-up examinations were 2, 64, and 219 days. The results are presented in Table 2.
Radiographic assessment
Five patients developed significant cage migration (6.7%), but none experienced severe neural symptoms during follow-up or underwent reoperation. The initial position of all cages was marked as (X0, Y0) according to the initially measured AP and lateral position, respectively. The mean X0 was 0.457 ± 0.083 (0.252, 0.623), and the mean Y0 was 0.635 ± 0.091 (0.389, 0.826). During follow-up, the cages tended to migrate posteriorly and toward the operative side. A paired t test and Pillai’s trace showed significant changes in the cage positions at each follow-up (Table 3). The rate of ≥3-mm cage subsidence was 17.9% (14 cages) at the long-term follow-up.
Patients’ demographic variables.

SD, standard deviation; P25, 25th percentile; P75, 75th percentile. Min, minimum; Max, maximum.
To explore the risk factors for cage migration, a general estimating equation was applied to the repeatedly measured data and revealed that AP migration was related only to age. Patients of advanced age developed more cage migration in the AP position than did younger patients (p = 0.038) (Table 4). We examined the relationship between AP migration and age and found that AP migration was more frequent in patients aged >70 years than in younger patients.
Cage positions during follow-up.

Data are presented as mean ± standard deviation; P<0.05 was accepted as significant.
AP, anterior–posterior.
Risk factors for anterior–posterior migration.

A p value of <0.05 was accepted as significant.
preMDH, preoperative mean disc height; postMDH, postoperative mean disc height.
Risk factors for lateral migration.

A p value of <0.05 was accepted as significant.
preMDH, preoperative mean disc height; postMDH, postoperative mean disc height.
Lateral migration was related to the initial lateral position of the cage (B = −0.219, p = 0.009). When the cage was placed closer to the operative side (i.e., farther from the nonoperative side), less migration occurred. The results are presented in Table 5.
Intraobserver and interobserver reliability
The kappa value for intraobserver agreement regarding measurement of the AP position of the cage was 0.997, and that regarding measurement of the lateral position was 0.929. For interobserver agreement, these kappa values were 0.994 and 0.906, respectively. Thus, all measurements showed excellent agreement.
Discussion
To accommodate the limited samples available for analysis, a classification standard was used to convert the variables tested into continuous variables. To our knowledge, no published clinical study of cage migration and its risk factors has been conducted in this way. In this study, we showed that the cages tended to migrate posteriorly or toward the operative side; this might have been caused by the pressure exerted on the disc remnants on the anterior or contralateral side. Traditional studies have also shown that cage migration almost always occurs in a posterior direction,9,11 which supports the accuracy of our method.
Our study showed that age was a significant risk factor for cage migration because patients of advanced age developed more AP migration, especially those older than 70 years. We presume that older patients have more highly unstable segments. The low bone mineral density (BMD) of older patients may also make the pedicle screw unstable. A previous study showed the same result; i.e., that older age is a risk factor for cage retropulsion. 12 Another study revealed that lower BMD can result in cage migration. 7 However, this is still only a hypothesis because BMD was not measured in all of the patients in our study. BMD is usually more strongly associated with subsidence. In our study, the rate of ≥3-mm cage subsidence was 17.9% (14 cages) at the long-term follow-up. In 2008, Schleicher et al. 13 found that TLIF with unilateral pedicle screw fixation was significantly less stable than TLIF with bilateral fixation, particularly in terms of lateral bending and rotation. Therefore, unilateral instrumented TLIF should be performed with caution in patients of advanced age. It may be beneficial to measure the BMD of patients, especially older ones, and to administer anti-osteoporosis drugs to those with osteoporosis. However, further studies are required to determine whether this would reduce the rate of cage migration.
Because the operative window is limited and the cage itself is relatively small, TLIF seems more susceptible to problems of cage position than does posterior lumbar interbody fusion. However, whether the cage position is related to its migration remains controversial. Some studies have shown that anterior positioning confers better sagittal balance 14 but more subsidence, whereas posterior positioning confers better stability. 15 A previous study showed no relationship between the initial position of the cage and cage migration, 9 whereas other research has shown that cages in a mediomedial position have a greater tendency to migrate after posterior lumbar interbody fusion than those in a posterolateral or posteromedial position. 16 In the present study, however, the initial position of the cage was unrelated to AP migration; instead, it was associated with lateral migration. Less migration occurred when the cage was placed in a position closer to the operative side, which is probably attributable to the pressure squeezing reaction and stress shielding reaction of the fixation system. In our clinical practice, we tend to place the cage near the middle of the lumbar region, slightly ahead of and away from the operated side. Therefore, the position of the cage is centered, which may reduce the rate of migration. It is commonly reported in retrospective studies that the position of the cage is not chosen randomly but instead according to the surgeon’s operative habit. Therefore, we presume that the influence of the initial cage position on its migration is underestimated.
The type and size of cage did not greatly affect its migration, perhaps because our choice of cage was appropriate. All cages were kidney-shaped and of the most suitable size. Although a bullet-shaped fusion cage can be more easily inserted into a suitable position, fitting well with the concave surface of the normal endplate, 11 several studies have shown that the use of a bullet-shaped cage is a possible risk factor for cage migration.7–9,17 PEEK is now widely used as the cage material because it offers radiolucency and good fusion and enhances the elastic modulus.18,19 Therefore, to minimize the influence of the shape and material of the cage on migration, we only included patients who were treated with kidney-shaped PEEK cages in the present study.
The major problem of migration is that it causes nonfusion and compression of the nerve roots and dura mater. Of the five patients with significant cage migration, none developed severe neural symptoms during follow-up or required reoperation. We did not collect all relevant data on cage fusion and clinical outcomes because the time assigned for the follow-ups was limited. Further studies are required to investigate the relationships among migration, fusion, and clinical outcomes over a longer follow-up period.
In conclusion, five patients developed significant cage migration (6.7%), but none experienced severe neural symptoms during follow-up or required reoperation. The cages tended to migrate posteriorly or toward the operative side, and less migration occurred when we initially placed the cage closer to the surgical side. Particular attention must be paid when choosing unilateral instrumented TLIF for patients of advanced age because they are more likely to develop cage migration than younger patients. We propose that this modified method, which includes repeated measurements, is an effective way to analyze cage migration and its risk factors.
Footnotes
Declaration of conflicting interest
The author(s) declare that there is no conflict of interest.
Funding
This work was supported by the National Natural Science Foundation of China, Youth (81801375), and the Medical Guidance Support Project of Shanghai Science and Technology Committee (16411964200).