
Abstract
Hyperglobulinemia is a common manifestation of plasma cell disease, and it is sometimes caused by autoimmune diseases (AIDs). We report an uncommon presentation of hyperglobulinemia, with a high amount of plasma cells in bone marrow, pancytopenia, hematemesis, and splenomegaly in an 18-year-old woman. Some examinations were performed to determine the diagnosis, including serum protein electrophoresis, immunofixation electrophoresis, the free light chain assay, abdominal enhanced computed tomography (CT) and CT venography, and positron-emission tomography-CT. The patient was finally diagnosed with AID. Considerable improvement in her symptoms was observed after immunosuppressive therapy. Findings in this case highlight that not only differentiation of hyperglobulinemia caused by monoclonal or polyclonal immunoglobulin, but also AIDs, need to be considered to exclude non-Hodgkin’s lymphoma and plasma cell disease.
Keywords
Introduction
Hyperglobulinemia is usually caused by monoclonal immunoglobulin, which is produced by malignant plasma cells, or by polyclonal immunoglobulin, caused by autoimmune diseases (AIDs).1,2 We report a complex case with presentation of hyperglobulinemia, increased plasma cells in the bone marrow, pancytopenia, hematemesis, and an enlarged spleen.
Case report
An 18-year-old woman presented with fever and hematemesis for 1 week. She had no previous medical history. She had a fever with a temperature of 38°C, she was not chilly, there was no arthralgia, and she presented with hematemesis (approximately 20 mL). Furthermore, there was no abdominal pain or diarrhea. A clinical examination showed a pale appearance, an enlarged spleen 5 cm below the ribs, and no enlarged lymph nodes or liver were found. Her laboratory examinations showed the following: white blood cell count, 1.64 × 109/L; hemoglobin level, 59 g/L; platelet count, 60 × 109/L; alanine aminotransferase level, 48U/L; aspartate aminotransferase level, 49U/L; globulin, 72 g/L; β2-microglobulin, 3.08 µmol/L; prothrombin time, 19.1 seconds; international normalized ratio, 1.72; activated partial thromboplastin time, 53.6 seconds; and fibrinogen, 0.98 g/L. Folic acid, vitamin B12, and ferritin levels were normal. A bone marrow smear showed hypercellularity with 17% mature plasma cells. Transabdominal ultrasound showed an enlarged spleen, a small amount of ascites, and splenic vein dilatation.
After admission, more examinations were performed to clarify the diagnosis. We found a positive result for serum protein electrophoresis and a negative result for immunofixation electrophoresis (Figure 1). A free light chain examination showed that κ and λfree were 388 mg/L and 299 mg/L, respectively, with a ratio of 1.30. CD59 and fluorochrome-labeled aerolysin examinations are normal. A bone marrow smear (illum) showed hypercellularity with 15% mature plasma cells (Figure 2a). A bone marrow biopsy showed dispersed plasma cells without light chain restrictive expression. Flow cytometry showed normal plasma cells with polyclonal immunoglobulin (Figure 2b). We found that the immunoglobulin G level was 6780 mg/dL, the complement (C) 3 level was 40.10 mg/dL, and the C4 level was 13.30 mg/dL. Antinuclear antibody was 1: 1600, the C1q level was 6.04 U/mL, anti-Sjogren’s syndrome A, anti-Sjogren’s syndrome B, anti-Ro 52, and rheumatoid factor were all positive, and double-stranded DNA antibody and anti-cardiolipin antibody were negative. An X-ray of the bone was negative. Abdominal enhanced computed tomography (CT) and CT venography showed splenic vein thrombosis, splenomegaly, portal hypertension, esophageal and gastric varices, mesenteric edema and multiple lymph node enlargement, and abdominal and pelvic effusion (Figure 3). Positron-emission tomography-CT showed that the maximum standardized uptake (SUVmax) was 2.7 in the liver, there was splenomegaly with an SUVmax of 2.9, and the SUVmax was 7.3 in the bone marrow. Additionally, there were some small lymph nodes in the bilateral axillary, inguinal, and mediastinal areas without tracer concentration.
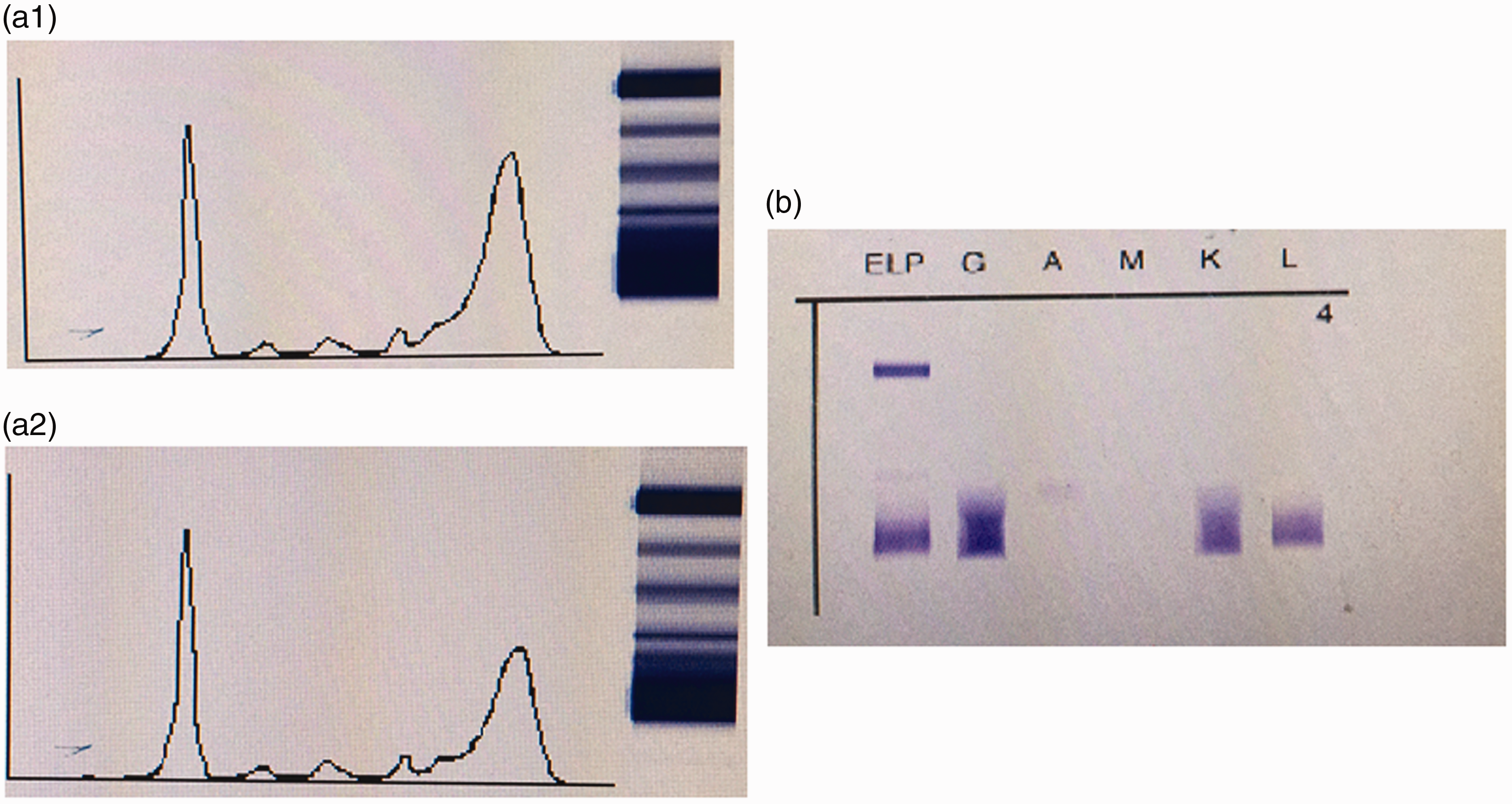
Serum protein electrophoresis and immunofixation electrophoresis. Serum protein electrophoresis was positive before (a1) and after treatment (a2), while immunofixation electrophoresis was negative at these times (b).
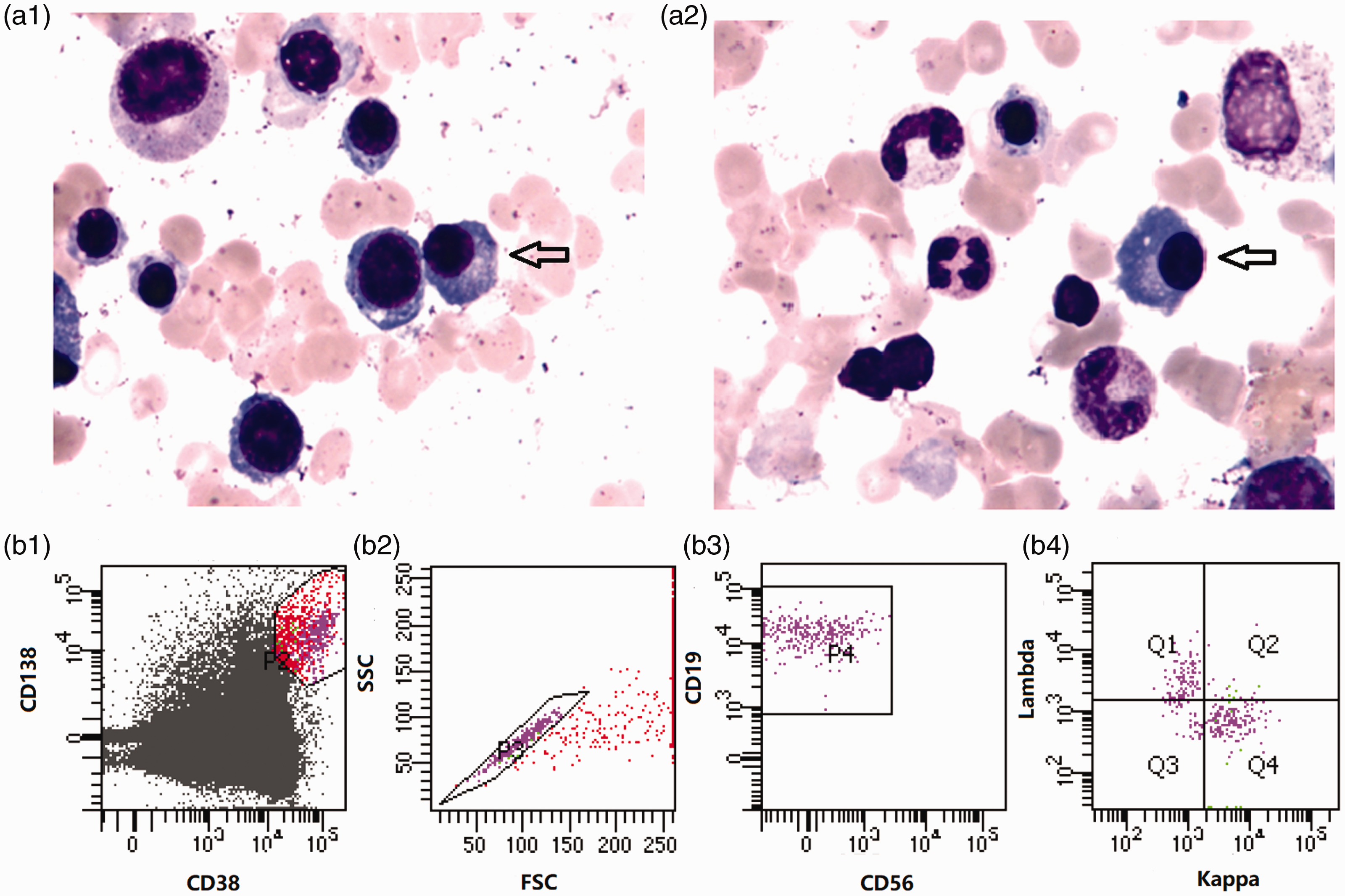
Bone marrow smear and immunophenotype examinations. A bone marrow smear shows plasma cells (black arrow) (a1, 2). An immunophenotype examination shows polyclonal plasma cells (b).

Abdominal enhanced computed tomography and computed tomography venography. Splenic vein thrombosis is shown by the red arrows.
The patient received hemostasis therapy and omeprazole immediately. She was then administered hydrocortisone 100 mg per day, erythropoietin 6000 U three times weekly, and thrombopoietin 15,000 U three times weekly for 2 weeks. A blood examination then showed that hemoglobin was 85 g/L, the platelet count was 115 × 109/L, the white blood cell count was 12.6 ×109/L, and globulin was 58 g/L, while autoantibodies were still positive. After consultation with the Immunology Department and Gastroenterology Department, the patient was diagnosed with AID, cirrhosis, hypersplenism, splenic vein thrombosis, upper gastrointestinal bleeding, dysfunction of blood coagulation, and pancytopenia. She was transferred to another department to receive gastric variceal ligation and splenectomy.
The study protocol was approved by the ethical committee of Tianjin Medical University General Hospital. The patient provided verbal informed consent.
Discussion
Monoclonal immunoglobulin is produced by malignant plasma cells, and it can be diagnosed by serum protein electrophoresis, serum immunofixation, and the free light chain assay.1–3 In our case, we found that hyperglobulinemia was polyclonal, and several autoantibodies were positive, including antinuclear antibody, anti-Sjogren’s syndrome A, anti-Sjogren’s syndrome B, and Ro-52, which support the diagnosis of Sjogren’s syndrome. Further examinations showed cirrhosis and hypersplenism, resulting from AID. While our patient had no dryness of the eyes or mouth, she did not meet the diagnostic criteria of Sjogren’s syndrome. 4 Finally, we diagnosed her with AID.
AIDs can predispose to non-Hodgkin’s lymphoma. Kleinstern et al. found that AID is an adverse prognostic factor in B-cell lymphoma, and is associated with a shorter time to relapse, especially in diffuse large B cell lymphoma. 5 Many studies have shown that patients with Sjogren’s syndrome have a higher risk of developing non-Hodgkin’s lymphoma compared with those with other AIDs. 6 Mucosa-associated lymphoid tissue lymphoma is the most common subtype associated with Sjogren’s syndrome. Several clinical manifestations, such as persistent enlargement of the salivary glands, lymphadenopathy,7,8 symptomatic cryoglobulinemic vasculitis, 9 and serological features, such as leukopenia, low C4 levels, and monoclonal gammopathy, 10 have been proposed as predictive for lymphoma. In our case, we found splenomegaly, leukopenia, and a low C4 level, which may be associated with lymphoma. Therefore, PET-CT was performed to search for evidence of lymphoma. Fortunately, we did not find any abnormal tracer concentrations. For this young patient, we consider that AID caused liver injury, as previously reported, 11 and then cirrhosis and hypersplenism occurred after a long time. Portal vein thrombosis and splenic vein thrombosis are common complications in cirrhosis mainly because of portal hypertension and dysfunction of blood coagulation. 12 In this situation, physicians are advised closely monitor patients for developing lymphoma, and if possible, a spleen biopsy is necessary.
Conclusion
Some AIDs are closely associated with B-cell lymphoma and plasma cell disorders. Physicians should be aware of this situation.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Tianjin Municipal Natural Science Foundation (Grant no. 18JCYBJC27200), Tianjin Health and Family Planning Commission (Grant no. 15KG150), and the Foundation of Tianjin Municipal Education Commission (2018KJ043).